Correction of Lower Lid Retraction Combined with Entropion using an Ear Cartilage Graft in the Anophthalmic Socket
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea. khwarg@snu.ac.kr
- 2Artificial Eye Center of Clinical Research Institute, Seoul National University Hospital, Seoul, Korea.
- 3Seoul National University Boramae Hospital, Seoul, Korea.
- KMID: 754418
- DOI: http://doi.org/10.3341/kjo.2005.19.3.161
Abstract
- PURPOSE
To investigate the surgical results of an ear cartilage graft and supplemental procedures for correcting lower lid retraction combined with entropion in anophthalmic patients. METHODS: We reviewed retrospectively the medical records of 7 anophthalmic patients with lower lid retraction and entropion, who received a posterior lamellar ear cartilage graft and one or both of lateral tarsal strip or eyelash-everting procedure between March 1998 and March 2003. Preoperative and postoperative lid and socket statuses were also investigated. RESULTS: Ear cartilage grafts were performed in all 7 patients, lateral tarsal strips in 6, and eyelash-everting procedures in 5. Postoperative follow-up durations ranged from 4 to 28 months (average 12.6 months). Retractions were corrected during follow-up in all patients. There were no cases of entropion immediately after surgery. However, the eyelashes of the lower lid returned to an upright position in 4 patients, but not so severe as to touch the ocular prosthesis, and thus did not require surgical correction during follow up. CONCLUSIONS: Lower lid retraction combined with entropion in anophthalmic patients can be corrected effectively using an ear cartilage graft with selective, supplemental procedures.
Keyword
MeSH Terms
Figure
-
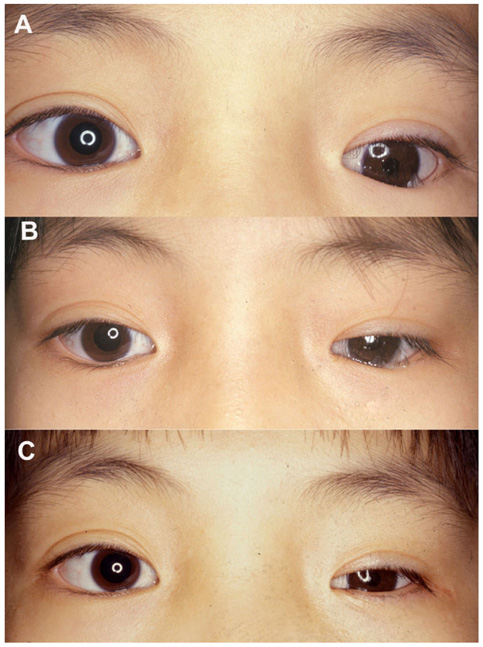
Fig. 1 An 11-year-old girl with congenital anophthalmos in the left eye (case 2). (A) At her initial visit to Our clinic, she had been wearing a thick ocular prosthesis for 36 months. Lower lid retraction combined With entropion was observed in the left side. Note mild enophthalmos and the lower eyelash touching the Ocular prosthesis. (B) Just before eyelid surgery and 6 months after enucleation and porous polyethylene Orbital implantation. Enophthalmos was corrected, but lower lid retraction combined with Entropion persisted. (C) Six months after surgical correction of lower lid retraction combined with entropion with ear cartilage graft, lateral tarsal strip, and tarsal suturing of subciliary subcutaneous tissue into the lower tarsus. Retraction and Entropion of the lower eyelid were well corrected.
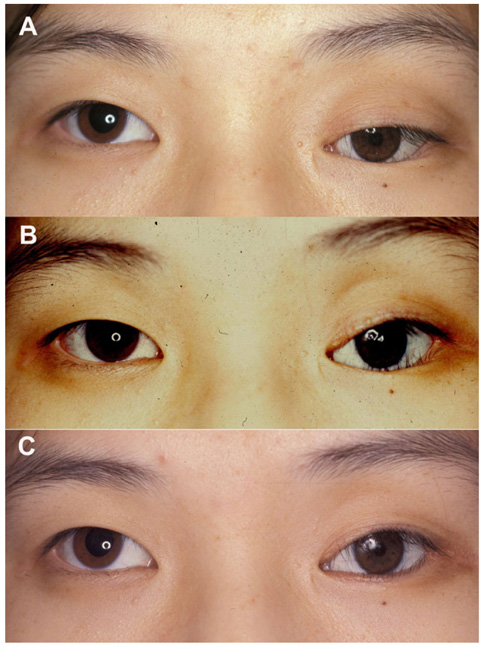
Fig. 2 A 19-year-old woman with an enucleated left eye due to retinoblastoma (case 5). (A) At her initial visit to our clinic, upper lid ptosis, enophthalmos, and lower lid retraction combined with entropion were noticed on the left side. (B) Six months after removing an implanted Allen sphere and a large subconjunctival cyst and porous polyethylene implantation prior to eyelid operation. (C) Four months after an ear cartilage graft, lateral tarsal strip and an eyelash-everting procedure, the lower lid retraction had been corrected, even though lower lid entropion persisted. However, this did not touch the prosthesis surface and did not require surgical correction.

Fig. 3 Harvested ear cartilage was placed in the space between the inferior border of the lower tarsus and the recessed lower retractor and conjunctiva, and sutured using 6-0 polyglactin.
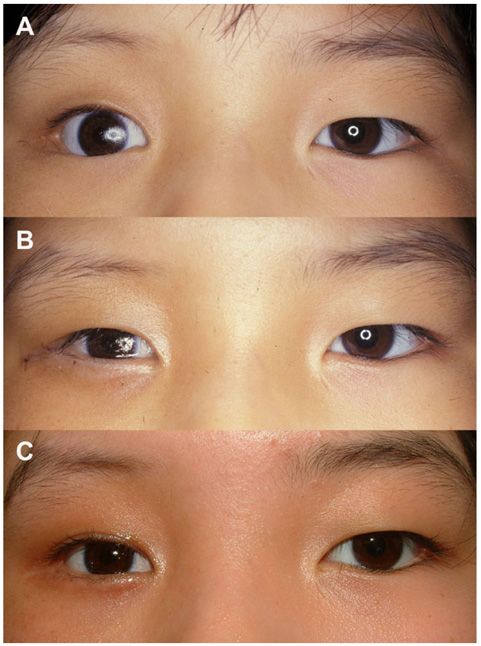
Fig. 4 A 9-year-old girl with an enucleated right eye due to retinoblastoma, who had been wearing an ocular prosthesis for 75 months (case 3). This patient had received orbital radiotherapy. (A) At her initial visit to our clinic, lower lid retraction with entropion and enophthalmos were observed on the right side. (B) One week after an ear cartilage. (C) Twenty-eight months after her surgery this correction was main graft and lateral tarsal strip. Separate eyelash-everting procedures were not performed, as lower lid retraction and entropion were corrected by the ear cartilage graft and lateral tarsal striptained.
Cited by 1 articles
-
Correction of Lower Lid Retraction Using Autologous Ear Cartilage Graft
Changho Yoon, Namju Kim, Min Joung Lee, Hokyung Choung, Min Seop Pahn, Sang In Khwarg
J Korean Ophthalmol Soc. 2011;52(2):136-140. doi: 10.3341/jkos.2011.52.2.136.
Reference
-
1. Vistnes LM. Mechanism of upper lid ptosis in the anophthalmic orbit. Plast Reconstr Surg. 1976. 58:539–545.2. Schaefer DP. Nesi FA, Lisman RD, Levine MR, editors. Evaluation and management of the anophthalmic socket and socket reconstruction. Smith's Ophthalmic Plastic and Reconstructive Surgery. 1998. 2nd ed. St. Louis: Mosby;chap. 58.3. Soll DB, Soll SM, Asbell RL. Nesi FA, Lisman RD, Levine MR, editors. Evolution and current concepts in the treatment of the anophthalmic socket. Smith's Ophthalmic Plastic and Reconstructive Surgery. 1998. 2nd ed. St. Louis: Mosby;chap. 57.4. Baylis HI, Perman KI, Fett DR, Sutcliffe RT. Autogenous auricular cartilage grafting for lower eyelid retraction. Ophthal Plast Reconstr Surg. 1985. 1:23–27.5. Vistnes LM, Iverson RE, Laub DR. The anophthalmic orbit: surgical correction of lower eyelid ptosis. Plast Reconstr Surg. 1973. 52:346–351.6. Wiggs EO, Guibor P, Hecht SD, Wolfley DE. Surgical treatment of the denervated or sagging lower lid. Ophthalmology. 1982. 89:428–432.7. Anderson RL. Tarsal strip procedure for correction of eyelid laxity and canthal malposition in the anophthalmic socket. Ophthalmology. 1981. 88:895–903.8. Anderson RL, Gordy DD. The tarsal strip procedure. Arch Ophthalmol. 1979. 97:2192–2196.9. Gardner TA, Kennerdell JS, Buerger GF. Treatment of dysthyroid lower lid retraction with autogenous tarsus transplants. Ophthal Plast Reconstr Surg. 1992. 8:26–31.10. Mommaerts MY, De Riu G. Prevention of lid retraction after lower lid blepharoplasties: an overview. J Craniomaxillofac Surg. 2000. 28:189–200.11. Patipa M, Patel BC, McLeish W, Anderson RL. Use of hard palate grafts for treatment of postsurgical lower eyelid retraction: a technical overview. J Craniomaxillofac Trauma. 1996. 2:18–28.12. Marks MW, Argenta LC, Friedman RJ, Hall JD. Conchal cartilage and composite grafts for correction of lower lid retraction. Plast Reconstr Surg. 1989. 83:629–635.13. Doxanas MT, Dryden RM. The use of sclera in the treatment of dysthyroid eyelid retraction. Ophthalmology. 1981. 88:887–894.14. Cohen MS, Shorr N. Eyelid reconstruction with hard palate mucosa grafts. Ophthal Plast Reconstr Surg. 1992. 8:183–195.15. Kersten RC, Kulwin DR, Levartovsky S, et al. Management of lower-lid retraction with hard-palate mucosa grafting. Arch Ophthalmol. 1990. 108:1339–1343.16. Millman AL, Katzen LB, Putterman AM. Cicatricial entropion; An analysis of its treatment with transverse blepharotomy and marginal rotation. Ophthalmic Surg. 1989. 20:575–579.17. Rizk SN, Mishra AK. Surgical correction of senile entropion of the lower lid with fascia lata sling. Br J Ophthalmol. 1979. 63:117–119.18. Tenzel RR, Miller GR, Rubenzik R. Cicatricial upper lid entropion. Treated with banked scleral graft. Arch Ophthalmol. 1975. 93:999–1000.19. Matsuo K, Hirose T. The use of conchal cartilage graft in involutional entropion. Plast Reconstr Surg. 1990. 86:968–970.20. Bartley GB, Kay PP. Posterior lamellar eyelid reconstruction with a hard palate mucosal graft. Am J Ophthalmol. 1989. 107:609–612.21. Karesh JW, Fabrega MA, Rodrigues MM, Glaros DS. Polytetrafluoroethylene as an interpositional graft material for the correction of lower eyelid retraction. Ophthalmology. 1989. 96:419–423.22. Woo KI, Yi KY, Kim YD. Surgical correction for lower lid epiblepharon in Asians. Br J Ophthalmol. 2000. 84:1407–1410.23. Choung HK, Khwarg SI. Epiblepharon of the lower eyelid; technique of surgical repair and quantification of excision according to the skin fold height. Ophthalmic Surgery and Lasers. 2002. 33:280–287.24. Quickert MH, Rathbun E. Suture repair of entropion. Arch Ophthalmol. 1971. 85:304–305.25. Baylis HI, Rosen N, Neuhaus RW. Obtaining auricular cartilage for reconstructive surgery. Am J Ophthalmol. 1982. 93:709–712.26. Nowinski T, Anderson RL. Advances in eyelid malpositions. Ophthal Plast Reconstr Surg. 1985. 1:145–148.27. Nolan WB III, Vistnes LM. Correction of lower eyelid ptosis in the anophthalmic orbit; a long-term follow-up. Plast Reconstr Surg. 1983. 72:289–292.28. Zbylski JR, LaRossa DD, Rich JD. Correction of lower eyelid ptosis in the anophthalmic orbit with an autogenous ear cartilage graft. Plastic Reconstr Surg. 1978. 61:220–223.29. Small RG, Scott M. The tight retracted lower eyelid. Arch Ophthalmol. 1990. 108:438–444.30. Migliori ME. Bosniak SL, editor. Evaluation and Management of the Anophthalmic Socket. Principles and Practice of Ophthalmic Plastic and Reconstructive Surgery. 1996. 1st ed. Philadelphia: Saunders;chap. 106.31. Patel BC, Patipa M, Anderson RL, McLeish W. Management of postblepharoplasty lower eyelid retraction with hard palate grafts and lateral tarsal strip. Plast Reconstr Surg. 1997. 99:1251–1260.32. Wies FA. Spastic entropion. Trans Am Acad Ophthalmol Otolaryngol. 1955. 59:503–506.33. Lyon DB, Dortzbach RK. Dortzbach RK, editor. Entropion, trichiasis, and distichiasis. Ophthalmic Plastic Surgery. Prevention and Management of Complications. 1994. 1st ed. New York: Raven Press;chap. 2.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hard Palate Mucosa Grafts for Lower Lid Retraction
- Acellular Dermal Allograft for the Correction of Eyelid Retraction
- Correction of Lower Lid Retraction Using Autologous Ear Cartilage Graft
- Anophthalmic Conjunctival Sac Reconstruction using Acellular Dermal Allograft
- Surgical Correction of Lower Lid Retraction Using The Scleral Spacer
