J Korean Neurosurg Soc.
2023 Jan;66(1):82-89. 10.3340/jkns.2022.0143.
Surgical Management and Long-Term Results of Rathke’s Cleft Cyst
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Bundang Hospital, Seongnam, Korea
- 2Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2537851
- DOI: http://doi.org/10.3340/jkns.2022.0143
Abstract
Objective
: Rathke’s cleft cysts (RCCs) are nonneoplastic cysts. Most of them are asymptomatic and stable; when symptomatic, RCCs are surgically fenestrated and drained. However, the outcomes remain unclear. The authors evaluated the outcomes of RCC decompression.
Methods
: Between 2004 and 2019, 32 RCCs were decompressed in a single tertiary institution. The clinical characteristics, intraoperative findings, postoperative complications, and endocrinological and surgical outcomes were retrospectively reviewed. Patients who underwent sequential imaging at least twice and at least 12 months after surgery were included in the analysis.
Results
: Patients’ mean age was 40.8±14.9 years, and 62.5% were women. The mean follow-up duration was 62.3±48.6 months. In 21 patients (65.6%), no residual cysts were identified on postoperative magnetic resonance imaging. Of the 18 patients with preoperative visual field defects, 17 (94.4%) experienced postoperative visual improvement. Postoperative complications included endocrinological deterioration in 11 patients (34.4%), permanent diabetes insipidus in 11 (34.4%), infection in four (12.5%), intrasellar hemorrhage in three (9.4%), and cerebrospinal fluid leak in two (6.3%). Follow-up images revealed cyst recurrence in nine patients (28.1%), an average of 20.4 months after surgery; in three patients, the cysts were symptomatic, and resection was repeated. Multivariable analysis revealed that postoperative endocrinological deterioration was the only independent factor associated with cyst recurrence (p=0.028; hazard ratio, 6.800).
Conclusion
: Our findings showed that although only cyst fenestration for decompression was performed to preserve pituitary function, more pituitary dysfunction occurred than expected. Besides, the postoperative hormonal deterioration itself acted as a risk factor for cyst recurrence. In conclusion, surgery for RCC should be more careful.
Figure
-
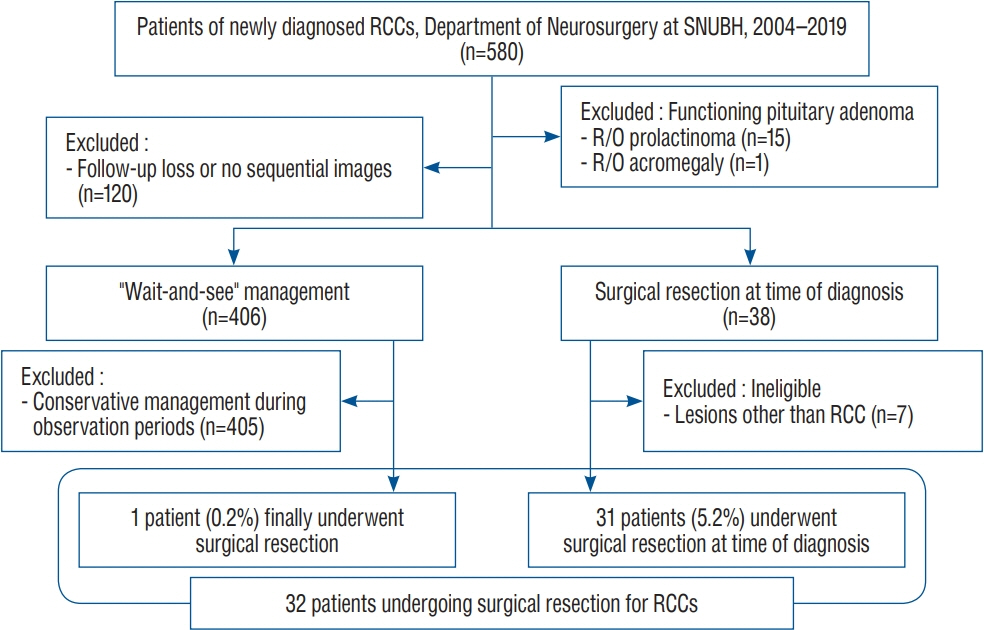
Fig. 1. Flow diagram of patient selection. RCC : Rathke’s cleft cyst, SNUBH : Seoul National University Bundang Hospital, R/O : rule out.

Fig. 2. Kaplan-Meier curve for recurrence free survival.
Reference
-
References
1. Aho CJ, Liu C, Zelman V, Couldwell WT, Weiss MH. Surgical outcomes in 118 patients with Rathke cleft cysts. J Neurosurg. 102:189–193. 2005.2. Barkhoudarian G, Palejwala SK, Ansari S, Eisenberg AA, Huang X, Griffiths CF, et al. Rathke’s cleft cysts: a 6-year experience of surgery vs. observation with comparative volumetric analysis. Pituitary. 22:362–371. 2019.3. Benveniste RJ, King WA, Walsh J, Lee JS, Naidich TP, Post KD. Surgery for Rathke cleft cysts: technical considerations and outcomes. J Neurosurg. 101:577–584. 2004.4. Cabuk B, Selek A, Emengen A, Anik I, Canturk Z, Ceylan S. Clinicopathologic characteristics and endoscopic surgical outcomes of symptomatic Rathke’s cleft cysts. World Neurosurg. 132:e208–e216. 2019.5. Higgins DM, Van Gompel JJ, Nippoldt TB, Meyer FB. Symptomatic Rathke cleft cysts: extent of resection and surgical complications. Neurosurg Focus. 31:E2. 2011.6. Hwang K, Kim YH, Kim JH, Lee JH, Yang HK, Hwang JM, et al. The outcomes of conservatively observed asymptomatic nonfunctioning pituitary adenomas with optic nerve compression. J Neurosurg. 134:1808–1815. 2020.7. Isono M, Kamida T, Kobayashi H, Shimomura T, Matsuyama J. Clinical features of symptomatic Rathke’s cleft cyst. Clin Neurol Neurosurg. 103:96–100. 2001.8. Kim E. Symptomatic Rathke cleft cyst: clinical features and surgical outcomes. World Neurosurg. 78:527–534. 2012.9. Kim JE, Kim JH, Kim OL, Paek SH, Kim DG, Chi JG, et al. Surgical treatment of symptomatic Rathke cleft cysts: clinical features and results with special attention to recurrence. J Neurosurg. 100:33–40. 2004.10. Koutourousiou M, Grotenhuis A, Kontogeorgos G, Seretis A. Treatment of Rathke’s cleft cysts: experience at a single centre. J Clin Neurosci. 16:900–903. 2009.11. Lee C, Park SH. Spontaneously regressed Rathke’s cleft cyst. J Korean Neurosurg Soc. 62:723–726. 2019.12. Lillehei KO, Widdel L, Astete CA, Wierman ME, Kleinschmidt-DeMasters BK, Kerr JM. Transsphenoidal resection of 82 Rathke cleft cysts: limited value of alcohol cauterization in reducing recurrence rates. J Neurosurg. 114:310–317. 2011.13. Lin M, Wedemeyer MA, Bradley D, Donoho DA, Fredrickson VL, Weiss MH, et al. Long-term surgical outcomes following transsphenoidal surgery in patients with Rathke’s cleft cysts. J Neurosurg. 130:831–837. 2018.14. Mendelson ZS, Husain Q, Elmoursi S, Svider PF, Eloy JA, Liu JK. Rathke’s cleft cyst recurrence after transsphenoidal surgery: a meta-analysis of 1151 cases. J Clin Neurosci. 21:378–385. 2014.15. Montaser AS, Catalino MP, Laws ER. Professor Rathke’s gift to neurosurgery: the cyst, its diagnosis, surgical management, and outcomes. Pituitary. 24:787–796. 2021.16. Nishioka H, Haraoka J, Izawa H, Ikeda Y. Headaches associated with Rathke’s cleft cyst. Headache. 46:1580–1586. 2006.17. Ogawa Y, Tominaga T, Ikeda H. Clinicopathological and endocrinological study of Rathke’s cleft cyst manifesting as hyponatremia. Neurol Med Chir (Tokyo). 47:58–63. discussion 63-64. 2007.18. Osborn AG, Preece MT. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology. 239:650–664. 2006.19. Petersson M, Berinder K, Eden Engström B, Tsatsaris E, Ekman B, Wahlberg J, et al. Natural history and surgical outcome of Rathke’s cleft cysts-a study from the Swedish Pituitary Registry. Clin Endocrinol (Oxf). 96:54–61. 2022.20. Prabhu VC, Brown HG. The pathogenesis of craniopharyngiomas. Childs Nerv Syst. 21:622–627. 2005.21. Ratha V, Patil S, Karmarkar VS, Shah NJ, Deopujari CE. Surgical management of Rathke cleft cysts. World Neurosurg. 107:276–284. 2017.22. Sala E, Moore JM, Amorin A, Carosi G, Martinez H Jr, Harsh GR, et al. Natural history of Rathke’s cleft cysts: a retrospective analysis of a two centres experience. Clin Endocrinol (Oxf). 89:178–186. 2018.23. Shatri J, Ahmetgjekaj I. Rathke’s cleft cyst or pituitary apoplexy: a case report and literature review. Open Access Maced J Med Sci. 6:544–547. 2018.24. Yamada H, Ueda R, Ozawa H, Toda M. Long-term outcomes of endoscopic cyst fenestration for Rathke cleft cyst. World Neurosurg. 161:e282–e288. 2022.25. Zada G. Rathke cleft cysts: a review of clinical and surgical management. Neurosurg Focus. 31:E1. 2011.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Symptomatic Rathke's Cleft Cyst in the Interpeduncular Cistern: Case Report
- Suprasellar Rathke Cleft Cyst: A case report
- Rathke's Cleft Cyst: Case Report
- Large Ossified Rathke's Cleft Cyst: A Case Report and Review of the Literature
- Pituitary Tumors Composed of Adenohypophysial Adenoma and Rathke's Cleft Cyst Elements
