MR Imaging and Histopathologic Findings of A Case of Cerebral Ganglioneurocytoma
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. hkkee2@amc.seoul.kr
- 2Department of Neurosurgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 754065
- DOI: http://doi.org/10.3348/kjr.2002.3.3.214
Abstract
- We report a case of ganglioneurocytoma manifesting as a complex partial seizure in a young adult male. MR images depicted a well-marginated cystic mass with a heterogeneous solid portion abutting the dura in the parietal lobe. The solid portion showed minimal heterogeneous enhancement, and pressure erosion of the overlying calvarium had occurred. Following gross total resection, the clinical outcome was satisfactory, with no further seizures, and during the five-year follow-up period, the tumor did not recur.
Keyword
MeSH Terms
Figure
-
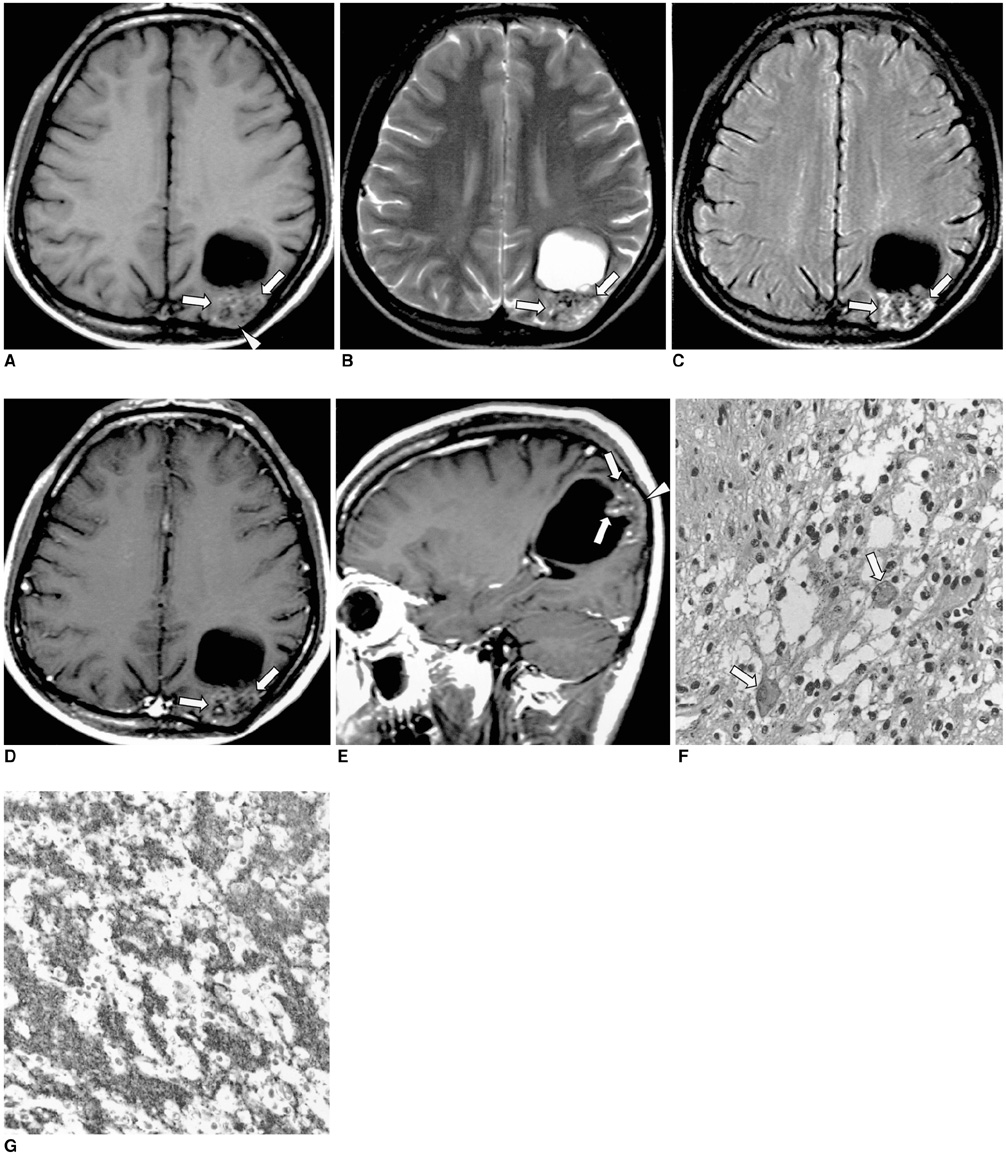
Fig. 1 A 23-year-old man with a longstanding history of seizure. A. T1-weighed (490/14) axial MR image depicts a large thin-walled cyst, isointense to CSF, in left parietal lobe white matter. The solid portion (arrows), located in the cortex, shaws relatively well-defined, heterogeneous mixed signal intensity. Erosion of the overlying calvarium (arrowhead) has occurred. B. In this T2-weighted (3500/99) axial MR image, the cystic portion isointense to CSF shows high signal intensity, while the solid portion shows heterogeneous high signal intensity (arrows). C. FLAIR (9999/119) image more clearly demonstrates the heterogeneous high signal intensity of the solid portion (arrows). D, E. Contrast-enhanced T1-weighed (490/14) axial (D) and sagittal (E) MR images show minimal enhancement of the solid portion (arrows). F. Photomicrograph (H & E staining, ×200) depicts ganglionic cells (arrows) among the small round cells. G. Photomicrograph (synaptophysin staining, ×200) reveals tumor cells embedded in a neurophil-like fibrillary background which is strongly immunoreactive for synaptophysin.
Reference
-
1. Funato H, Inoshita N, Okeda R, Yamamoto S, Aoyagi M. Cystic ganglioneurocytoma outside the ventricular region. Acta Neuropathol. 1997. 94:95–98.2. Nishio S, Takeshita I, Fukui M. Primary cerebral ganglioneurocytoma in an adult. Cancer. 1990. 66:358–362.3. Shimada H. Transmission and scanning electron microscopic studies on the tumors of neuroblastoma group. Acta Pathol Jpn. 1982. 32:415–426.4. Chang KH, Han MH, Kim DG, et al. MR appearance of central neurocytoma. Acta Radiol. 1993. 34:520–526.5. Nishio S, Tashima T, Takeshita I, Fukui M. Intraventricular neurocytoma: clinicopathological features of six cases. J Neurosurg. 1988. 68:665–670.6. Chan A, McAbee G, Queenan J, Manning A. Ganglioneurocytoma mimicking a malignant tumor: case report with a literature review of the MRI appearance of neurocytomas and gangliogliomas. J Neuroimaging. 2001. 11:47–50.7. Biernat W, Zakrzewski K, Liberski PP. Twelve-year-old boy with recent onset seizures. Brain Pathol. 2000. 10:313–314. 3198. von Deimling A, Janzer R, Kleihues P, Wiestler OD. Patterns of differentiation in central neurocytoma: an immunohistochemical study of eleven biopsies. Acta Neuropathol. 1990. 79:473–479.9. Castillo M, Davis PC, Takei Y, Hoffman JC Jr. Intracranial ganglioglioma: MR, CT, and clinical findings in 18 patients. Am J Neuroradiol. 1990. 11:109–114.10. Kim HS, Lee HK, Jeong AK, Shin JH, Choi CG, Khang SK. Supratentorial gangliocytoma mimicking extra-axial tumor: a report of two cases. Korean J Radiol. 2001. 2:108–112.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- MR Imaging of Focal Cervical Edema Mimicking Carcinoma: A Case Report
- MR Angiography in Hydranencephaly: Case Report
- Intraventricular Anaplastic Hemangiopericytoma: CT and MR Imaging Findings
- Undifferentiated Embryonal Sarcoma of Liver in Child
- Gd-DTPA Eenhanced IVIRI of the Cerebral Venous Angiomas: Cornparision with Cerebral Angiography
