The Safety and Efficacy of Transconjunctival Sutureless 23-gauge Vitrectomy
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea.
- 2Seoul Artificial Eye Center, Seoul National University Hospital Clinical Research Institute, Seoul, Korea.
- 3Seoul National University Bundang Hospital, Seoul, Korea. jiani4@snu.ac.kr
- KMID: 754636
- DOI: http://doi.org/10.3341/kjo.2007.21.4.201
Abstract
- PURPOSE: To evaluate the efficacy and safety of vitreoretinal surgery using a 23-gauge transconjunctival sutureless vitrectomy (TSV) system for various vitreoretinal diseases. METHODS: A retrospective, consecutive, interventional case series was performed for 40 eyes of 40 patients. The patients underwent vitreoretinal procedures using the 23-gauge TSV system, including idiopathic epiretinal membrane (n=7), vitreous hemorrhage (n=11), diabetic macular edema (n=10), macular hole (n=5), vitreomacular traction syndrome (n=5), diabetic tractional retinal detachment (n=1), and rhegmatogenous retinal detachment (n=1). Best corrected visual acuity (BCVA), intraocular pressure (IOP), and intra- and post-operative complications were evaluated. RESULTS: Intraoperative suture placement was necessary in 3 eyes (7.5%). The median BCVA improved from 20/400 (LogMAR, 1.21+/-0.63) to 20/140 (LogMAR, 0.83+/-0.48) at 1 week (p=0.003), 20/100 (LogMAR, 0.85+/-0.65) at 1 month (p=0.002), 20/100 (LogMAR, 0.73+/-0.6) at 3 months (p=0.001). In 1 eye, IOP was 5 mmHg at 2 hours and 4 mmHg at 5 hours, but none of the eyes showed hypotony after 1 postoperative day. No serous postoperative complications were observed during a mean follow-up of 8.4+/-3.4 months (range 3-13 months) CONCLUSIONS: The 23-gauge TSV system shows promise as an effective and safe technique for a variety of vitreoretinal procedures. It appears to be a less traumatic, more convenient alternative to 20-gauge vitrectomy in some indications.
Keyword
MeSH Terms
Figure
-
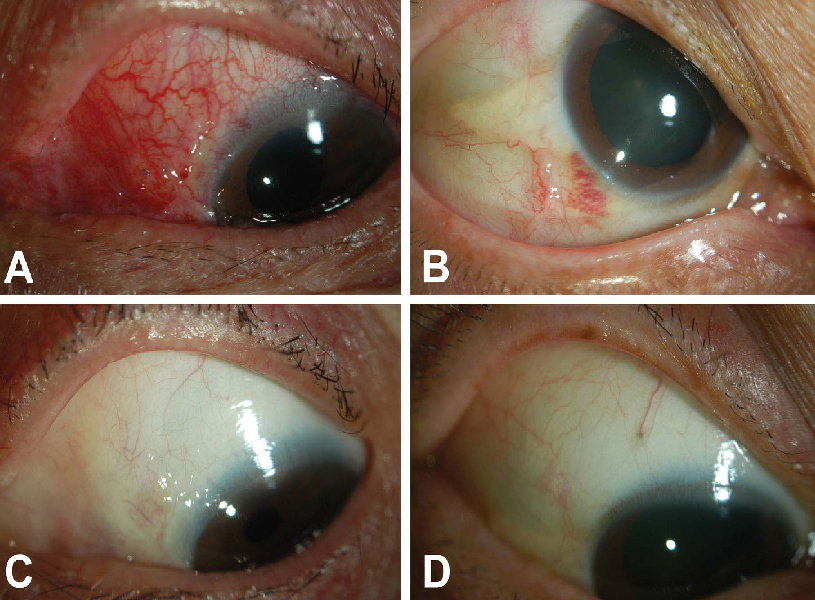
Fig. 1 Anterior segment photography of eyes after performing 20-gauge standard vitrectomy (A: postoperative 1 week, C: postoperative 6 weeks) and 23-gauge transconjunctival sutureless vitrectomy (B: postoperative 1 week, D: postoperative 6 weeks). Conjunctival injection and late scar formation were almost negligible in the external feature of the eyes that underwent 23-gauge TSV (B,D). On the contrary, severe conjunctival injection (A) and late protruding healed scar were prominent in the eye that underwent 20-gauge vitrectomy (A,C).
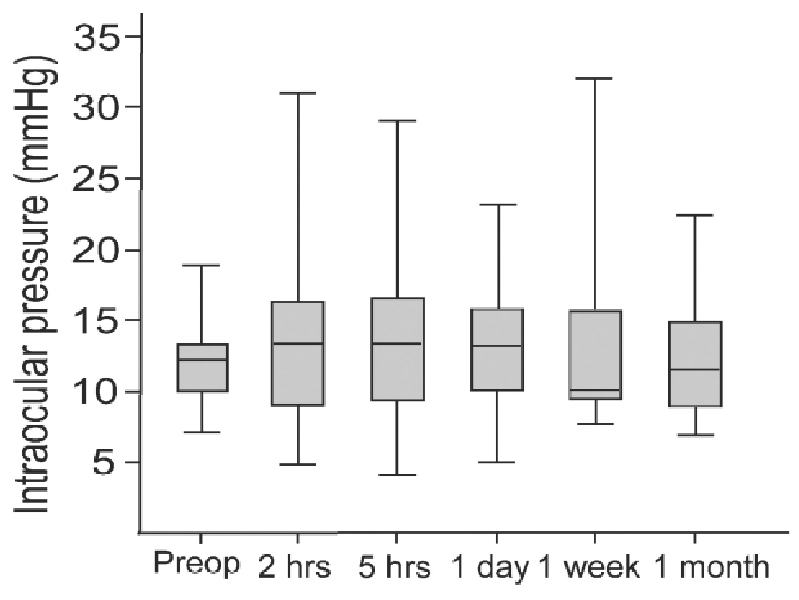
Fig. 2 Preoperative and postoperative intraocular pressure changes at 2 hours, 5 hours, 1 day, 1 week, and 1 month. There were no significant differences in IOP among the measurements. No hypotony was observed after 1 postoperative day in any of the 40 eyes. preop=preoperative; h=hours; d=day; w=week; m=month.
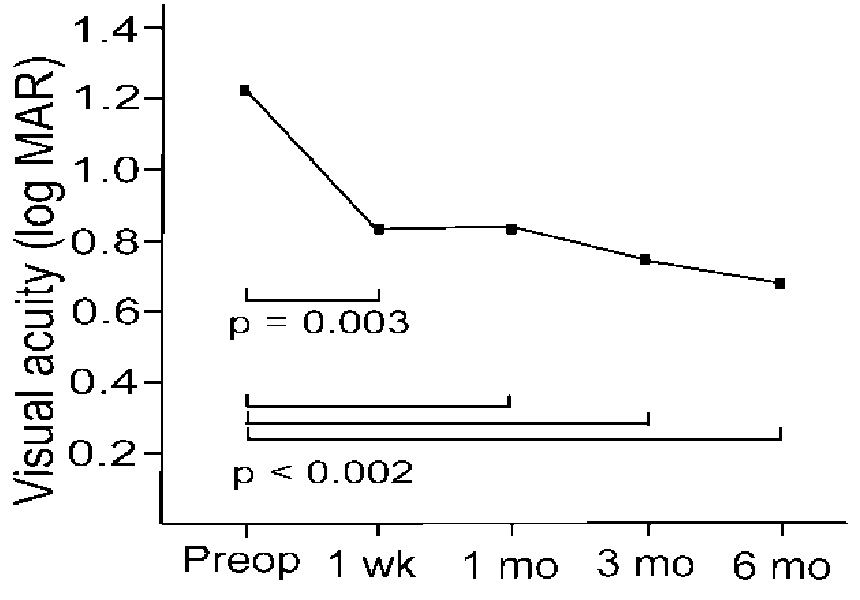
Fig. 3 Visual acuity in logarithm of the minimal angle of resolution (LogMAR) units observed preoperatively and postoperatively at 1 week and 1, 3 and 6 months following surgery. Visual improvement was noted at 1 week and 1, 3 and 6 months following 23-gauge transconjunctival sutureless vitrectomy (Wilcoxon signed rank test, P < .05). Preop; preoperative, wk; week, mo; month.
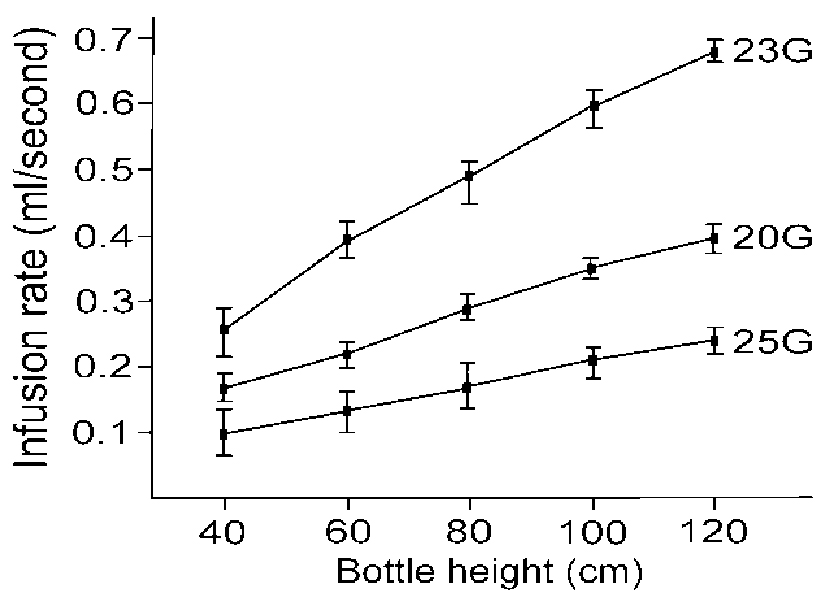
Fig. 4 Comparison among the infusion rates of balanced saline solution for 20-, 23- and 25-gauge infusion cannulas. The overall average infusion rate of the 23-gauge cannula was 1.7- and 2.8-fold greater than that of the 20- and 25-gauge cannulas, respectively.
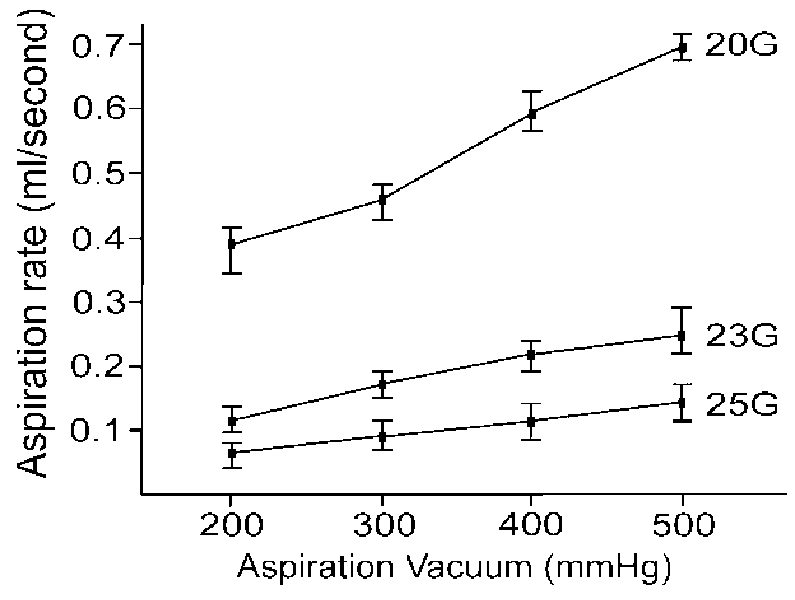
Fig. 5 Comparison among the aspiration rates of balanced saline solution for 20-, 23- and 25-gauge ocutomes. The overall average aspiration rate of the 20-gauge ocutome was 3.2- and 5.9-fold greater than that of the 23- and 25-gauge ocutomes, respectively. The average aspiration rate of the 23-gauge ocutome was 1.9-fold greater than that of the 25-gauge ocutome.
Cited by 2 articles
-
Partial Fluid-Air-Exchange at the End of 23 Gauge Sutureless Vitrectomy to Prevent Postoperative Hypotony
Myun Ku, Hee Jin Sohn, Dae Yeong Lee, Dong Heun Nam
J Korean Ophthalmol Soc. 2009;50(3):359-364. doi: 10.3341/jkos.2009.50.3.359.Comparison of Intraocular Pressure Between Sutureless and Sutured 23-gauge Vitrectomy
Hyung Jung Kim, Sojin Hong, Young Sook Park, Joon Hong Sohn
J Korean Ophthalmol Soc. 2010;51(6):835-841. doi: 10.3341/jkos.2010.51.6.835.
Reference
-
1. Fujii GY, De Juan E Jr, Humayun MS, et al. A new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgery. Ophthalmology. 2002. 109:1807–1812.2. Fujii GY, De Juan E Jr, Humayun MS, et al. Initial experience using the transconjunctival sutureless vitrectomy system for vitreoretinal surgery. Ophthalmology. 2002. 109:1814–1820.3. Eckardt C. Transconjunctival sutureless 23-gauge vitrectomy. Retina. 2005. 25:208–211.4. Yoon YH, Kim DS, Kim JG, Hwang JU. Sutureless vitreoretinal surgery using a new 25-gauge transconjunctival system. Ophthalmic Surg Lasers Imaging. 2006. 37:12–19.5. O' Reilly P, Beatty S. Transconjunctival sutureless vitrectomy: initial experience and surgical tips. Eye. 2007. 21:518–521.6. Lakhanpal RR, Humayun MS, de Juan E Jr, et al. Outcomes of 140 consecutive cases of 25-gauge transconjunctival surgery for posterior segment disease. Ophthalmology. 2005. 112:817–824.7. Ibarra MS, Hermel M, Prenner JL, Hassan TS. Longer-term outcomes of transconjunctival sutureless 25-gauge vitrectomy. Am J Ophthalmol. 2005. 139:831–836.8. Hwang J, Yoon YH, Kim D, Kim J. Combined phacoemulsification, foldable intraocular lens implantation, and 25-gauge transconjunctival sutureless vitrectomy. J Cataract Refract Surg. 2006. 32:727–731.9. Kellner L, Wimpissinger B, Stolba U, et al. 25 Gauge versus 20 Gauge System for Pars Plana Vitrectomy: A Prospective Randomized Clinical Trial. Br J Ophthalmol. 2007. 91:945–948.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Initial Experience With 20-Gauge Transconjunctival Sutureless Vitrectomy Using Conventional Instruments
- A Combination of 23-gauge and 20-gauge Transconjunctival Sutureless Vitrectomy
- A Case of Endophthalmitis after 25-gauge Transconjunctival Sutureless Vitrectomy
- A Case of Acute Endophthalmitis After 23-gauge Transconjunctival Sutureless Vitrectomy
- Comparison of Intraocular Pressure Between Sutureless and Sutured 23-gauge Vitrectomy
