Newly Designed Sheaths for Gastroduodenal Intervention: An Experimental Study in a Phantom and Dogs
- Affiliations
-
- 1Department of Radiology Asan Medical Center, University of Ulsan College of Medicine. hysong@www.amc.seoul.kr
- 2Department of Radiology, Gachon Medical School, Gil Medical Center.
- 3Department of Biomedical Engineering, Asan Medical Center, University of Ulsan College of Medicine.
- KMID: 753991
- DOI: http://doi.org/10.3348/kjr.2004.5.2.114
Abstract
OBJECTIVE
To evaluate the usefulness of newly designed sheaths for gastroduodenal intervention in a gastric phantom and dogs. MATERIALS AND METHODS: A regular sheath was made using a polytetrafluoroethylene tube (4 mm in diameter, 90 cm long) with a bent tip (4 cm long, 100 degree angle). For the supported type of sheath, a 5 Fr catheter was attached to a regular sheath to act as a side lumen. To evaluate their supportability, we measured the distance of movement of the sheath's tip within a silicone gastric phantom for three types of sheath, the regular type, supported type, and supported type with a supporting guide wire. The experiments were repeated 30 times, and the results were analyzed using ANOVA with the postHoc test. In addition, an animal experiment was performed in six mongrel dogs (total: 12 sessions) to evaluate the torque and supportability of the sheaths in the stomach, while pushing a guide wire or coil catheter under fluoroscopic guidance. RESULTS: In the guide wire application, the distances of movement of the sheath tip in the three types of sheath, the regular type, supported type, and supported type with supporting guide wire, were 8.40+/-0.51 cm, 6.23+/-0.41 cm, and 4.47+/-0.32 cm, respectively (p < 0.001). In the coil catheter application, the corresponding values were 7.22+/-0.70 cm, 5.61+/-0.31 cm and 3.91+/-0.59 cm, respectively (p < 0.001). All three types of sheath rotated smoothly and enabled both the wires and catheters to be guided toward the pylorus of the dog in all cases. CONCLUSION: The newly designed sheaths can be useful for gastroduodenal intervention.
MeSH Terms
Figure
-
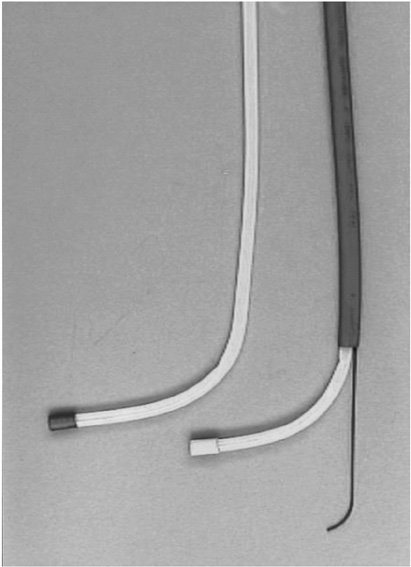
Fig. 1 A regular sheath (left) and supported sheath with a supporting wire in the side lumen (right).
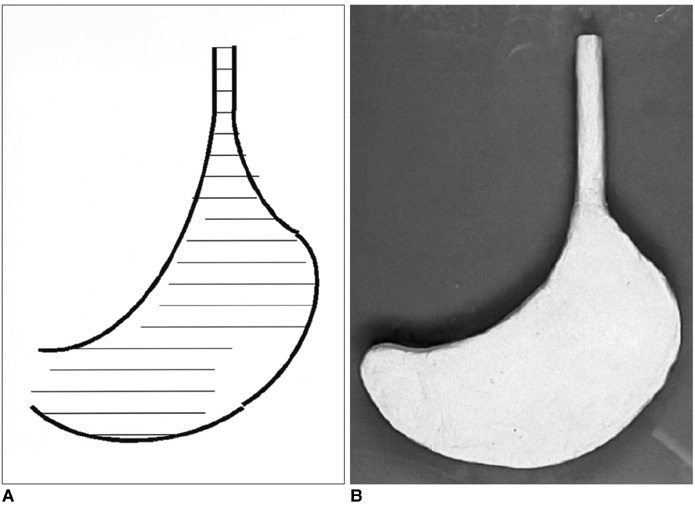
Fig. 2 A. An outline of the stomach was drawn, in order to make the gastric phantom, as follows. The distances from the greater to lesser curvature were measured in each section on the abdominal CT scan. The locations of the greater curvature on one section relative to that on the next section on the abdominal CT scan were also evaluated. Both the distances and relative locations were plotted on a 2-dimensional plane; subsequently, the contour of the greater and lesser curvature of the stomach was drawn by connecting these points on a 2-dimensional plane. The esophageal outline was drawn from the esophagus to the cardia, with a diameter of 2 cm and a length of 5 cm. B. Clay was shaped, so as to be 2 cm in height, and to follow the gastric contour with a tubular shape at the esophageal portion.
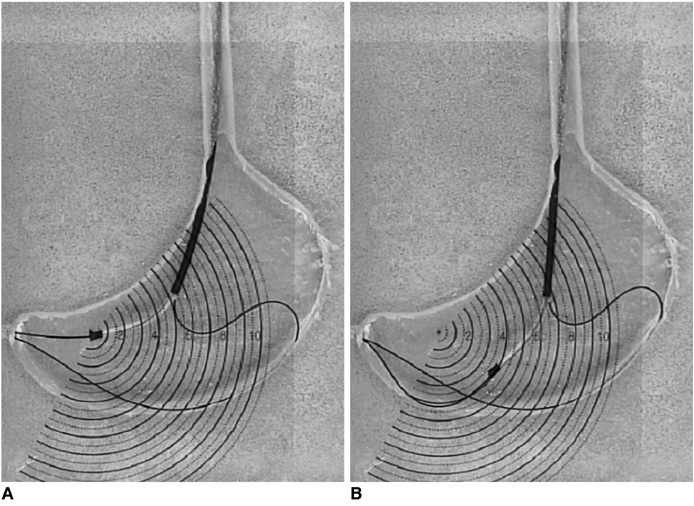
Fig. 3 A. A guide wire is inserted in a supported sheath, and a supporting wire is inserted into the gastric portion through the side lumen. When the supporting wire is pushed, the tip of the wire is pressed against the greater curvature side of the gastric phantom. B. The distance of movement of the tip of the supported sheath from the central point was measured while pushing the guide and supporting wire, and was found to be approximately 4 cm.
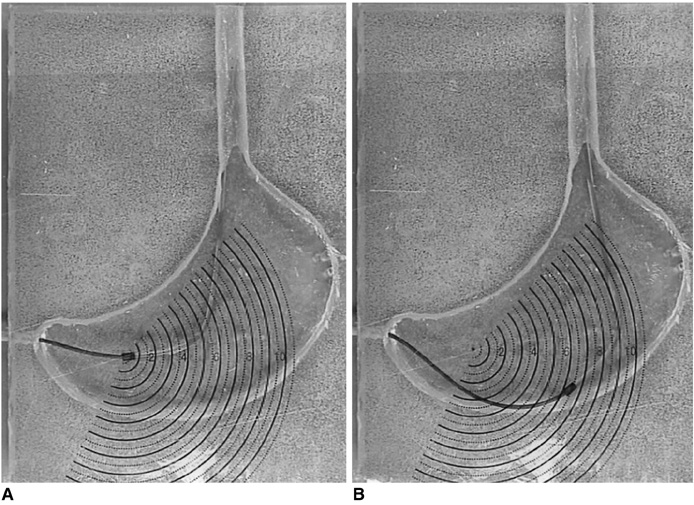
Fig. 4 A. A regular sheath is inserted into the gastric portion via the esophageal portion, and a coil catheter is advanced beyond the pyloric portion. B. The distance between the central point and point of the tip of the sheath is approximately 6 cm.

Fig. 5 Experimental study in dogs. While pushing a coil catheter through the sheath, the direction is changed from the long axis of the esophagus to the transverse axis oriented toward the pylorus in the stomach. The coil catheter is then advanced to the pylorus with support from the sheath, without any kinking occurring in the stomach.
Reference
-
1. Lindor KD, Ott BJ, Hughes RW Jr. Balloon dilatation of upper digestive tract strictures. Gastroenterology. 1985. 89:545–548.2. Jung GS, Song HY, Kang SG, et al. Malignant gastroduodenal obstructions: treatment by means of a covered expandable metallic stent-initial experience. Radiology. 2000. 216:758–763.3. Song HY, Yang DH, Kuh JH, Choi KC. Obstructing cancer of the gastric antrum: palliative treatment with covered metallic stents. Radiology. 1993. 187:357–358.4. Mauro MA, Koehler RE, Baron TH. Advances in gastrointestinal intervention: the treatment of gastroduodenal and colorectal obstructions with metallic stents. Radiology. 2000. 215:659–669.5. Pinto IT. Malignant gastric and duodenal stenosis: palliation by peroral implantation of a self-expanding metallic stent. Cardiovasc Intervent Radiol. 1997. 20:431–434.6. McLean GK, Meranze SG. Interventional radiologic management of enteric strictures. Radiology. 1989. 170:1049–1053.7. McLean GK, Cooper GS, Hartz WH, Burke DR, Meranze SG. Radiologically guided balloon dilation of gastrointestinal strictures. Part I. Technique and factors influencing procedural success. Radiology. 1987. 165:35–40.8. McLean GK, Cooper GS, Hartz WH, Burke DR, Meranze SG. Radiologically guided balloon dilation of gastrointestinal strictures. Part II. Results of long-term follow-up. Radiology. 1987. 165:41–43.9. Holt PD, de Lange EE, Shaffer HA Jr. Strictures after gastric surgery: treatment with fluoroscopically guided balloon dilatation. AJR Am J Roentgenol. 1995. 164:895–899.10. Hegedus V, Raaschou HO. Radiologically guided dilatation of stenotic gastroduodenal anastomosis. Gastrointest Radiol. 1986. 11:27–29.11. Kozarek RA. Hydrostatic balloon dilation of gastrointestinal stenoses: a national survey. Gastrointest Endosc. 1986. 32:15–19.12. de Baere T, Harry G, Ducreux M, et al. Self-expanding metallic stents as palliative treatment of malignant gastroduodenal stenosis. AJR Am J Roentgenol. 1997. 169:1079–1083.13. Shin JH, He X, Lee JH, et al. Newly designed multifunctional coil catheter for gastrointestinal intervention: feasibility determined by experimental study in dogs. Invest Radiol. 2003. 38:796–801.14. Binkert CA, Jost R, Steiner A, Zollikofer CL. Benign and malignant stenoses of the stomach and duodenum: treatment with self-expanding metallic endoprostheses. Radiology. 1996. 199:335–338.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Balloon Sheaths for Gastrointestinal Guidance and Access: A Preliminary Phantom Study
- Understanding the Rome IV: Gastroduodenal Disorders
- The effect of newly designed toothbrush on plaque control, treatment of gingivitis and periodontitis
- Development of gastroduodenal self-expandable metallic stents: 30 years of trial and error
- Design of Multipurpose Phantom for External Audit on Radiotherapy
