Pulmonary Cryptococcosis: Imaging Findings in 23 Non-AIDS Patients
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea. kyungs.lee@samsung.com
- 2Division of Pulmonary and Critical Care Medicine at the Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- KMID: 984894
- DOI: http://doi.org/10.3348/kjr.2010.11.4.407
Abstract
OBJECTIVE
We aimed to review the patterns of lung abnormalities of pulmonary cryptococcosis on CT images, position emission tomography (PET) findings of the disease, and the response of lung abnormalities to the therapies in non-AIDS patients.
MATERIALS AND METHODS
We evaluated the initial CT (n = 23) and 18F-fluorodeoxyglucose (FDG) PET (n = 10), and follow-up (n = 23) imaging findings of pulmonary cryptococcosis in 23 non-AIDS patients. Lung lesions were classified into five patterns at CT: single nodular, multiple clustered nodular, multiple scattered nodular, mass-like, and bronchopneumonic patterns. The CT pattern analyses, PET findings, and therapeutic responses were recorded.
RESULTS
A clustered nodular pattern was the most prevalent and was observed in 10 (43%) patients. This pattern was followed by solitary pulmonary nodular (n = 4, 17%), scattered nodular (n = 3, 13%), bronchopneumonic (n = 2, 9%), and single mass (n = 1, 4%) patterns. On PET scans, six (60%) of 10 patients showed higher FDG uptake and four (40%) demonstrated lower FDG uptake than the mediastinal blood pool. With specific treatment of the disease, a complete clearance of lung abnormalities was noted in 15 patients, whereas a partial response was noted in seven patients. In one patient where treatment was not performed, the disease showed progression.
CONCLUSION
Pulmonary cryptococcosis most commonly appears as clustered nodules and is a slowly progressive and slowly resolving pulmonary infection. In two-thirds of patients, lung lesions show high FDG uptake, thus simulating a possible malignant condition.
Keyword
MeSH Terms
-
Adult
Aged
Contrast Media/diagnostic use
Cryptococcosis/*radiography/*radionuclide imaging/therapy
Disease Progression
Female
Fluorodeoxyglucose F18/diagnostic use
Follow-Up Studies
Humans
Lung Diseases, Fungal/*radiography/*radionuclide imaging/therapy
Male
Middle Aged
Positron-Emission Tomography/*methods
Radiopharmaceuticals/diagnostic use
Retrospective Studies
Tomography, Spiral Computed/*methods
Figure
-

Fig. 1 Pulmonary cryptococcosis with clustered nodular pattern in 53-year-old man who had hepatocellular carcinoma (patient 11 in Tables 1, 2). A. Lung window of transverse CT scan obtained at level of distal trachea demonstrates clustered nodules in posterior segment of right upper lobe. B. PET/CT scan obtained at similar level to A demonstrates high FDG uptake (arrow) within main nodule (maximum standardized uptake value, 9.3), hence simulating malignant nodule. C. Follow-up CT scan obtained at similar level to and three months after A demonstrates slightly increased extent of clustered nodules in right upper lobe.
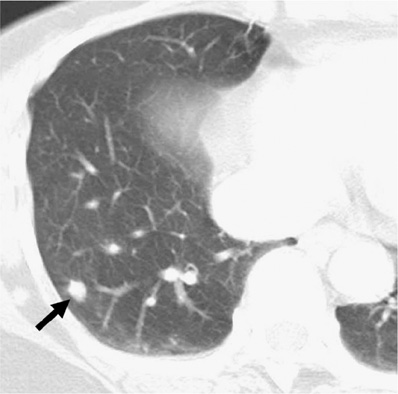
Fig. 2 Pulmonary cryptococcosis of solitary pulmonary nodular pattern in 58-year-old man who had esophageal cancer (patient 19 in Tables 1, 2). Lung window of transverse CT scan obtained at level of suprahepatic inferior vena cava shows 7-mm-sized solitary pulmonary nodule (arrow) in right lower lobe.
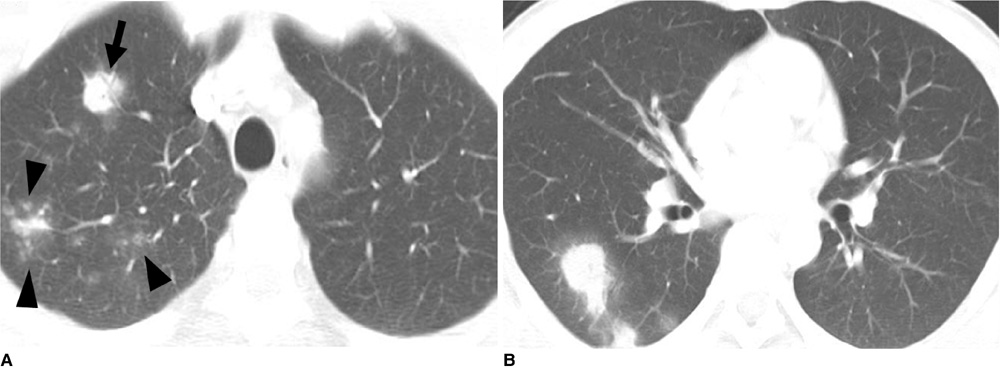
Fig. 3 Pulmonary cryptococcosis with scattered nodular pattern in 38-year-old man who had no underlying disease (patient 7 in Tables 1, 2). A. Lung window of transverse CT scan obtained at level of great vessels shows nodule (arrow) with surrounding ground-glass opacity (halo sign) and centrilobular small nodules (arrowheads) in right upper lobe. B. CT scan obtained at level of basal trunk demonstrates nodules with halo sign in superior segment of right lower lobe.
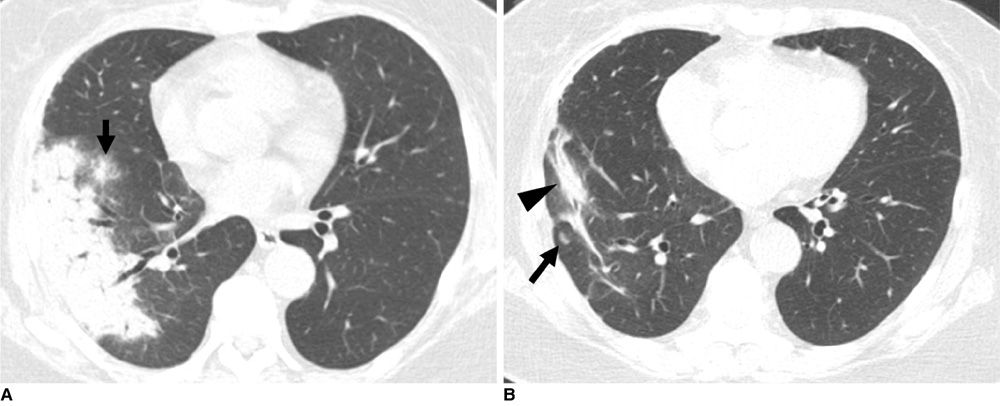
Fig. 4 Cryptococcosis of bronchopneumonic pattern in 72-year-old woman who has underlying breast cancer (patient 22 in Tables 1, 2). A. Lung window of transverse CT scan obtained at level of right inferior pulmonary vein shows subpleural consolidation and nodule (arrow) with surrounding halo in right lower lobe. B. Follow-up CT scan obtained five months after A and with four months of anti-fungal therapy demonstrates remaining lesions of consolidation (arrowhead) and nodule (arrow) in right lower lobe.

Fig. 5 Pulmonary cryptococcosis of solitary mass pattern in 52-year-old woman with no underlying disease (patient 8 in Tables 1, 2). Lung window of CT scan obtained at level of right middle lobar bronchus shows mass in right middle lobe.
Cited by 1 articles
-
Two Cases of Cryptococcuria Developed as Isolated Cryptococcuria and Disseminated Cryptococcosis
Mi Hyun Bae, Seung Namgoong, Dongheui An, Mi-Na Kim, Sung-Han Kim, Ki-Ho Park, Sung-Gyu Lee
Korean J Clin Microbiol. 2011;14(4):148-152. doi: 10.5145/KJCM.2011.14.4.148.
Reference
-
1. Sarosi GA. Cryptococcal pneumonia. Semin Respir Infect. 1997. 12:50–53.2. Woodring JH, Ciporkin G, Lee C, Worm B, Woolley S. Pulmonary cryptococcosis. Semin Roentgenol. 1996. 31:67–75.3. Levitz SM. The ecology of Cryptococcus neoformans and the epidemiology of cryptococcosis. Rev Infect Dis. 1991. 13:1163–1169.4. Miller WT Jr, Edelman JM, Miller WT. Cryptococcal pulmonary infection in patients with AIDS: radiographic appearance. Radiology. 1990. 175:725–728.5. Meyohas MC, Roux P, Bollens D, Chouaid C, Rozenbaum W, Meynard JL, et al. Pulmonary cryptococcosis: localized and disseminated infections in 27 patients with AIDS. Clin Infect Dis. 1995. 21:628–633.6. Friedman EP, Miller RF, Severn A, Williams IG, Shaw PJ. Cryptococcal pneumonia in patients with the acquired immunodeficiency syndrome. Clin Radiol. 1995. 50:756–760.7. Lacomis JM, Costello P, Vilchez R, Kusne S. The radiology of pulmonary cryptococcosis in a tertiary medical center. J Thorac Imaging. 2001. 16:139–148.8. Khoury MB, Godwin JD, Ravin CE, Gallis HA, Halvorsen RA, Putman CE. Thoracic cryptococcosis: immunologic competence and radiologic appearance. AJR Am J Roentgenol. 1984. 142:893–896.9. Zinck SE, Leung AN, Frost M, Berry GJ, Müller NL. Pulmonary cryptococcosis: CT and pathologic findings. J Comput Assist Tomogr. 2002. 26:330–334.10. Fox DL, Müller NL. Pulmonary cryptococcosis in immunocompetent patients: CT findings in 12 patients. AJR Am J Roentgenol. 2005. 185:622–626.11. Lindell RM, Hartman TE, Nadrous HF, Ryu JH. Pulmonary cryptococcosis: CT findings in immunocompetent patients. Radiology. 2005. 236:326–331.12. Aberg JA, Mundy LM, Powderly WG. Pulmonary cryptococcosis in patients without HIV infection. Chest. 1999. 115:734–740.13. Nadrous HF, Antonios VS, Terrell CL, Ryu JH. Pulmonary cryptococcosis in nonimmunocompromised patients. Chest. 2003. 124:2143–2147.14. Huang CJ, You DL, Lee PI, Hsu LH, Liu CC, Shih CS, et al. Characteristics of integrated 18F-FDG PET/CT in pulmonary cryptococcosis. Acta Radiol. 2009. 50:374–378.15. Vinson AE, Solis V, Williams HT, Bell B. F-18-FDG-PET/CT leads to diagnosis of cryptococcal pneumonia where recurrent metastatic rhabdomyosarcoma was suspected. Clin Nucl Med. 2007. 32:401–403.16. Igai H, Gotoh M, Yokomise H. Computed tomography (CT) and positron emission tomography with [18f]fluoro-2-deoxy-D-glucose (FDG-PET) images of pulmonary cryptococcosis mimicking lung cancer. Eur J Cardiothorac Surg. 2006. 30:837–839.17. Hsu CH, Lee CM, Wang FC, Lin YH. F-18 fluorodeoxyglucose positron emission tomography in pulmonary cryptococcoma. Clin Nucl Med. 2003. 28:791–793.18. Webb WR, Muller NL, Naidich DP. High-resolution CT of the lung. 2009. 4th ed. Philadelphia: Lippincott Williams & Wilkins, PA.19. Shim SS, Lee KS, Kim BT, Chung MJ, Lee EJ, Han J, et al. Non-small cell lung cancer: prospective comparison of integrated FDG PET/CT and CT alone for preoperative staging. Radiology. 2005. 246:1011–1019.20. Kim YK, Lee KS, Kim BT, Choi JY, Kim H, Kwon OJ, et al. Mediastinal nodal staging of nonsmall cell lung cancer using integrated 18F-FDG PET/CT in a tuberculosis-endemic country: diagnostic efficacy in 674 patients. Cancer. 2007. 109:1068–1077.21. Chang WC, Tzao C, Hsu HH, Lee SC, Huang KL, Tung HJ, et al. Pulmonary cryptococcosis: comparison of clinical and radiographic characteristics in immunocompetent and immunocompromised patients. Chest. 2006. 129:333–340.22. Shim SS, Lee KS, Kim BT, Choi JY, Chung MJ, Lee EJ. Focal parenchymal lung lesions showing a potential of false-positive and false-negative interpretations on integrated PET/CT. AJR Am J Roentgenol. 2006. 186:639–648.23. Cheon JE, Im JG, Kim MY, Lee JS, Choi GM, Yeon KM. Thoracic actinomycosis: CT findings. Radiology. 1998. 209:229–233.24. Aquino SL, Kee ST, Warnock ML, Gamsu G. Pulmonary aspergillosis: imaging findings with pathologic correlation. AJR Am J Roentgenol. 1994. 163:811–815.25. Kim SY, Lee KS, Han J, Kim J, Kim TS, Choo SW, et al. Semiinvasive pulmonary aspergillosis: CT and pathologic findings in six patients. AJR Am J Roentgenol. 2000. 174:795–798.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Various Pulmonary Manifestations of the Cryptococcal Pneumoniae in the three Immunocompetent Patients
- A Case of Pulmonary Cryptococcosis Followed by Pulmonary Tuberculosis Developed after Bilateral Adrenalectomy
- An Autopsy Case of the AIDS Presented with Disseminated Cryptococcosis
- Clinicoradiological Features of Pulmonary Cryptococcosis in Immunocompetent Patients
- Massive Mediastinal Lymph Node Involvement of Cryptococcosis in Immunocompetent Host
