J Yeungnam Med Sci.
2023 Jan;40(1):91-95. 10.12701/yujm.2021.01543.
Diagnosis and successful visual biofeedback therapy using fiberoptic endoscopic evaluation of swallowing in a young adult patient with psychogenic dysphagia: a case report
- Affiliations
-
- 1Department of Rehabilitation Medicine, Biomedical Research Institute, Pusan National University Hospital, Busan, Korea
- 2Department of Rehabilitation Medicine, Pusan National University School of Medicine, Busan, Korea
- KMID: 2538790
- DOI: http://doi.org/10.12701/yujm.2021.01543
Abstract
- Psychogenic dysphagia is a deglutition disorder characterized by a fear of swallowing, with no structural or functional causes. This report presents the case of a young male patient who had severe malnutrition due to psychogenic dysphagia and was provided visual biofeedback using fiberoptic endoscopic evaluation of swallowing (FEES). A healthy 25-year-old man presented to our clinic with a complaint of throat discomfort when swallowing that had started 6 months prior. As the symptoms worsened, he became fearful of food spreading to his lungs after swallowing and the development of respiratory difficulties. His food intake gradually decreased, resulting in a weight loss of 20 kg within 2 months. Evaluation of organic and other functional causes of dysphagia was performed, but no abnormalities were detected. The sensation of a lump in his throat, fear of swallowing, and anxiety were transformed into somatic symptoms. The patient was diagnosed with psychogenic dysphagia. After visual biofeedback by a physician who performed FEES, the patient resumed eating normally and increased his food intake. If routine tests do not reveal structural or functional causes of dysphagia, assessment of a psychogenic swallowing disorder should be considered. FEES can help in the diagnosis and management of psychogenic dysphagia.
Keyword
Figure
-
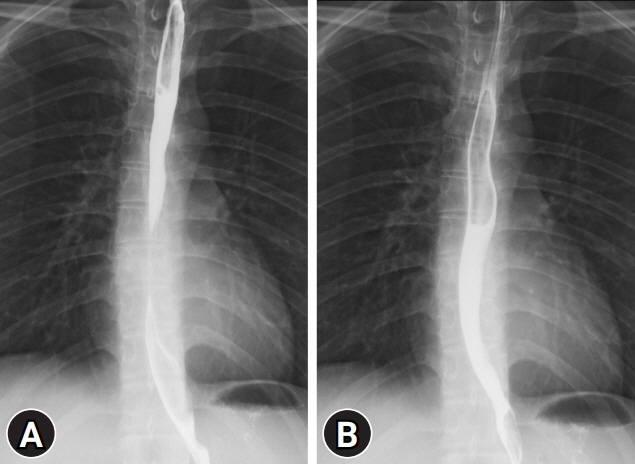
Fig. 1. Esophagography shows no structural abnormality or dysmotility from (A) the upper and middle thoracic esophagus to (B) the lower thoracic esophagus and esophagogastric junction.
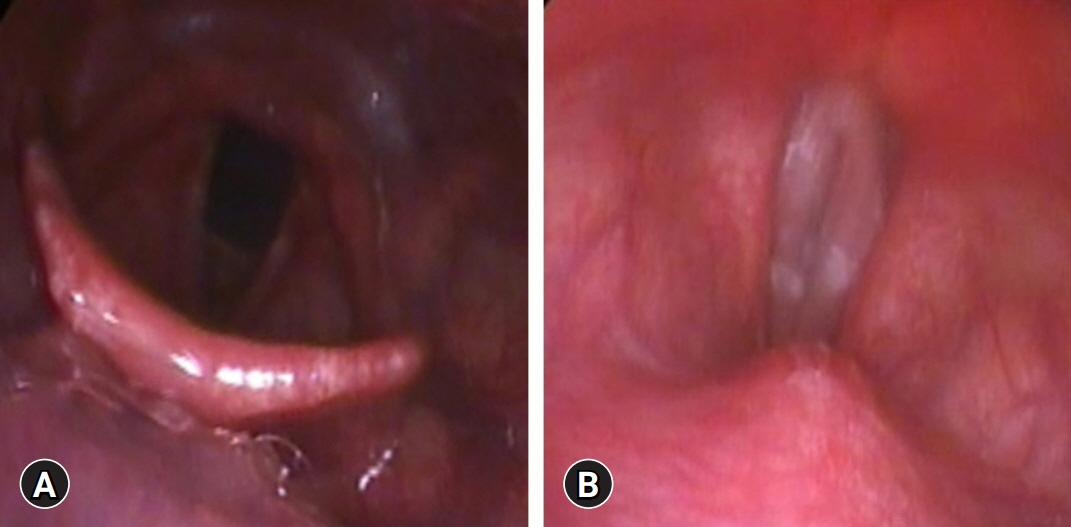
Fig. 2. Fiberoptic endoscopic evaluation of swallowing shows (A) no laryngeal penetration or aspiration and (B) no structural abnormality during phonation.
Reference
-
References
1. Bülow M. Psychogenic dysphagia. In : Shaker R, Belafsky PC, Postma GN, Easterling C, editors. Principles of deglutition. New York: Springer;2013. p. 771–6.2. Barofsky I, Fontaine KR. Do psychogenic dysphagia patients have an eating disorder? Dysphagia. 1998; 13:24–7.3. Scemes S, Wielenska RC, Savoia MG, Bernik M. Choking phobia: full remission following behavior therapy. Braz J Psychiatry. 2009; 31:257–60.4. McNally RJ. Choking phobia: a review of the literature. Compr Psychiatry. 1994; 35:83–9.5. Finkenbine R, Miele VJ. Globus hystericus: a brief review. Gen Hosp Psychiatry. 2004; 26:78–82.6. Ciyiltepe M, Türkbay T. Phagophobia: a case report. Turk J Pediatr. 2006; 48:80–4.7. Shapiro J, Franko DL, Gagne A. Phagophobia: a form of psychogenic dysphagia: a new entity. Ann Otol Rhinol Laryngol. 1997; 106:286–90.8. Ravich WJ, Wilson RS, Jones B, Donner MW. Psychogenic dysphagia and globus: reevaluation of 23 patients. Dysphagia. 1989; 4:35–8.9. Malcomson KG. Radiological findings in globus hystericus. Br J Radiol. 1966; 39:583–6.10. Casado E, Gratacós J, Tolosa C, Martínez JM, Ojanguren I, Ariza A, et al. Antimalarial myopathy: an underdiagnosed complication?: prospective longitudinal study of 119 patients. Ann Rheum Dis. 2006; 65:385–90.11. Kalajian AH, Callen JP. Myopathy induced by antimalarial agents: the relevance of screening muscle enzyme levels. Arch Dermatol. 2009; 145:597–600.12. Knuijt S, Kalf JG, de Swart BJ, Drost G, Hendricks HT, Geurts AC, et al. Dysarthria and dysphagia are highly prevalent among various types of neuromuscular diseases. Disabil Rehabil. 2014; 36:1285–9.13. Somer H, Dubowitz V, Donner M. Creatine kinase isoenzymes in neuromuscular diseases. J Neurol Sci. 1976; 29:129–36.14. Hobson-Webb LD, Jones HN, Kishnani PS. Oropharyngeal dysphagia may occur in late-onset Pompe disease, implicating bulbar muscle involvement. Neuromuscul Disord. 2013; 23:319–23.15. Ito K, Chitose H, Kobayashi A. Upper airway obstruction caused by a floppy epiglottis: report of two cases of amyotrophic lateral sclerosis (ALS). Nihon Jibiinkoka Gakkai Kaiho. 2009; 112:660–4.16. Thottam PJ, Silva RC, McLevy JD, Simons JP, Mehta DK. Use of fiberoptic endoscopic evaluation of swallowing (FEES) in the management of psychogenic dysphagia in children. Int J Pediatr Otorhinolaryngol. 2015; 79:108–10.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Detection of pharyngeal perforation during fiberoptic endoscopic evaluation of swallowing in a person with cervical spinal cord injury in the intensive care unit: a case report
- Evaluation of Dysphagia
- Instrumental Assessment of Swallowing
- The Usefulness of Flexible Endoscopic Evaluation of Swallowing in Head and Neck Cancer Patients
- Rehabilitation Techniques for Dysphagia
