A Case of Liposarcoma Arising in the Mesentery
- Affiliations
-
- 1Department of Internal Medicin, Soonchunhyang University College of Medicine, Korea.
- 2Department of Surgery, Soonchunhyang University College of Medicine, Korea.
- 3Department of Clinical Pathology, Soonchunhyang University College of Medicine, Korea.
- 4Digestive Disease Center, Konkuk University Medical Center, Seoul, Korea. chansshim@naver.com
- KMID: 783230
- DOI: http://doi.org/10.4166/kjg.2009.54.4.243
Abstract
- A liposarcoma is the most common soft tissue sarcoma in adults with an incidence of about 20% of all soft tissue sarcomas. Although incidence differs from a region of origination, a case arisen from mesentery has rarely been reported. We experienced a case of liposarcoma arising from the mesentery of a 51-year-old male patient. He was treated by wide excision. Histologically, the tumor was composed of a mixed well-differentiated liposarcoma with myxoid and spindle cell type.
Keyword
MeSH Terms
Figure
-
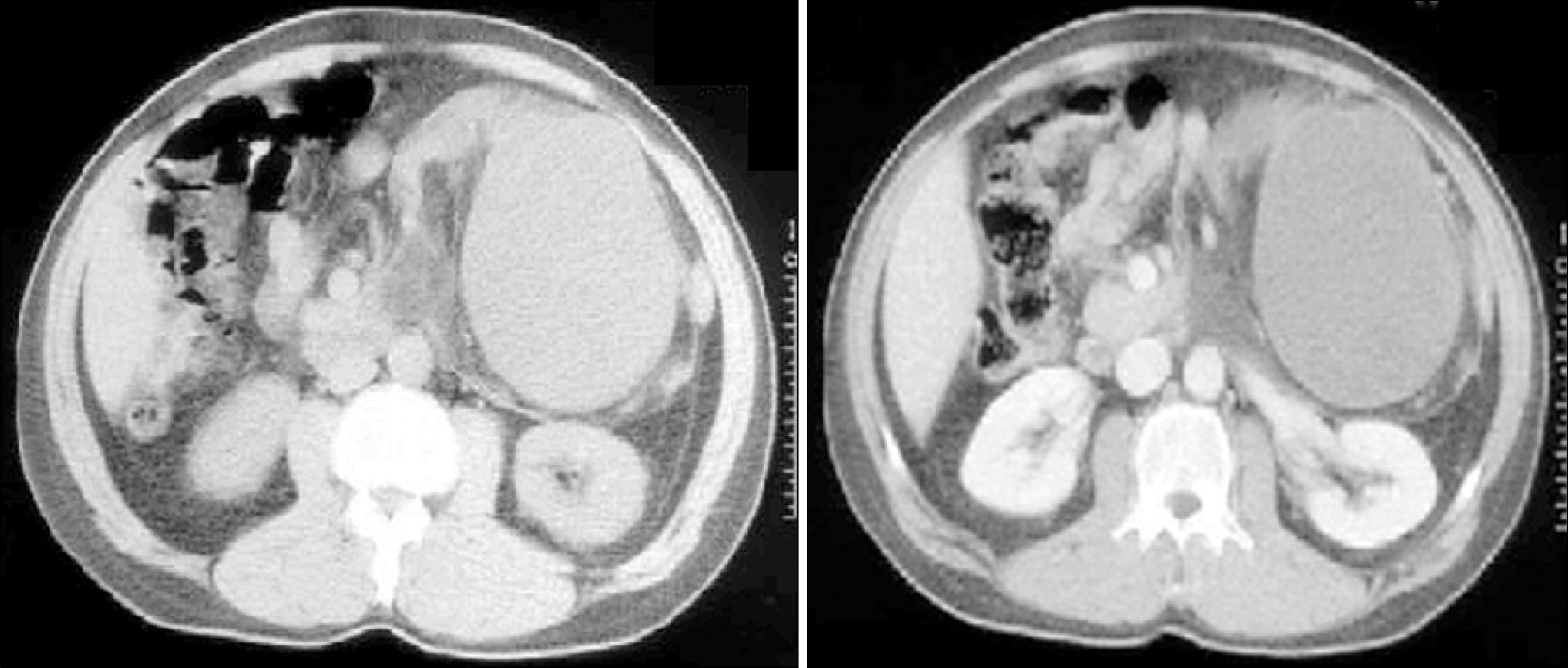
Fig. 1. CT findings showed a large, heterogeneous, left-sided abdominal mass that did not extend across the midline into the right abdomen. The mass displaced the descending and transverse colon anteriorly and pushed most of the bowel into the right abdomen.
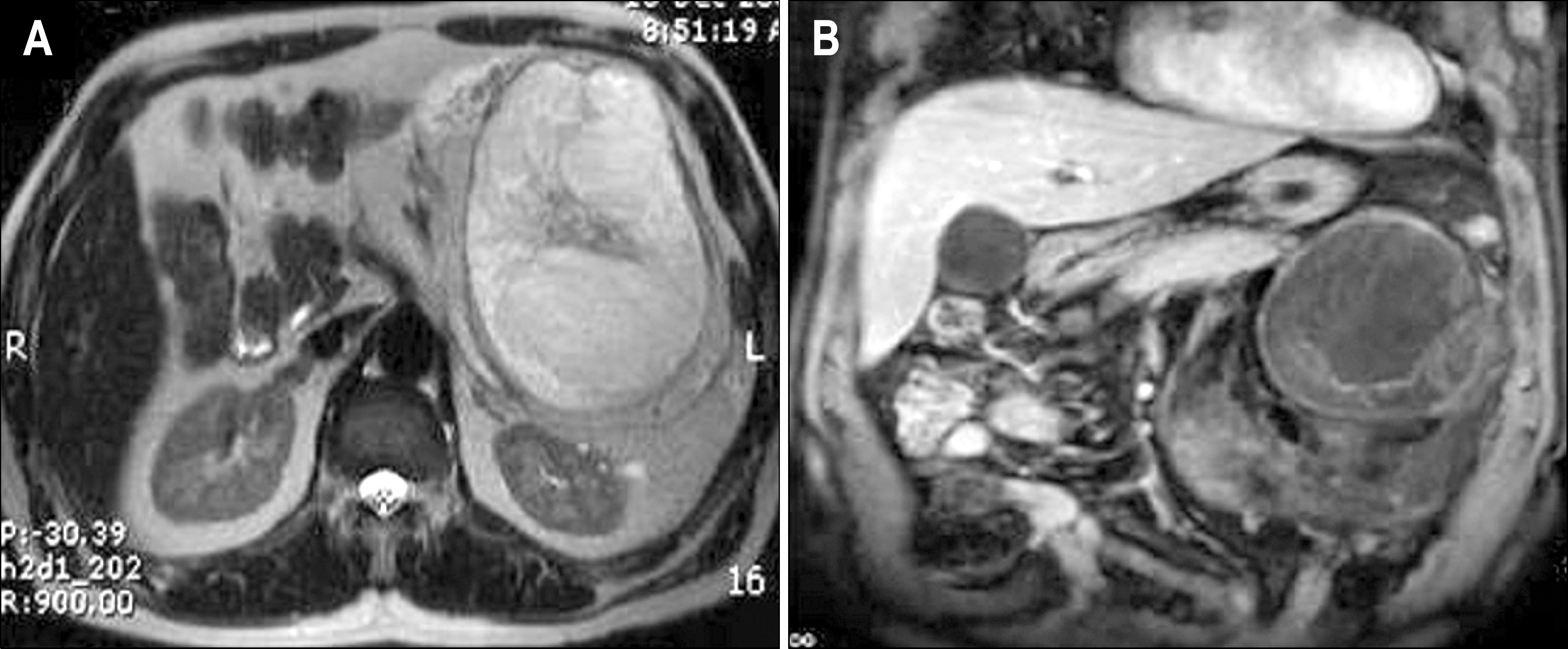
Fig. 2. (A) Axial T2-weighted fast spin echo MR image showed a large tumor with heterogeneous high signal intensity and central intermediate signal intensity in left peritoneal cavity. (B) Coronal contrast-enhanced T1-weighted MR image showed heterogenous peripheral enhancement in the mass.
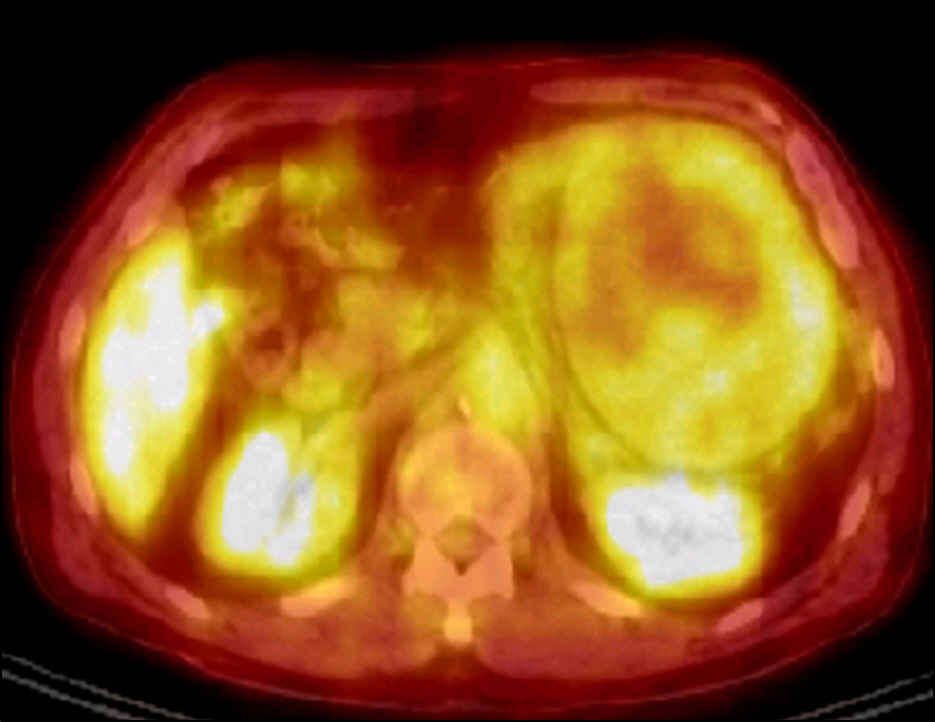
Fig. 3. Integrated 18F-PET CT showed a FDG uptake in the peripheral portion of the mass (peak SUV=2.37) with central pho-topenic region.
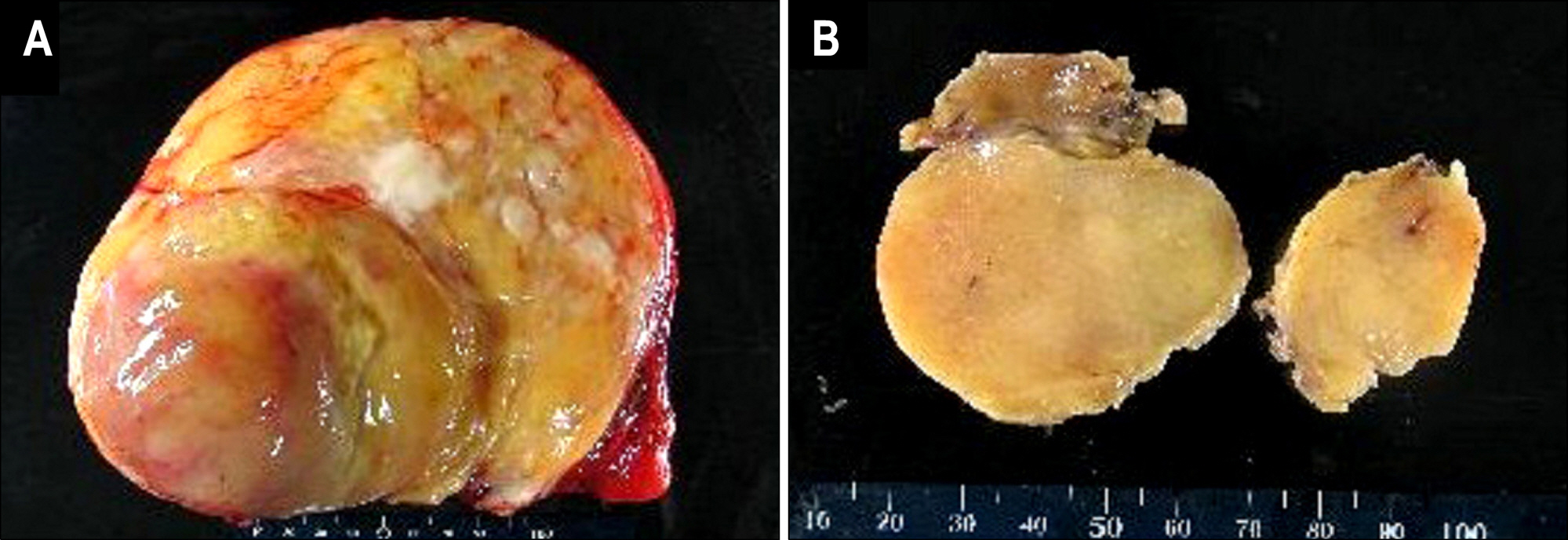
Fig. 4. Cut surfaces of the mesenteric masses. (A) The cut surface of the largest mass exhibited tan brown nodule in grey-yellow solid nodule. (B) The macroscopic findings of smaller masses resembled lipomas.
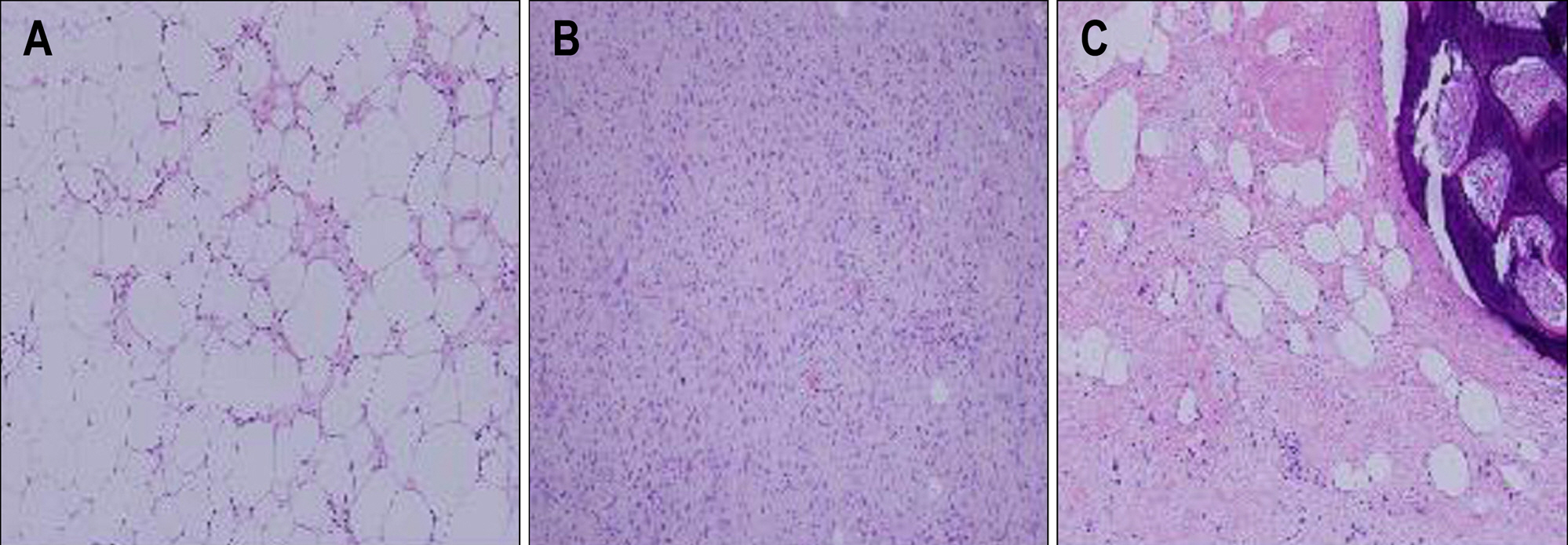
Fig. 5. Microscopic findings of liposarcoma masses. (A) Two smaller masses consisted of many mature adipocytes and intervening few atypical spindle cells. (B) The central nodule of the largest mass demonstrated proliferation of stellate spindle cells and plexiform vasculature on rich myxoid stroma. (C) The peripheral portion of the largest mass contained areas of sclerosing variant with bony metaplasia (A & C: H-E, ×100; B: H-E, ×40).
Cited by 1 articles
-
A Case of Pleomorphic Liposarcoma Originating from Mesentery
Jin Young Choi, Ji Eun Kim, Seung Min Lee, Ho Jun Kang, Ji Hee Sung, Byung Sung Koh, Ju Sang Park, Il Dong Kim, So Ya Baik
Korean J Gastroenterol. 2015;65(3):182-185. doi: 10.4166/kjg.2015.65.3.182.
Reference
-
1. Russell WO, Cohen J, Enzinger FM, et al. A clinical and pathological staging system for soft sarcomas. Cancer. 1977; 40:1562–1570.2. Lopez-Negrete L, Luyando L, Sala J, Lopez C, Menendez de Llano R, Gomez JL. Liposarcoma of the stomach. Abdominal Imaging. 1997; 22:373–375.3. Takagi H, Kato K, Yamada E, Suchi T. Six recent liposarcomas including the largest to date. J Surg Oncol. 1984; 26:260–267.4. Moyana TN. Primary mesenteric liposarcoma. Am J Gastroenterol. 1988; 83:89–92.5. Devita VT, Hellman S, Rosenberg SA. Cancer: principle practice of oncology. 6th ed.Philadelphia: Lippincott Williams & Wilkins;2001.6. Angelo P, Dei Tos MD. Liposarcoma: new entities and evolving concepts. Ann Diagn Pathol. 2000; 4:252–266.7. Robbins SL, Cotran RS. Robbins and Cotran pathologic basis of disease. 7th ed.Philadelphia: Elsevier Saunders;2005.8. Devita VT, Hellman S, Rosenberg SA. Cancer: principle practice of oncology. 7th ed.Philadelphia: Lippincott Williams & Wilkins;2005.9. Sato T, Nishimura G, Nonomura A, Miwa K. Intraabdominal and retroperitoneal liposarcomas. Int Surg. 1999; 84:163–167.10. Singer S, Antonescu CR, Riedel E, Brennan MF. Histologic subtype and margin of resection predict pattern of recurrence and survival for retroperitoneal liposarcoma. Ann Surg. 2003; 238:358–371.
Article11. Bautista N, Su W, Oconnell TX. Retroperitoneal soft-tissue sarcomas: prognosis and treatment of primary and recurrent disease. Am Surg. 2000; 66:832–836.12. Reitan JB, Kaalhus O, Brennhovd IO, Sager EM, Stenwig AE, Talle K. Prognosis factors in liposarcoma. Cancer. 1985; 55:2482–2490.13. Miettinen M, Sobin LH, Lasota J. Gastrointestinal stromal tumors of the stomach: a clincopathologic, immunohistochemical, and molecular genetic study of 1765 cases with longterm follow-up. Am J Surg Pathol. 2005; 29:52–68.14. Chang HR, Hajdu SI, Collin C, Brennan MF. The prognostic value of histologic subtypes in primary extremity liposarcoma. Cancer. 1989; 64:1514–1520.
Article15. Enzinger FM, Winslow DJ. Liposarcoma. A study of 103 cases. Virchows Arch. 1962; 335:367–388.16. Fernandez-Trigo V, Sugarbaker PH. Sarcomas involving the abdominal and pelvic cavity. Tumori. 1993; 79:77–91.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Giant Liposarcoma Arising in the Mesentery
- The Magnetic Resonance (MR) Imaging Features of Myxoid Liposarcoma Arising from the Mesentery: a Case Report
- Primary Round Cell Liposarcoma of the Omentum: A case report
- A Case of Pleomorphic Liposarcoma Originating from Mesentery
- Primary Multiple Mesenteric Liposarcoma of the Transverse Mesocolon
