A Case of Weill-Marchesani Syndrome with Inversion of Chromosome 15
- Affiliations
-
- 1Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea. eungkkim@yumc.yonsei.ac.kr
- 2Department of Ophthalmology, Soonchunhyang University College of Medicine, Soonchunhayng University Bucheon Hospital, Bucheon, Korea.
- KMID: 754646
- DOI: http://doi.org/10.3341/kjo.2007.21.4.255
Abstract
- PURPOSE: To present a case of Weill-Marchesani syndrome with corneal endothelial dysfunction due to anterior dislocation of a spherophakic lens and corneolenticular contact. METHODS: A 17-year-old woman presented with high myopia and progressive visual disturbance. She was of short stature and had brachydactyly. Her initial Snellen best corrected visual acuity (BCVA) was 20/50 (-sph 20.50 -cyl 3.00 Ax 180) in her right eye and 20/40 (-sph 16.00 -cyl 6.00 Ax 30) in her left eye. Slit lamp examination revealed a dislocated spherophakic lens touching corenal endothelium. A microspherophakic lens, hypoplastic ciliary body, and elongated zonules were confirmed on rotating Scheimpflug camera (Pentacam(R)) and on ultrasound biomicroscopy. Specular microscopy showed corneal endothealial dysfunction. Systemic evaluation was performed, and chromosomal study showed 46, XX, inv (15) (q13qter). The patient was diagnosed with Weill-Marchesani syndrome. RESULTS: Due to impending corneal decompensation, phacoemulsification and suture fixation of the intraocular lens were performed. The operation and postoperative course were uneventful. Three months postoperatively, the visual acuity was 20/30 (OD) and 20/40 (OS) without correction, and BCVA was 20/20 (+sph 0.50 -cyl 2.00 Ax 160 : OD) and 20/25 (+sph 1.50 -cyl 3.00 Ax 30 : OS). During the follow-up period, increased corneal endothelial counts, hexagonality, and decreased corneal thickness were achieved. CONCLUSIONS: In Weill-Marchesani syndrome with a chromosomal anomaly, a dislocated spherophakic lens may cause severe corneal endothelial dysfunction due to corneolenticular contact, and prompt lensectomy is important to prevent such complications.
MeSH Terms
-
*Abnormalities, Multiple
Adolescent
*Chromosomes, Human, Pair 15
Diagnosis, Differential
Dwarfism/*genetics
Endothelium, Corneal/pathology/ultrasonography
Female
Fingers/*abnormalities
Hand Deformities, Congenital/diagnosis/*genetics
Humans
Inversion, Chromosome/*genetics
Lens Implantation, Intraocular/methods
Lens Subluxation/diagnosis/*genetics/surgery
Microscopy, Acoustic
Phacoemulsification/methods
Syndrome
Figure
-

Fig. 1 X-ray of the hand showing brachydactyly, short metacarpal bones, and delayed carpal ossification.
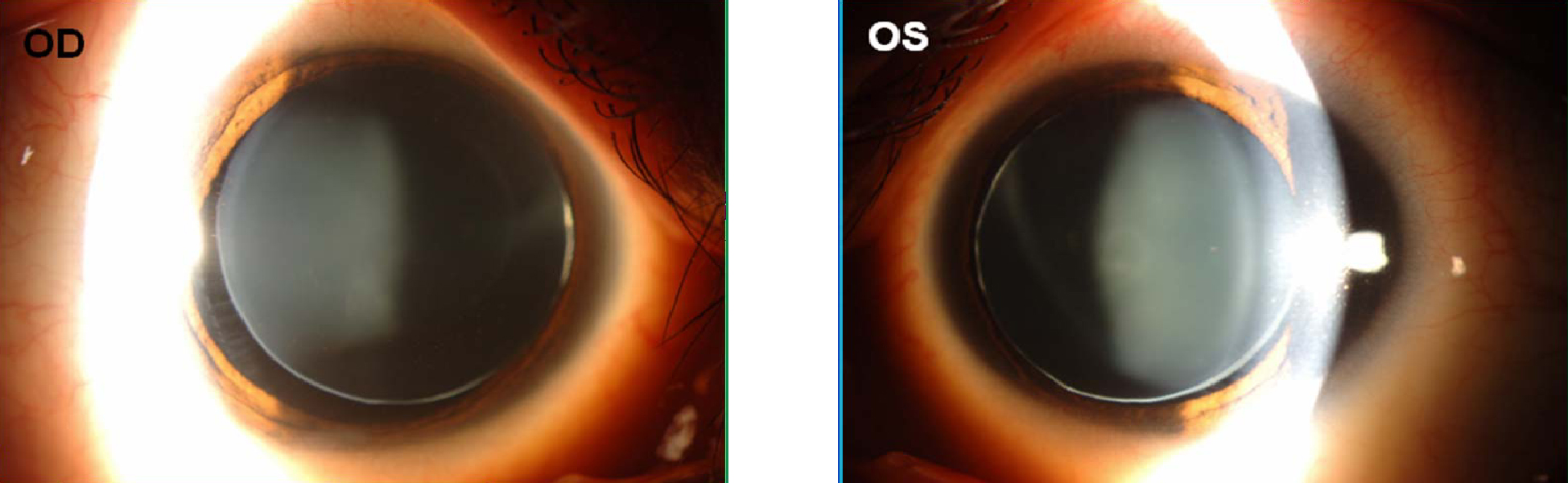
Fig. 2 Slit lamp examination showing bilateral superonasal subluxation of the crystalline lens with the lens equator and zonule visible within the pupil.
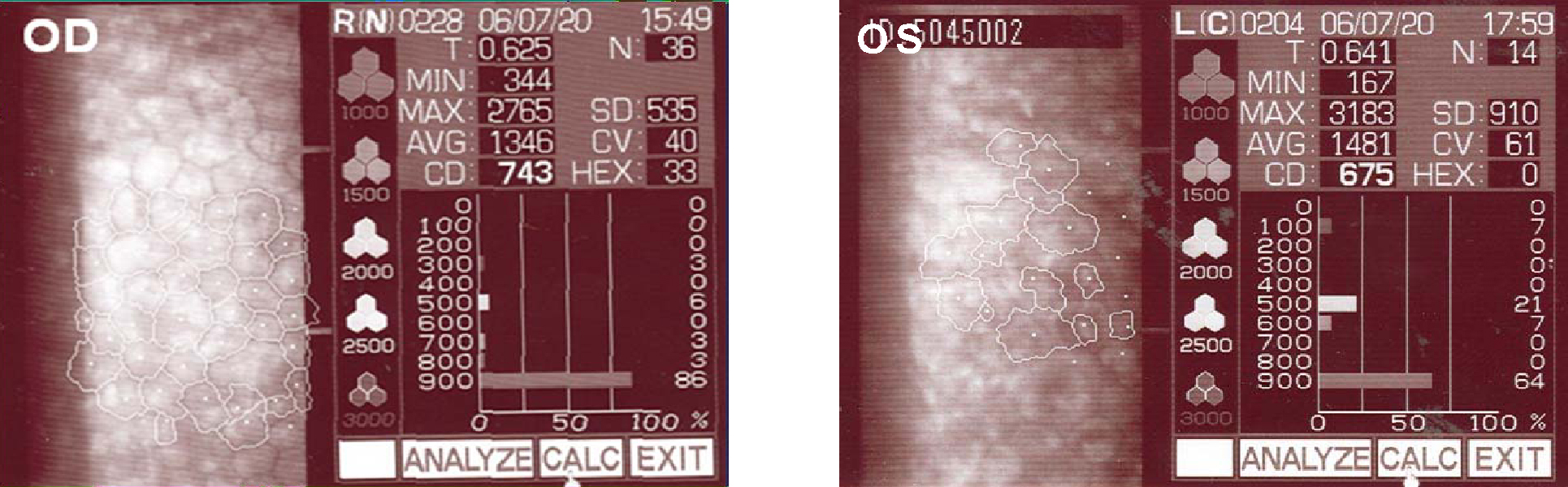
Fig. 3 Specular microscopic examination showing decreased endothelial cell counts (743/675 cells per mm2) and hexagonality (33/0%) due to corneal endothelial dysfunction.
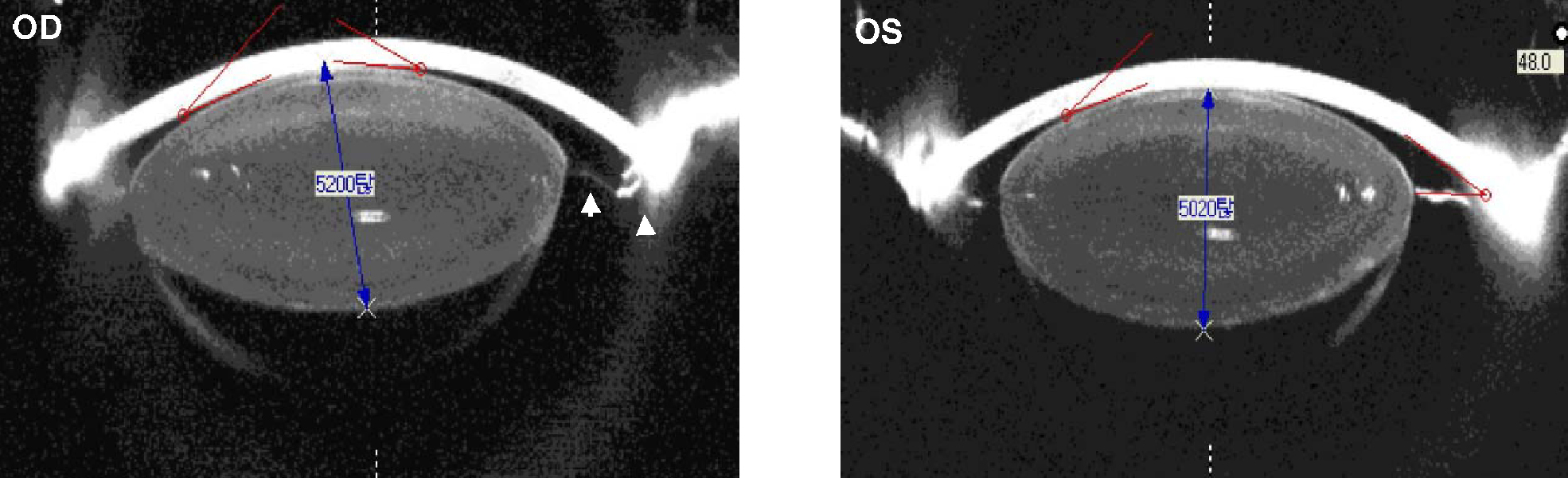
Fig. 4 On rotating Scheimpflug camera examination, increased anteroposterior diameter of the spherophakic lens (5200/5020 µm) and contact between the anteriorly dislocated lens and the central corneal endothelium were clearly demonstrated. The hypoplastic ciliary body (arrow) and elongated zonules (arrowhead) were also observed.
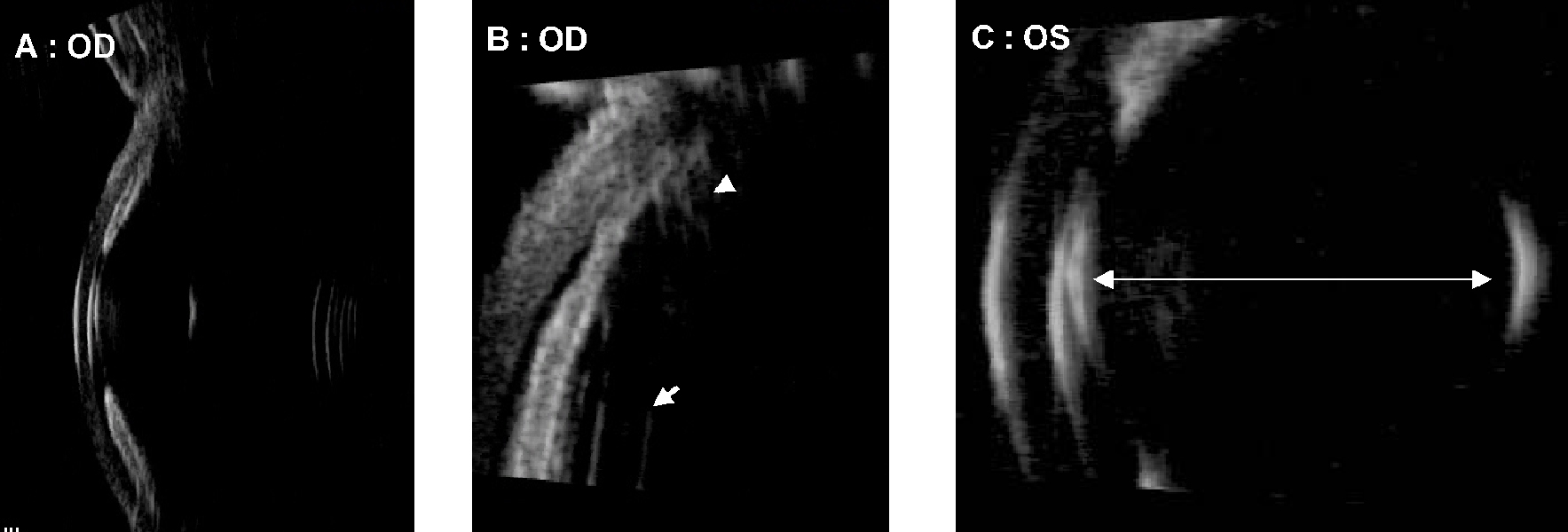
Fig. 5 Ultrasound biomicroscopic assessment revealed (A) a steep anterior lens curvature, angle narrowing and iridocorneal contact, (B) hypoplastic ciliary body (arrowhead) and elongated zonules (arrow) in her right eye, and (C) increased anteroposterior diameter of lens and iridocorneal/corneolenticular contact in her left eye.

Fig. 6 Chromosomal analysis of phytohemagglutinin stimulated peripheral lymphocytes by the Giemsa banding technique revealed 46, XX, inv (15) (q13qter) (red arrowhead).

Fig. 7 Three months postoperatively, the cornea was clear and the anterior chamber had deepened. The visual acuity was 20/30 (OD) and 20/40 (OS) without correction, and best corrected visual acuity was 20/20 (+sph 0.50 -cyl 2.00 Ax 160 : OD) and 20/25 (+sph 1.50-cyl 3.00 Ax 30 : OS).
Reference
-
1. Weill G. Ectopie du cristallin et malformations générales. Ann Ocul. 1932. 169:21–44.2. Marchesani O. Brachydaktylie und angeborene kugellines als systemerkrankung. Klin Mibl Augenheilkd. 1939. 103:392–406.3. Faivre L, Dollfus H, Lyonnet S, et al. Clinical homogeneity and genetic heterogeneity in Weill-Marchesani syndrome. Am J Med Genet A. 2003. 123:204–207.4. Dagoneau N, Benoist-Lasselin C, Huber C, et al. ADAMTS10 mutations in autosomal recessive Weill-Marchesani syndrome. Am J Hum Genet. 2004. 75:801–806.5. Wirtz MK, Samples JR, Kramer PL, et al. Weill-Marchesani syndrome--possible linkage of the autosomal dominant form to 15q21.1. Am J Med Genet. 1996. 65:68–75.6. Dietlein TS, Mietz H, Jacobi PC, Krieglstein GK. Spherophakia, nanophthalmia, hypoplastic ciliary body and glaucoma in brachydactyly-associated syndromes. Graefes Arch Clin Exp Ophthalmol. 1996. 234:suppl 1. S187–S192.7. Lee WR, Lee HB. A Case of Spherophakia. J Korean Ophthalmol Soc. 1982. 23:761–765.8. Park SC, Lee KH. Two Cases of Spherophakia in Sister and Brother. J Korean Ophthalmol Soc. 1986. 27:429–435.9. Kloepfer HW, Rosenthal JW. Possible genetic carriers in the spherophakia-brachymorphia syndrome. Am J Hum Genet. 1955. 7:398–425.10. Faivre L, Gorlin RJ, Wirtz MK, et al. In frame fibrillin-1 gene deletion in autosomal dominant Weill-Marchesani syndrome. J Med Genet. 2003. 40:34–36.11. Apte SS. A disintegrin-like and metalloprotease (reprolysin type) with thrombospondin type 1 motifs: the ADAMTS family. Int J Biochem Cell Biol. 2004. 36:981–985.12. Porter S, Clark IM, Kevorkian L, Edwards DR. The ADAMTS metalloproteinases. Biochem J. 2005. 386:15–27.13. Nicholson AC, Malik SB, Logsdon JM, Van Meir EG. Functional evolution of ADAMTS genes: evidence from analyses of phylogeny and gene organization. BMC Evol Biol. 2005. 5:11.14. Hayward C, Brock DJ. Fibrillin-1 mutations in Marfan syndrome and other type-1 fibrillinopathies. Hum Mutat. 1997. 10:415–423.15. Sakai LY, Keene DR, Engvall E. Fibrillin, a new 350-kD glycoprotein, is a component of extracellular microfibrils. J Cell Biol. 1986. 103:2499–2509.16. Willi M, Kut L, Cotlier E. Pupillary-block glaucoma in the Marchesani syndrome. Arch Ophthal. 1973. 90:504–508.17. Ritch R, Wand M. Treatment of the Weill-Marchesani syndrome. Ann Ophthalmol. 1981. 13:665–667.18. Macken PL, Pavlin CJ, Tuli R, Trope GE. Ultrasound biomicroscopic features of spherophakia. Aust N Z J Ophthalmol. 1995. 23:217–220.19. Urbanek J. Glaucoma juvenile inversum. Z Augenheilkd. 1930. 71:171–172.20. Pavlin CJ, Buys YM, Pathmanathan T. Imaging zonular abnormalities using ultrasound biomicroscopy. Arch Ophthal. 1998. 116:854–857.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ocular Manifestations of Pediatric Systemic Disease
- Incidence and Karyotypes According to Each Chromosome in 13 Cases with Inversion
- A Case of Pericentric Inversion of Chromosome 5(p15.1q11.2 )
- Chromosome abnormalities in a referred population for suspected chromosomal aberrations: a report of 4117 cases
- A Case of Paracentric Inversion of Chromosome 12(q13q22)
