Energy-dispersive X-ray spectroscopic investigation of a fractured non-submerged dental implant associated with abutment fracture
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea
- 2Oral and Maxillofacial Microvascular Reconstruction LAB, Brong Ahafo Regional Hospital, Sunyani, Ghana
- KMID: 2539703
- DOI: http://doi.org/10.5125/jkaoms.2023.49.1.43
Abstract
- The biocompatibility and durability of implant fixtures are major concerns for dentists and patients. Mechanical complications of the implant include abutment screw loosening, screw fracture, loss of implant prostheses, and implant fracture. This case report aims to describe management of a case of fixture damage that occurred after screw fracture in a tissue level, internal connection implant and microscopic evaluation of the fractured fixture. A trephine bur was used to remove the fixture, and the socket was grafted using allogeneic bone material. The failed implant was examined by scanning electron microscopy (SEM) and energy dispersive X-ray spectroscopy (EDS), which revealed a fractured fixture with both normal and irregular bone patterns. The SEM and EDS results give an enlightenment of the failed fixture surface micromorphology with microfracture and contaminated chemical compositions. Noticeably, the significantly high level of gold (Au) on the implant surface and the trace amounts of Au and titanium (Ti) in the bone tissue were recorded, which might have resulted from instability and micro-movement of the implant-abutment connection over an extended period of time. Further study with larger number of patient and different types of implants is needed for further conclusion.
Keyword
Figure
-

Fig. 1 Abutment of the implant was fractured at the same height level as the surrounding alveolar bone. A. A radiolucency was observed on the coronal portion of the fixture, indicating that the fixture body also was fractured (arrow). B. Axial computed tomography showed the location of the fracture at the mesiolingual aspect of the fixture body (arrows). C. The #37i fixture was retrieved with bony attachments after removal using a trephine bur.
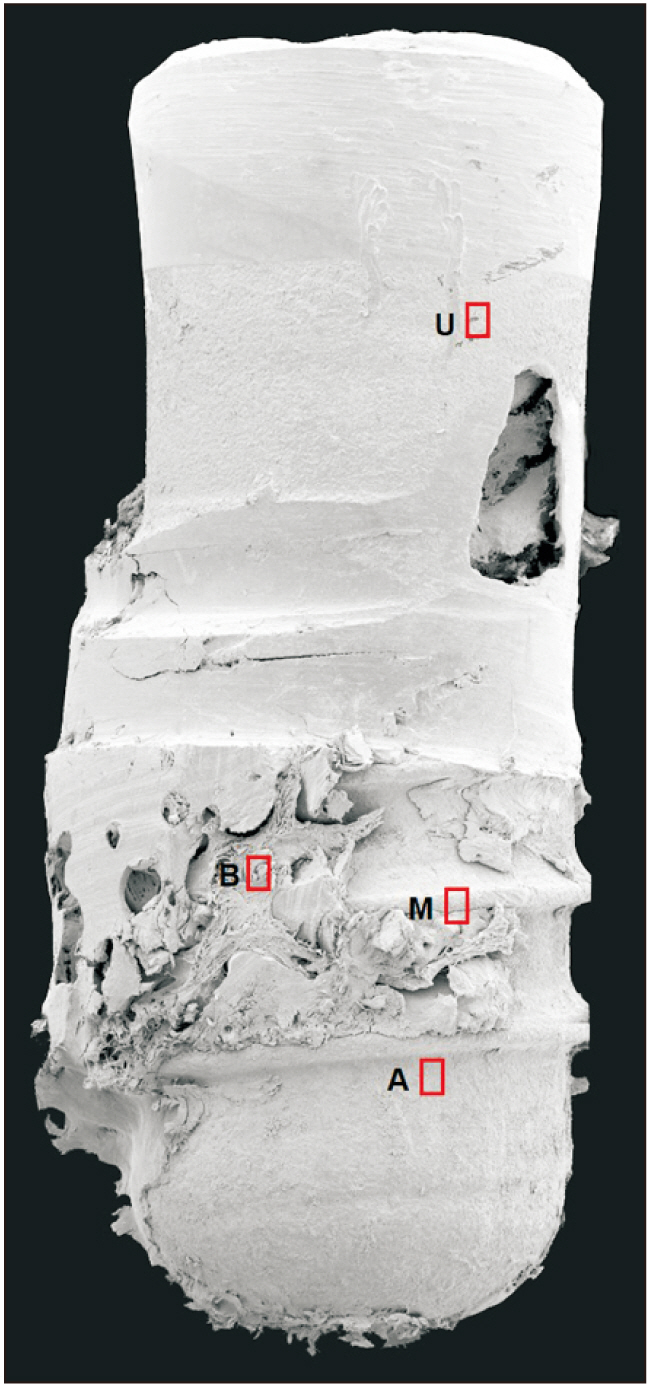
Fig. 2 Scanning electron microscopy photograph of the failed implant at ×65 magnification. The regions of interest examined by energy dispersive X-ray spectroscopy at ×10,000 magnifications are marked with red rectangles. U: surface in the upper area of the fixture, adjacent to the fracture region, M: implant surface at the middle of the implant fixture, B: attached bone tissue in the middle region of the fixture, A: implant surface in the apical region of the implant.

Fig. 3 Scanning electron microscopy-energy dispersive X-ray spectroscopy (SEM-EDS) analysis of the failed implant. SEM micrograph at ×500 and ×10,000 magnifications, EDS elemental distribution map, and spectrum of representative points on the failed implants. U: microfracture (white arrowheads) and scratching lines (black arrows) are observed. The elemental distribution map showed a homogeneous oxidized Ti surface with particles composed of C and Si. M: normal bone structure with bony lacunae covering the fixture surface (blue arrowheads). The Ti surface was detected on EDS in the region with a thin bone layer (black arrowheads). B: SEM images showing irregular bone structure with the presence of organic matter (blue arrowheads). EDS results reveal the presence of Na, F, N, Si, and Au. A: normal bone structure with lacunae covering the fixture surface (blue arrowheads). Trace amounts of Ti can be observed in the elemental distribution map (black arrowheads). (cps/eV: count per second per electron-volt)
Reference
-
References
1. Albrektsson T, Zarb G, Worthington P, Eriksson AR. 1986; The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants. 1:11–25. PMID: 3527955.2. Berglundh T, Persson L, Klinge B. 2002; A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J Clin Periodontol. 29 Suppl 3:197–212. discussion 232–3. https://doi.org/10.1034/j.1600-051x.29.s3.12.x. DOI: 10.1034/j.1600-051X.29.s3.12.x. PMID: 12787220.3. Rangert B, Krogh PH, Langer B, Van Roekel N. 1995; Bending overload and implant fracture: a retrospective clinical analysis. Int J Oral Maxillofac Implants. 10:326–34. PMID: 7615329.4. Balshi TJ. 1996; An analysis and management of fractured implants: a clinical report. Int J Oral Maxillofac Implants. 11:660–6. PMID: 8908866.5. Singh A, Singh A, Vivek R, Chaturvedi TP, Chauhan P, Gupta S. 2013; SEM analysis and management of fracture dental implant. Case Rep Dent. 2013:270385. https://doi.org/10.1155/2013/270385. DOI: 10.1155/2013/270385. PMID: 23710372. PMCID: PMC3655462.6. Sánchez-Pérez A, Moya-Villaescusa MJ, Jornet-Garcia A, Gomez S. 2010; Etiology, risk factors and management of implant fractures. Med Oral Patol Oral Cir Bucal. 15:e504–8. https://doi.org/10.4317/medoral.15.e504. DOI: 10.4317/medoral.15.e504. PMID: 20038899.7. Wee K, Lee BA. 2019; Implant fracture after screw fracture in a tissue-level implant: a case report. Implantology. 23:229–34. https://doi.org/10.32542/implantology.2019020. DOI: 10.32542/implantology.2019020.8. Delgado-Ruiz R, Romanos G. 2018; Potential causes of titanium particle and ion release in implant dentistry: a systematic review. Int J Mol Sci. 19:3585. https://doi.org/10.3390/ijms19113585. DOI: 10.3390/ijms19113585. PMID: 30428596. PMCID: PMC6274707.9. Hellsing M. 1997; Comparative surface analysis of four dental implant systems. J Dent Assoc S Afr. 52:399–402. PMID: 9461954.10. Sawase T, Hai K, Yoshida K, Baba K, Hatada R, Atsuta M. 1998; Spectroscopic studies of three osseointegrated implants. J Dent. 26:119–24. https://doi.org/10.1016/s0300-5712(96)00080-2. DOI: 10.1016/S0300-5712(96)00080-2. PMID: 9540308.11. Shibli JA, Marcantonio E, dʼAvila S, Guastaldi AC, Marcantonio E Jr. 2005; Analysis of failed commercially pure titanium dental implants: a scanning electron microscopy and energy-dispersive spectrometer x-ray study. J Periodontol. 76:1092–9. https://doi.org/10.1902/jop.2005.76.7.1092. DOI: 10.1902/jop.2005.76.7.1092. PMID: 16018751.12. Romeed SA, Malik R, Dunne SM. 2013; Marginal bone loss influence on the biomechanics of single implant crowns. J Craniofac Surg. 24:1459–65. https://doi.org/10.1097/SCS.0b013e3182902db0. DOI: 10.1097/SCS.0b013e3182902db0. PMID: 23851832.13. Jimbo R, Halldin A, Janda M, Wennerberg A, Vandeweghe S. 2013; Vertical fracture and marginal bone loss of internal-connection implants: a finite element analysis. Int J Oral Maxillofac Implants. 28:e171–6. https://doi.org/10.11607/jomi.3052. DOI: 10.11607/jomi.3052. PMID: 23869374.14. Shemtov-Yona K, Rittel D. 2014; Identification of failure mechanisms in retrieved fractured dental implants. Eng Fail Anal. 38:58–65. https://doi.org/10.1016/j.engfailanal.2014.01.002. DOI: 10.1016/j.engfailanal.2014.01.002.15. Apaza-Bedoya K, Tarce M, Benfatti CAM, Henriques B, Mathew MT, Teughels W, et al. 2017; Synergistic interactions between corrosion and wear at titanium-based dental implant connections: a scoping review. J Periodontal Res. 52:946–54. https://doi.org/10.1111/jre.12469. DOI: 10.1111/jre.12469. PMID: 28612506.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Removal of fractured implant screws: case report
- Repairment of abutment and abutment screw fracture in implant prosthesis: A case report
- Implant Fracture After Screw Fracture in a TissueLevel Implant: A Case Report
- Alternative Method to Salvage an Internally Damaged Implant using Cast Post
- Comparison of implant component fractures in external and internal type: A 12-year retrospective study
