Korean J Ophthalmol.
2010 Aug;24(4):249-251. 10.3341/kjo.2010.24.4.249.
A Case of Bilateral Endogenous Pantoea Agglomerans Endophthalmitis with Interstitial Lung Disease
- Affiliations
-
- 1Department of Ophthalmology, Dongguk University College of Medicine, Gyeongju, Korea. ophho@hanmail.net
- 2Department of Clinical Pathology, Dongguk University College of Medicine, Gyeongju, Korea.
- KMID: 949065
- DOI: http://doi.org/10.3341/kjo.2010.24.4.249
Abstract
- We here in report a case of bilateral endogenous endophthalmitis caused by Pantoea agglomerans (P. agglomerans) in a patient who had interstitial lung disease and was treated with oral corticosteroids. A 72-year-old man presented with decreased visual acuity in both eyes nine days after he received oral corticosteroids. He had marked uveitis, cataracts, and vitreous opacities. Cultures were taken of blood, aqueous humor, and vitreous. We initially suspected a fungal etiology and treated him with antifungal drugs; however, the intraocular disease progressed without improvement. Vitreous culture was positive for P. agglomerans. The patient underwent pars plana vitrectomy with cataract surgery bilaterally, followed by a 2-week course of antibiotics. The final visual acuity was 20/25 in the right eye and 20/200 in the left eye. This is the first report of bilateral endogenous endophthalmitis caused by P. agglomerans in Korea; it is also the first case reported outside of the United States.
Keyword
MeSH Terms
-
Aged
Anti-Bacterial Agents/therapeutic use
Endophthalmitis/complications/*microbiology/therapy
Enterobacteriaceae Infections/complications/*microbiology/therapy
Eye Infections, Bacterial/complications/*microbiology/therapy
Follow-Up Studies
Humans
Lung Diseases, Interstitial/*complications
Male
Pantoea/*isolation & purification
Visual Acuity
Vitrectomy
Figure
-
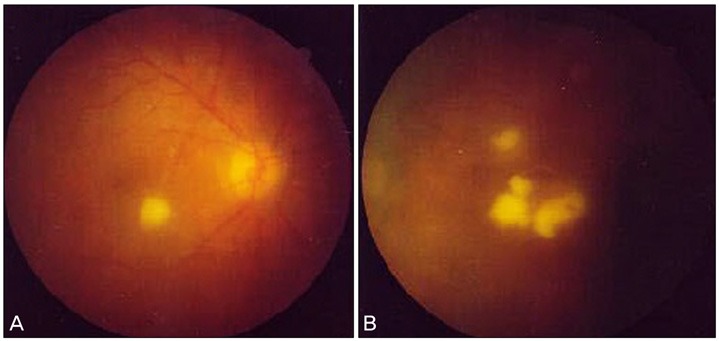
Fig. 1 (A) Right eye. Exudate was round, whitish-yellow, and slightly elevated towards the vitreous cavity. (B) Left eye. Exudates were irregular, whitish-yellow, and slightly elevated towards the vitreous cavity.

Fig. 2 Hypopyon in the anterior chamber of the right eye.
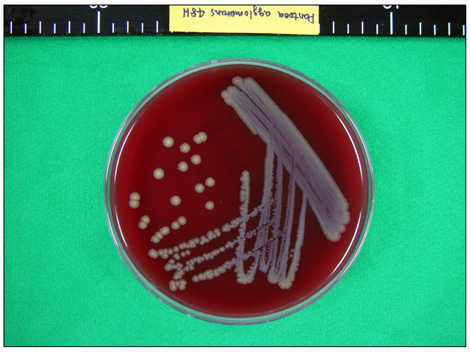
Fig. 3 Pantoea agglomerans was isolated in the vitreous culture. Yellow pigment-producing colonies that were 2 mm in size, nonhemolytic, and convex were detected on a blood agar plate.
Reference
-
1. Maki DG, Martin WT. Nationwide epidemic of septicemia caused by contaminated infusion products. IV. Growth of microbial pathogens in fluids for intravenous infusions. J Infect Dis. 1975. 131:267–272.2. Maki DG, Rhame FS, Mackel DC, Bennett JV. Nationwide epidemic of septicemia caused by contaminated intravenous products. I. Epidemiologic and clinical features. Am J Med. 1976. 60:471–485.3. Burchard KW, Barrall DT, Reed M, Slotman GJ. Enterobacter bacteremia in surgical patients. Surgery. 1986. 100:857–862.4. Chow JW, Fine MJ, Shlaes DM, et al. Enterobacter bacteremia: clinical features and emergence of antibiotic resistance during therapy. Ann Intern Med. 1991. 115:585–590.5. Gallagher PG. Enterobacter bacteremia in pediatric patients. Rev Infect Dis. 1990. 12:808–812.6. Jackson TL, Eykyn SJ, Graham EM, Stanford MR. Endogenous bacterial endophthalmitis: a 17-year prospective series and review of 267 reported cases. Surv Ophthalmol. 2003. 48:403–423.7. Zeiter JH, Koch DD, Park ED 2nd, Font RL. Endogenous endophthalmitis with lenticular abscess caused by Enterobacter agglomerans (Erwinia species). Ophthalmic Surg. 1989. 20:9–12.8. Cruz AT, Cazacu AC, Allen CH. Pantoea agglomerans, a plant pathogen causing human disease. J Clin Microbiol. 2007. 45:1989–1992.9. Ferguson R, Feeney C, Chirurgi VA. Enterobacter agglomerans: associated cotton fever. Arch Intern Med. 1993. 153:2381–2382.10. Harrison DW, Walls RM. "Cotton fever": a benign febrile syndrome in intravenous drug abusers. J Emerg Med. 1990. 8:135–139.11. Rowsey JJ, Newsom DL, Sexton DJ, Harms WK. Endophthalmitis: current approaches. Ophthalmology. 1982. 89:1055–1066.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of peritonitis caused by Pantoea agglomerans in a patient undergoing continuous ambulatory peritoneal dialysis
- Consecutive episodes of peritonitis in a patient undergoing peritoneal dialysis caused by unusual organisms: Brevibacterium and Pantoea agglomerans
- A Case of Bilateral Endogenous Enterococcus Faecalis Endophthalmitis in Liver Abscess
- A Case of the Bilateral Metastatic Endophthalmitis
- Endogenous Candida Endophthalmitis with Bilateral Massive Submacular Abscess
