Treatment of Internal Carotid Artery Dissections with Endovascular Stent Placement: Report of Two Cases
- Affiliations
-
- 1Univ Ulsan,Kangnung Hosp Coll Med Dept Diagnost Radiol,415 Bandong Ri/Kangnung si 210711, Kangwon do, South Korea.
- KMID: 754123
- DOI: http://doi.org/10.3348/kjr.2001.2.1.52
Abstract
- Extracranial carotid artery dissection may manifest as arterial stenosis or occlusion, or as dissecting aneurysm formation. Anticoagulation and/or antiplatelet therapy is the first-line treatment, but because it is effective and less invasive than other procedures, endovascular treatment of carotid artery dissection has recently attracted interest. We encountered two consecutive cases of traumarelated extracranial internal carotid artery dissection, one in the suprabulbar portion and one in the subpetrosal portion. We managed the patient with suprabulbar dissection using a self-expandable metallic stent and managed the patient with subpet-rosal dissection using a balloon-expandable metallic stent. In both patients the dissecting aneurysm disappeared, and at follow-up improved luminal patency was observed.
Keyword
MeSH Terms
Figure
-
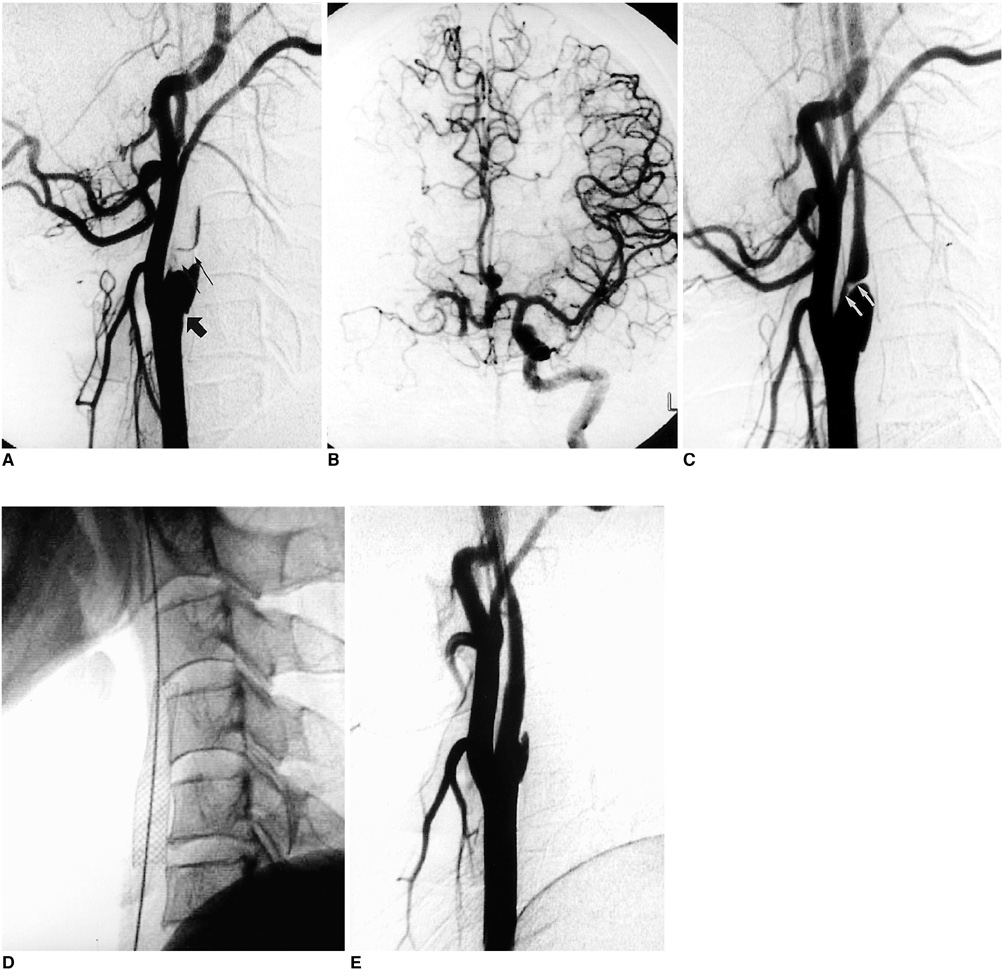
Fig. 1 Case 1 A. Lateral angiogram of right common carotid artery shows occlusion of its proximal internal branch. Focal dimpling (black arrow) of the posterior aspect indicates partial filling of false lumen by thrombus (small arrows). Distal true lumen has collapsed, with linear filling by contrast media. B. Left internal carotid angiogram shows complete occlusion of proximal segment of right middle cerebral artery, suggesting thromboembolic occlusion. C. Follow-up angiogram obtained 20 days after initial angiography shows partial recanalization of true lumen. A thick dissecting flap is present (arrows) and the dilated false lumen persists. D. Angioplasty was performed 35 days after injury, and a self-expandable metallic stent is seen. E. After angioplasty using a stent, true lumen regained its original diameter. The false lumen, now smaller, may be observed behind the stent. Thirty-five days after stent placement, patency was assessed with CT and the false lumen was no longer visible (not shown).
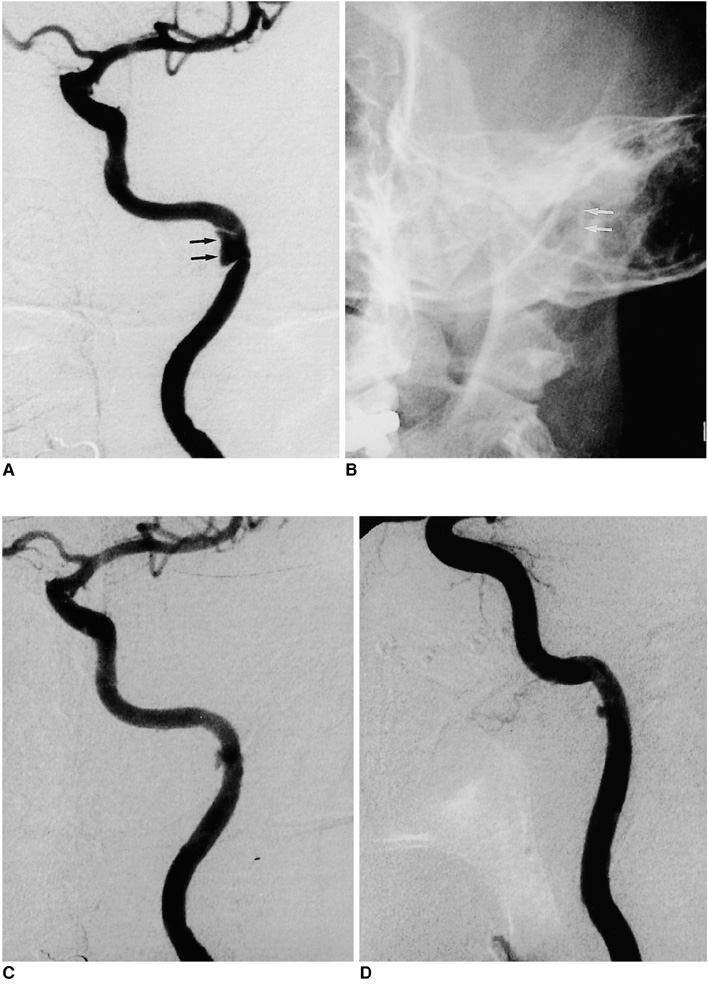
Fig. 2 Case 2 A. Initial angiogram of left internal carotid artery demonstrates a focal stenosis of the subpetrosal portion of the artery, associated with a dissecting aneurysm (arrows). The aneurysmal sac is restricted by the bony canal of that portion. B. A balloon-expandable stent was inserted, but is barely visible due to the relatively poor radiopacity and surrounding bony structures. C. Luminal patency of the dissected segment is improved substantially after stent placement, and the aneurysmal sac is much smaller. D. Follow-up angiography was performed 65 days after stent placement. The arterial lumen is well preserved, though the aneurysmal sac is still partly filled. After stent placement, the patient was asymptomatic.
Reference
-
1. Anson J, Crowell RM. Cervicocranial arterial dissection. Neurosurgery. 1991. 29:89–96.2. Lucas C, Moulin T, Deplanque D, et al. Stroke patterns of internal carotid artery dissection in 40 patients. Stroke. 1998. 29:2646–2648.3. Mulloy JP, Flick PA, Gold RE. Blunt carotid injury: a review. Radiology. 1998. 207:571–585.4. Bejjani GK, Monsein LH, Laird JR, et al. Treatment of symptomatic cervical carotid dissections with endovascular stents. Neurosurgery. 1999. 44:755–760.5. Simionato F, Righi C, Scotti G. Post-traumatic dissecting aneurysm of extracranial internal carotid artery: endovascular treatment with stenting. Neuroradiology. 1999. 41:543–547.6. DeOcampo J, Brillman J, Levy DI. Stenting: a new approach to carotid dissection. J Neuroimaging. 1997. 7:187–190.7. Bernstein SM, Coldwell DM, Prall JA, Brega KE. Treatment of traumatic carotid pseudoaneurysm with endovascular stent placement. J Vasc Interv Radiol. 1997. 8:1065–1068.8. Coric D, Wilson JA, Regan JD, Bell A. Primary stenting of the extracranial internal carotid artery in a patient with multiple cervical dissections: technical case report. Neurosurgery. 1998. 43:956–959.9. Horowitz MB, Miller G III, Meyer Y, Carstens G III, Purdy PD. Use of intravascular stents in the treatment of internal carotid and extracranial vertebral artery pseudoaneurysms. AJNR. 1996. 17:693–696.10. Klein GE, Szolar DH, Raith J, et al. Post-traumatic extracranial aneurysm of the internal carotid artery: combined endovascular treatment with coils and stents. AJNR. 1997. 18:1261–1264.11. Chalmers RT, Brittenden J, Bradbury AW. The use of endovascular stented grafts in the management of traumatic false aneurysms: a caveat. J Vasc Surg. 1995. 22:337–338.12. Biousse V, D'Anglejan-Chatillon J, Touboul P, Amarenco P, Bousser M. Time course of symptoms in extracranial carotid artery dissections. Stroke. 1995. 26:235–239.13. Fabian TC, Patton JH Jr, Croce MA, et al. Blunt carotid injury: importance of early diagnosis and anticoagulation therapy. Ann Surg. 1996. 223:513–525.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stent Angioplasty for Intracranial Vertebral Dissections: Single Stent versus Double Stent Placement
- Supra-aortic Arterial Recanalization: Report of 5 cases
- Endovascular Treatment with a Stent-Graft for Internal Carotid Artery Laceration during Trans Sphenoidal Surgery: A Case Report
- How to Escape Stentriever Wedging in an Open-cell Carotid Stent during Mechanical Thrombectomy for Tandem Cervical Internal Carotid Artery and Middle Cerebral Artery Occlusion
- Endovascular Treatment Using Multiple Stents for Symptomatic Intracranial Vertebral Artery Dissecting Aneurysm
