Dry Eye After Cataract Surgery and Associated Intraoperative Risk Factors
- Affiliations
-
- 1The Catholic University of Korea, St. Vincent's hospital, Suwon, Korea.
- 2The Catholic University of Korea, Seoul St. Mary's Hospital, Seoul, Korea. mskim@catholic.ac.kr
- KMID: 754720
- DOI: http://doi.org/10.3341/kjo.2009.23.2.65
Abstract
-
PURPOSE: To investigate changes in dry eye symptoms and diagnostic test values after cataract surgery and to address factors that might influence those symptoms and test results.
METHODS
Twenty-eight eyes from 14 patients with preoperative dry eye (dry eye group) and 70 eyes from 35 patients without preoperative dry eye (non-dry eye group) were studied prospectively. In each group, we measured values such as tear break-up time (tBUT), Schirmer I test (ST-I), tear meniscus height (TMH), and subjective dry eye symptoms (Sx), and evaluated the postoperative changes in these values. We also evaluated the influence of corneal incision location and shape on these values. The correlations between these values and microscopic light exposure time and phacoemulsification energy were investigated.
RESULTS
In the dry eye group, there were significant aggravations in Sx at 2 months postoperatively and in TMH at 3 days, 10 days, 1 month, and 2 months postoperatively, compared with preoperative values. All dry eye test values were significantly worse after cataract surgery in the non-dry eye group. With regard to incision location, there was no difference in tBUT, Sx, ST-I, or TMH in either the dry eye group or the non-dry eye group at any postoperative time point. Regarding incision shape, there was no difference in tBUT, Sx, ST-I or TMH at any postoperative time point in the dry eye group. In the superior incision sub-group of the non-dry eye group, tBUT and Sx were worse in the grooved incision group at day 1. In the temporal incision sub-group of the non-dry eye group, Sx were worse in the grooved incision group at 1 day, 3 days, and 10 days postoperatively. In both groups, significant correlations were noted between microscopic light exposure time and dry eye test values, but no correlation was noted between phacoemulsification energy and dry eye test values.
CONCLUSIONS
Cataract surgery may lead to dry eye. A grooved incision can aggravate the symptoms during the early postoperative period in patients without dry eye preoperatively. Long microscopic light exposure times can have an adverse effect on dry eye test values.
Keyword
MeSH Terms
Figure
-
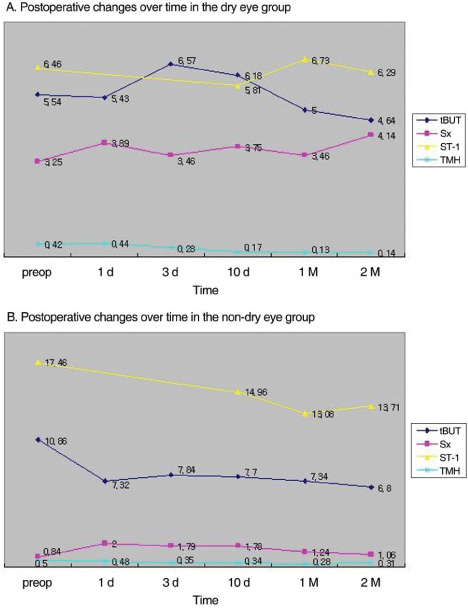
Fig. 1 Postoperative changes in tear break-up time (tBUT, second), dryness symptoms (Sx), Schirmer test I (ST-I, mm) and tear meniscus height (TMH, mm) over time in both the dry eye (A) and non-dry eye group (B). In the dry eye group, there were significant aggravations in Sx at 2 months postoperative and in TMH at 3 days, 10 days, 1 month, and 2 months postoperative (p<0.05). In the non-dry eye group, almost all dry eye test values were significantly worse after cataract surgery (p<0.05).
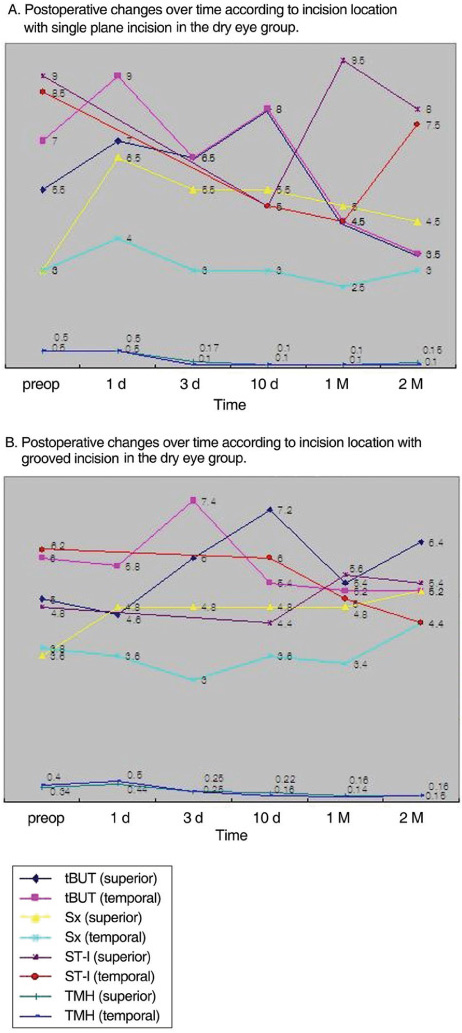
Fig. 2 Postoperative changes in tear break-up time (tBUT, second), dryness symptoms (Sx), Schirmer test I (ST-I, mm) and tear meniscus height (TMH, mm) over time according to incision location with a single plane (A) or grooved incision (B) in the dry eye group. There was no difference in tBUT, Sx, ST-I, or TMH according to incision location in the single plane incision sub-group at any postoperative time point (p>0.05). There was no difference in tBUT, Sx, ST-I, or TMH according to incision location in the grooved incision sub-group at any postoperative time point (p>0.05).
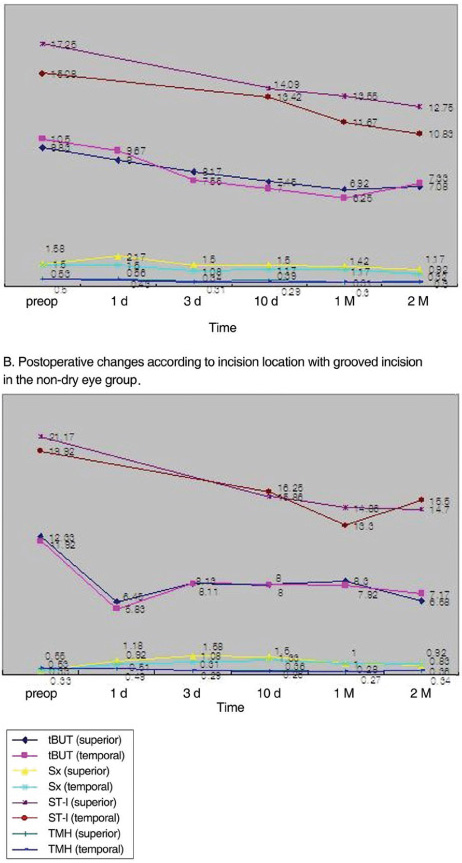
Fig. 3 Postoperative changes in tear break-up time (tBUT, second), dryness symptoms (Sx), Schirmer test I (ST-I, mm) and tear meniscus height (TMH, mm) over time according to incision location with a single plane (A) or grooved incision (B) in the non-dry eye group. There was no difference in tBUT, Sx, ST-I, or TMH according to incision location in the single plane incision sub-group at any postoperative time point (p>0.05). There was no difference in tBUT, Sx, ST-I, or TMH according to incision location in the grooved incision sub-group at any postoperative time point (p>0.05).

Fig. 4 Postoperative changes in tear break-up time (tBUT, second), dryness symptoms (Sx), Schirmer test I (ST-I, mm) and tear meniscus height (TMH, mm) over time according to incision shape with a superior (A) or temporal incision (B) in the dry eye group. There was no difference in tBUT, Sx, ST-I or TMH according to incision shape in the superior incision sub-group at any postoperative time point (p>0.05). There was no difference in tBUT, Sx, ST-I or TMH according to incision shape in the temporal incision sub-group at any postoperative time point (p>0.05).

Fig. 5 Postoperative changes in tear break-up time (tBUT, second), dryness symptoms (Sx), Schirmer test I (ST-I, mm) and tear meniscus height (TMH, mm) over time according to incision shape with a superior (A) or temporal incision (B) in the non-dry eye group. tBUT were shorter and Sx were worse with grooved incision than single plane incision at postoperative day 1 in the superior incision sub-group (p=0.04). Sx were worse in the grooved incision subgroup at 1 day (p=0.00), 3 days (p=0.01), and 10 days (p=0.01) postoperative in the temporal incision sub-group.
Cited by 8 articles
-
Effectiveness of Cyclosporine-steroid Treatment after Cataract Surgery according to Dry Eye Severity
Jae Yeong Park, Sang Cheol Yang, Young Min Park, Ji Eun Lee, Choul Yong Park, Jong Soo Lee
J Korean Ophthalmol Soc. 2019;60(9):821-828. doi: 10.3341/jkos.2019.60.9.821.Evaluation of the Protective Effect of an Ophthalmic Viscosurgical Device on the Ocular Surface in Dry Eye Patients during Cataract Surgery
Do Yeh Yoon, Joo Hyun Kim, Hyun Sun Jeon, Hee Eun Jeon, Sang Beom Han, Joon Young Hyon
Korean J Ophthalmol. 2019;33(5):467-474. doi: 10.3341/kjo.2019.0060.Changes in Clinical Manifestations of Dry Eye Syndrome after Cataract Surgery and the Affecting Factors
Young Rae Roh, Sang Mok Lee, Young Keun Han, Mee Kum Kim, Won Ryang Wee, Jin Hak Lee
J Korean Ophthalmol Soc. 2011;52(9):1030-1038. doi: 10.3341/jkos.2011.52.9.1030.The Influence of Preoperative Meibomian Gland Disease on Dryness after Cataract Surgery
Jin Ah Lee, Yang Kyeung Cho
J Korean Ophthalmol Soc. 2016;57(2):228-235. doi: 10.3341/jkos.2016.57.2.228.Effect of 0.05% Cyclosporine A on the Ocular Surface after Photorefractive Keratectomy
Yong Il Kim, Sung Hyun Koo, Sang Won Ha, Gwang Ja Lee, Kyoo Won Lee, Young Jeung Park
J Korean Ophthalmol Soc. 2016;57(5):710-717. doi: 10.3341/jkos.2016.57.5.710.A Pilot Study of Changes in Tear Film Short-term Dynamics with Infrared Imaging after Phacoemulsification
Seonjoo Kim, Yuli Park, Kyung-Sun Na, Hyun-Seung Kim
J Korean Ophthalmol Soc. 2017;58(4):395-400. doi: 10.3341/jkos.2017.58.4.395.Effect of 0.1% Sodium Hyaluronate and 0.05% Cyclosporine on Tear Film Parameters after Cataract Surgery
Won Choi, Kyung-Chul Yoon
J Korean Ophthalmol Soc. 2011;52(7):800-806. doi: 10.3341/jkos.2011.52.7.800.Changes of Higher Order Aberration Analyzed by Continuous Measurement after Phacoemulsification
Hyung Bin Lim, Jong Joo Lee, Si Hwan Choi
J Korean Ophthalmol Soc. 2015;56(1):25-32. doi: 10.3341/jkos.2015.56.1.25.
Reference
-
1. Hiroko BM. Steinert RF, editor. Cataract Surgery in the Presence of other ocular comorbidities. Cataract Surgery: Technique, Complication and Management. 2004. Saunders;chap. 32.2. Jagat R, Amit G, Gagandeep SB, et al. Outcomes of phacoemulsification in patients with dry eye. J Cataract Refract Surg. 2002. 28:1386–1389.3. Xue-Min Li, Lizhong H, Jinping H, Wei W. Investigation of dry eye disease and analysis of the pathologic factors in patients after cataract surgery. Cornea. 2007. 26:S16–S20.4. Kohlhaas M. Corneal sensation after cataract and refractive surgery. J Cataract Refract Surg. 1998. 24:1399–1409.5. Ang RT, Dartt DA, Tsubota K. Dry eye after refractive surgery. Curr Opin Ophthalmol. 2001. 12:318–322.6. Belmonte C. Eye Driness Sensations after Refractive surgery: Impaired Tear Secretion or "Phantom" Cornea? J Refract Surg. 2007. 23:598–602.7. Altinors DD, Akca S, Akova YA, et al. Smoking associated with damage to the lipid layer of the ocular surface. Am J Ophthalmol. 2006. 141:1016–1021.8. Moss SE, Klein R, Klein BE. Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. 2000. 118:1264–1268.9. Lee AJ, Lee J, Saw SM, et al. Prevalence and risk factors associated with dry eye symptoms: a population based study in Indonesia. Br J Ophthalmol. 2002. 86:1347–1351.10. Schiffman RM, Christianson MD, Jacobsen G, et al. Reliability and Validity of the Ocular Surface Disease Index. Arch Ophthalmol. 2000. 118:615–621.11. Vitali C, Moutsopoulos HM, Bombardieri S. The European community study group on diagnostic criteria for Sjogren's syndrome.sensitivity and specificity of tests for ocular and oral involvement in Sjogren's syndrome. Ann Rheum Dis. 1994. 53:637–647.12. Khanal S, Tomlinson A, McFadyen A, et al. Dry eye diagnosis. Invest Ophthalmol Vis Sci. 2008. 49:1407–1414.13. Walker TD. Benzalkonium Toxicity. Clin Experiment Ophthalmol. 2004. 32:657.14. Fine IH, Hoffman RS, Packer M. Profile of clear corneal cataract incisions demonstrated by ocular coherence tomography. J Cataract Refract Surg. 2007. 33:94–97.15. Fine IH, Hoffmann RS, Packer M. Steinert RF, editor. Incision Construction. Cataract Surgery: Technique, Complication and Management. 2004. Saunders;chap.12.16. Jaffe NS, Jaffe MS, Jaffe GF. Surgical Technique. Cataract Surgery and Its Complications. 1997. 6th ed. Mosby;chap. 9.17. Donnenfeld ED, Solomon K, Perry HD, et al. The effect of hinge position on corneal sensation and dry eye after LASIK. Ophthalmology. 2003. 110:1023–1029.18. Chang-Ling T, Vannas A, Holden BA, O'Leary DJ. Incision Depth Affects the recovery of corneal sensitivity and neural regeneration in the cat. Invest Ophthalmol Vis Sci. 1990. 31:1533–1541.19. Chan-Ling T, Tervo K, Tervo T, et al. Long term neural regeneration in the rabbit following 180 degress Limbal Incision. Invest Ophthalmol Vis Sci. 1987. 28:2083–2088.20. Ernest PH, Neuhann T. Posterior limbal incision. J Cataract Refract Surg. 1996. 23:78–84.21. Mencucci R, Ambrosini S, Ponchietti C, et al. Ultrasound thermal damage to rabbit corenas after simulated phacoemulsification. J Cataract Refract Surg. 2005. 31:2180–2186.22. Michels M, Sternberg P Jr. Operating microscope_induced retinal phototoxicity: Pathophysiology, Cinical Manifestations and Prevention. Surv Ophthalmol. 1990. 34:237–252.23. Michael R, Wegener A. Estimation of safe exposure time from an ophthalmic operating microscope with regard to ultraviolet radiation and blue-light hazards to the eye. J Opt Soc Am A Opt Image Sci Vis. 2004. 21:1388–1392.24. Pavilack MA, Brod RD. Site of potential operating microscope light-induced phototoxicity on the human retina during temporal approach eye surgery. Ophthalmology. 2001. 108:381–385.25. Serin D, Karsloğlu S, Kyan A, Alagöz G. A simple approach to the repeatability of the Shirmer test without anesthesia. Cornea. 2007. 26:903–906.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prevalence and Risk Factors of Dry Eye Disease after Refractive Surgery
- The Effect of Topical Cyclosporine 0.05% on Dry Eye after Cataract Surgery
- Comparison of the Effects of 0.05% and 0.1% Cyclosporine for Dry Eye Syndrome Patients after Cataract Surgery
- Factors Associated with Dry Eye Symptoms in Elderly Koreans: The Fifth Korea National Health and Nutrition Examination Survey 2010–2012
- Change of Lipid Layer in Tear Film after Cataract Surgery
