Histopathologic and Molecular Biomarkers of PD-1/PD-L1 Inhibitor Treatment Response among Patients with Microsatellite Instability‒High Colon Cancer
- Affiliations
-
- 1Department of Oncology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Asan Center for Cancer Genome Discovery, Asan Institute for Life Sciences, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 3Department of Medical Science, Asan Medical Institute of Convergence Science and Technology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 4Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2534197
- DOI: http://doi.org/10.4143/crt.2021.1133
Abstract
- Purpose
Recent clinical trials have reported response rates < 50% among patients treated with programmed death-1 (PD-1)/programmed death-ligand 1 (PD-L1) inhibitors for microsatellite instability‒high (MSI-H) colorectal cancer (CRC), and factors predicting treatment response have not been fully identified. This study aimed to identify potential biomarkers of PD-1/PD-L1 inhibitor treatment response among patients with MSI-H CRC.
Materials and Methods
MSI-H CRC patients enrolled in three clinical trials of PD-1/PD-L1 blockade at Asan Medical Center (Seoul, Republic of Korea) were screened and classified into two groups according to treatment response. Their histopathologic features and expression of 730 immune-related genes from the NanoString platform were evaluated, and a machine learning–based classification model was built to predict treatment response among MSI-H CRCs patients.
Results
A total of 27 patients (15 responders, 12 non-responders) were included. A high degree of lymphocytic/neutrophilic infiltration and an expansile tumor border were associated with treatment response and prolonged progression-free survival (PFS), while mucinous/signet-ring cell carcinoma was associated with a lack of treatment response and short PFS. Gene expression profiles revealed that the interferon-γ response pathway was enriched in the responder group. Of the top eight differentially expressed immune-related genes, PRAME had the highest fold change in the responder group. Higher expression of PRAME was independently associated with better PFS along with histologic subtypes in the multivariate analysis. The classification model using these genes showed good performance for predicting treatment response.
Conclusion
We identified histologic and immune-related gene expression characteristics associated with treatment response in MSI-H CRC, which may contribute to optimal patient stratification.
Keyword
Figure
-
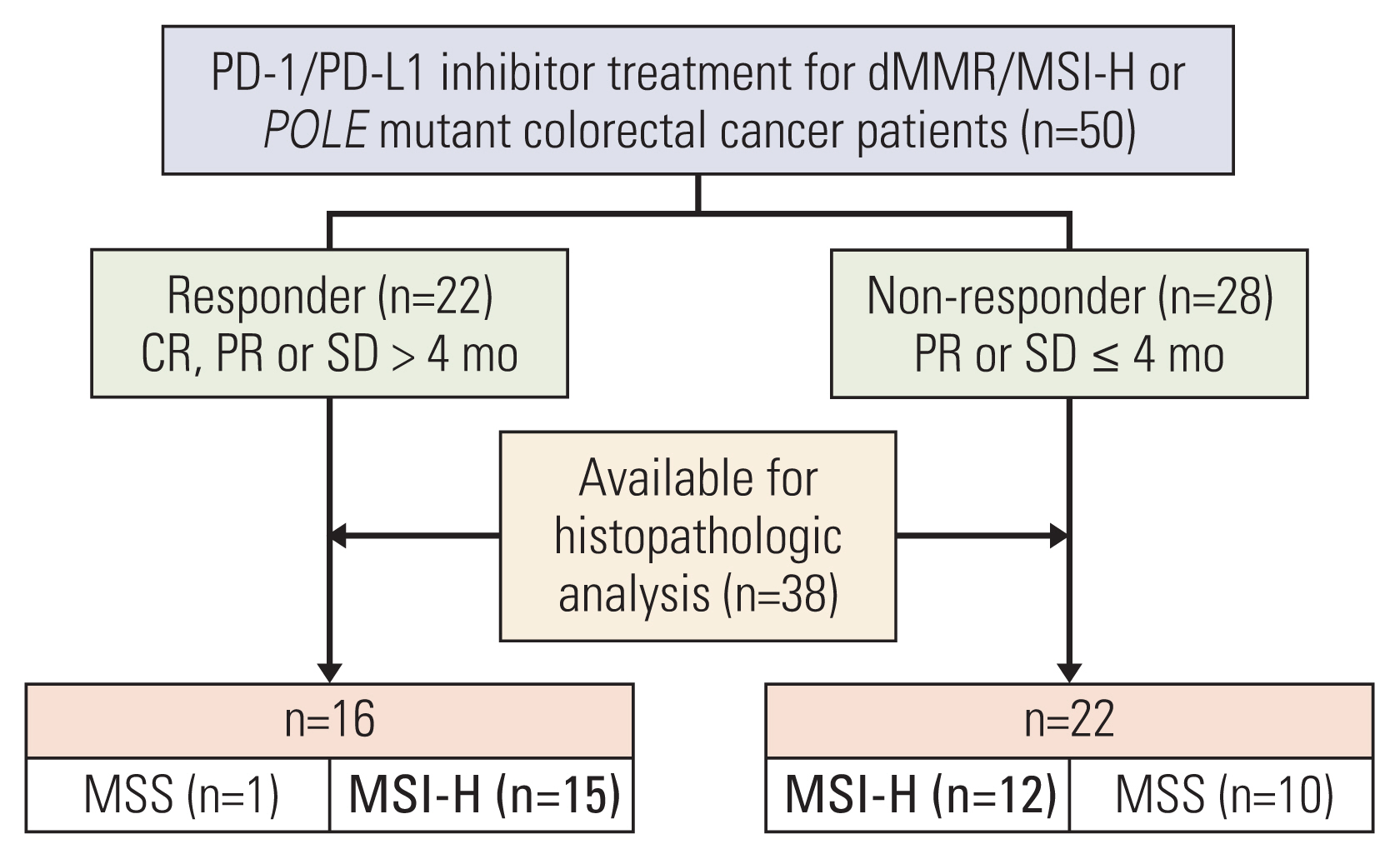
Fig. 1 Case selection and study design according to the response to immune checkpoint inhibitor treatment among patients with deficient mismatch repair (dMMR)/microsatellite instability–high (MSI-H) metastatic colorectal cancers. CR, complete response; MSS, microsatellite stable; PD-1, programmed death-1; PD-L1, programmed death-ligand 1; PR, partial response; SD, stable disease.
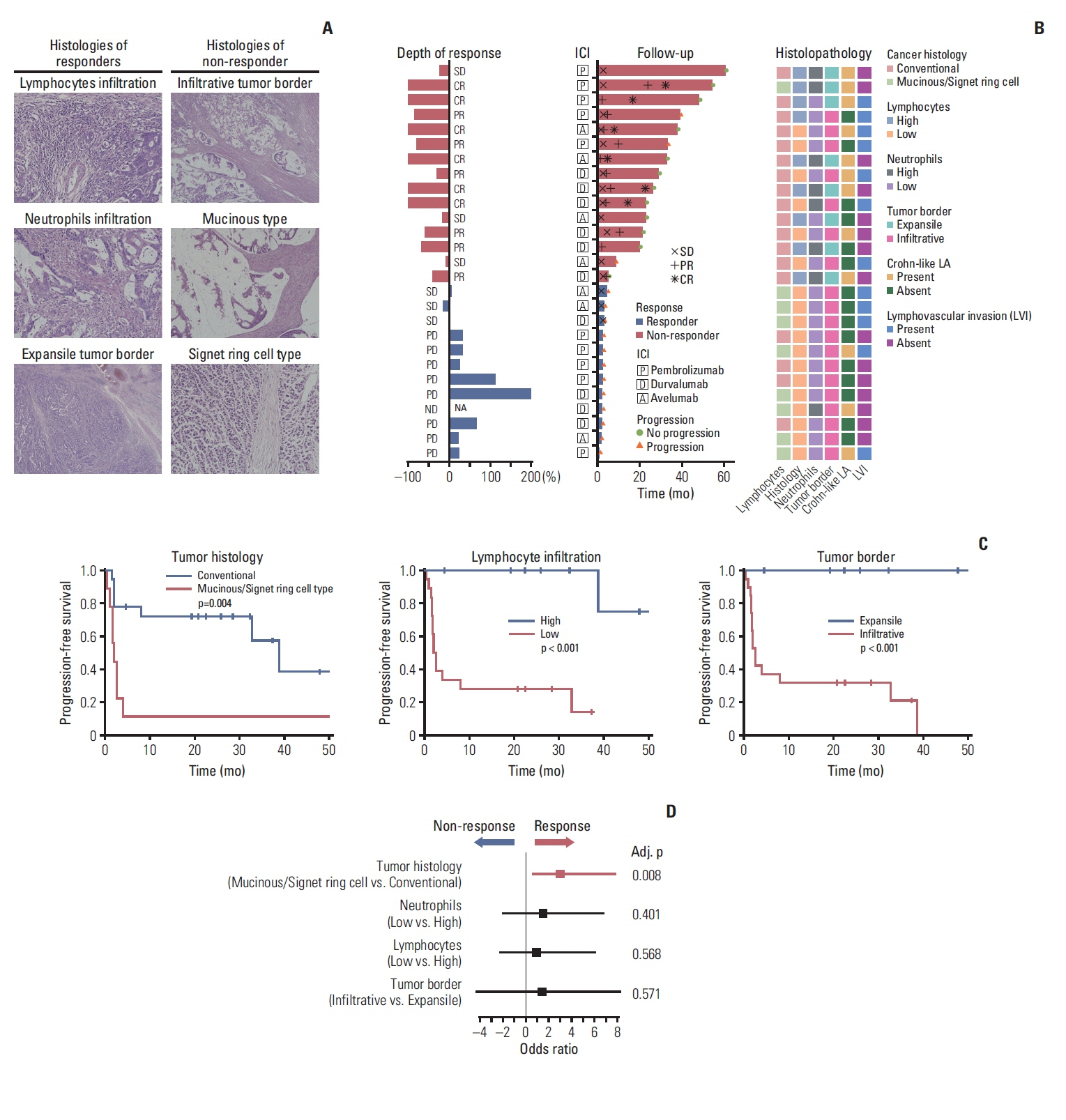
Fig. 2 Histopathologic features associated with ICI response among patients with dMMR/MSI-H CRC. (A) Representative histologic features of MSI-H CRCs among responders and non-responders. High degree of lymphocytic infiltration along the tumor border in the responder group (upper left, ×200). High degree of neutrophil infiltration grade along the tumor-stroma interface in the responder group (middle left, ×200). Expansile tumor border and surrounding of tumor cells by inflammatory cell infiltrates in the responder group (lower left, ×40). Infiltrative tumor border in the non-responder group (upper right, ×40). Mucinous adenocarcinoma with abundant extracellular mucin separating tumor cells from adjacent stroma in the non-responder group (middle right, ×100). Signet-ring cell carcinoma without signs of inflammatory cell infiltration along the tumor-stroma interface in the non-responder group (lower right, ×200). (B) Response status after ICI during follow-up and histopathologic features in patients with MSI-H CRCs. (C) Progression-free survival (log-rank test) of patients with MSI-H CRCs after ICI according to tumor histology, lymphocyte infiltration, and tumor border. (D) Multivariable logistic regression analysis of treatment response with histopathologic variables. CR, complete response; CRC, colorectal cancer; dMMR, deficient mismatch repair; ICI, immune checkpoint inhibitor; LA, lymphoid aggregate; MSI-H, microsatellite instability–high; ND, not determined; PD, progressive disease; PR, partial response; SD, stable disease.
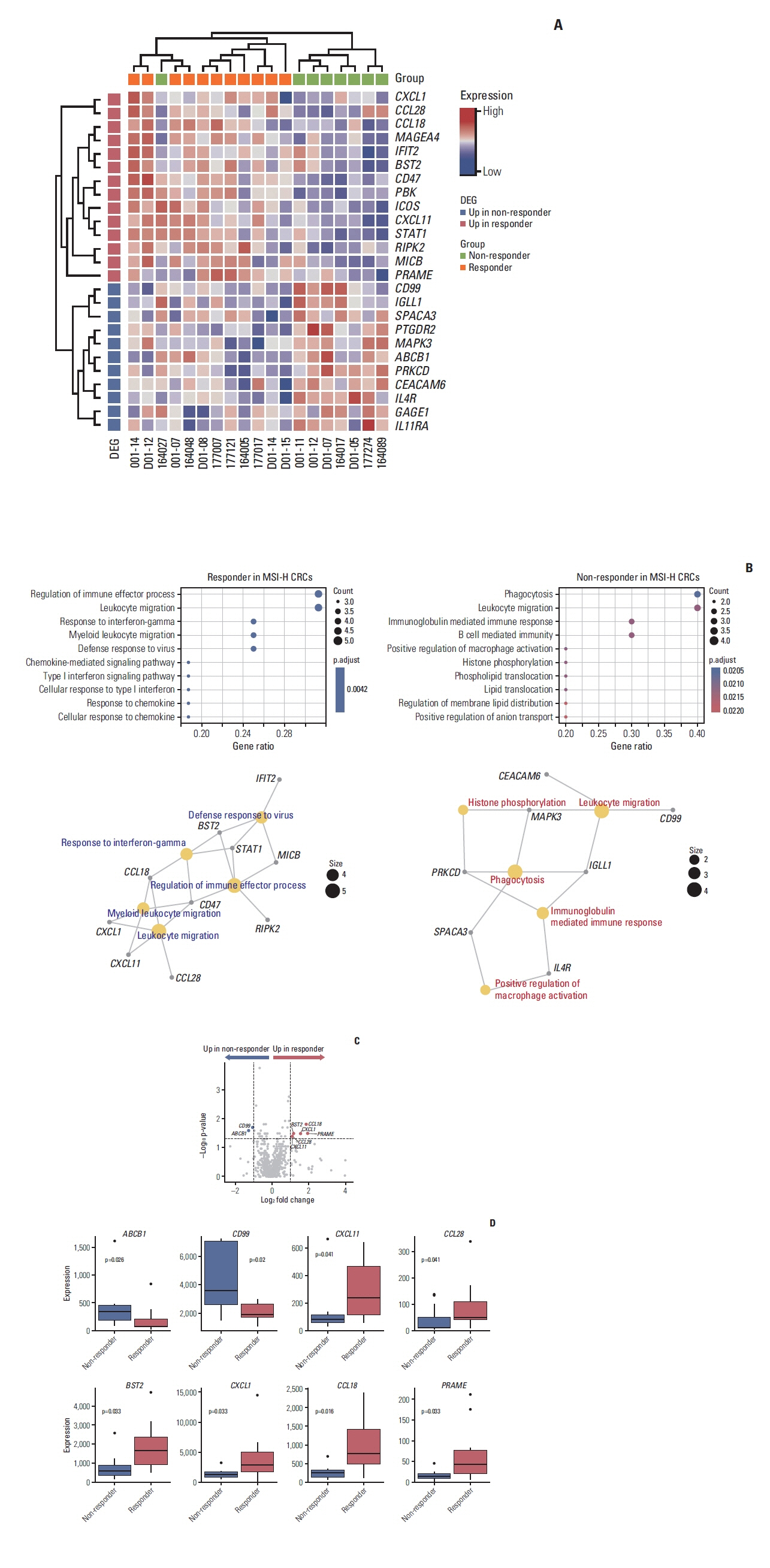
Fig. 3 Differential expression analysis of immune genes between the two groups (11 responders vs. 8 non-responders). (A) Heatmap of differentially expressed immune genes (absolute log2FC > 0.5 and p < 0.05 by Wilcoxon rank-sum test) between the two groups. (B) Enriched pathways in gene ontology enrichment analysis of responders and non-responders. (C) Volcano plots highlighting genes with significantly higher expression in the responder group and non-responder group (absolute log2FC > 0.5 and p < 0.05 by Wilcoxon rank-sum test). (D) The comparative expression levels of genes with significantly higher expression in the responder group (BST2, CCL18, CCL28, CXCL1, CXCL11, and PRAME) and the non-responder group (ABCB1 and CD99). CRC, colorectal cancer; DEG, differentially expressed genes; MSI-H, microsatellite instability–high.

Fig. 4 Association between PRAME expression and response to ICIs. (A) Representative IHC results of PRAME with nuclear expression in CRC cells (×100) and significant correlation between protein expression and mRNA expression (p=0.0036, Wilcoxon rank-sum test). (B) Spider plot of the changes in the sum of target lesions from the baseline along ICI treatment with annotation of the PRAME IHC results. (C) Swimmer plot showing the clinical response and duration of ICI treatment with PRAME IHC results and PRAME mRNA expression levels. (D) Progression-free survival outcomes according to PRAME protein expression and PRAME mRNA expression among patients with MSI-H CRCs after ICI treatment (log-rank test). (E) Multivariable Cox regression analysis for progression-free survival. CI, confidence interval; CR, complete response; CRC, colorectal cancer; ICI, immune checkpoint inhibitor; IHC, immunohistochemistry; MSI-H, microsatellite instability–high; PD, progressive disease; PR, partial response; SD, stable disease.
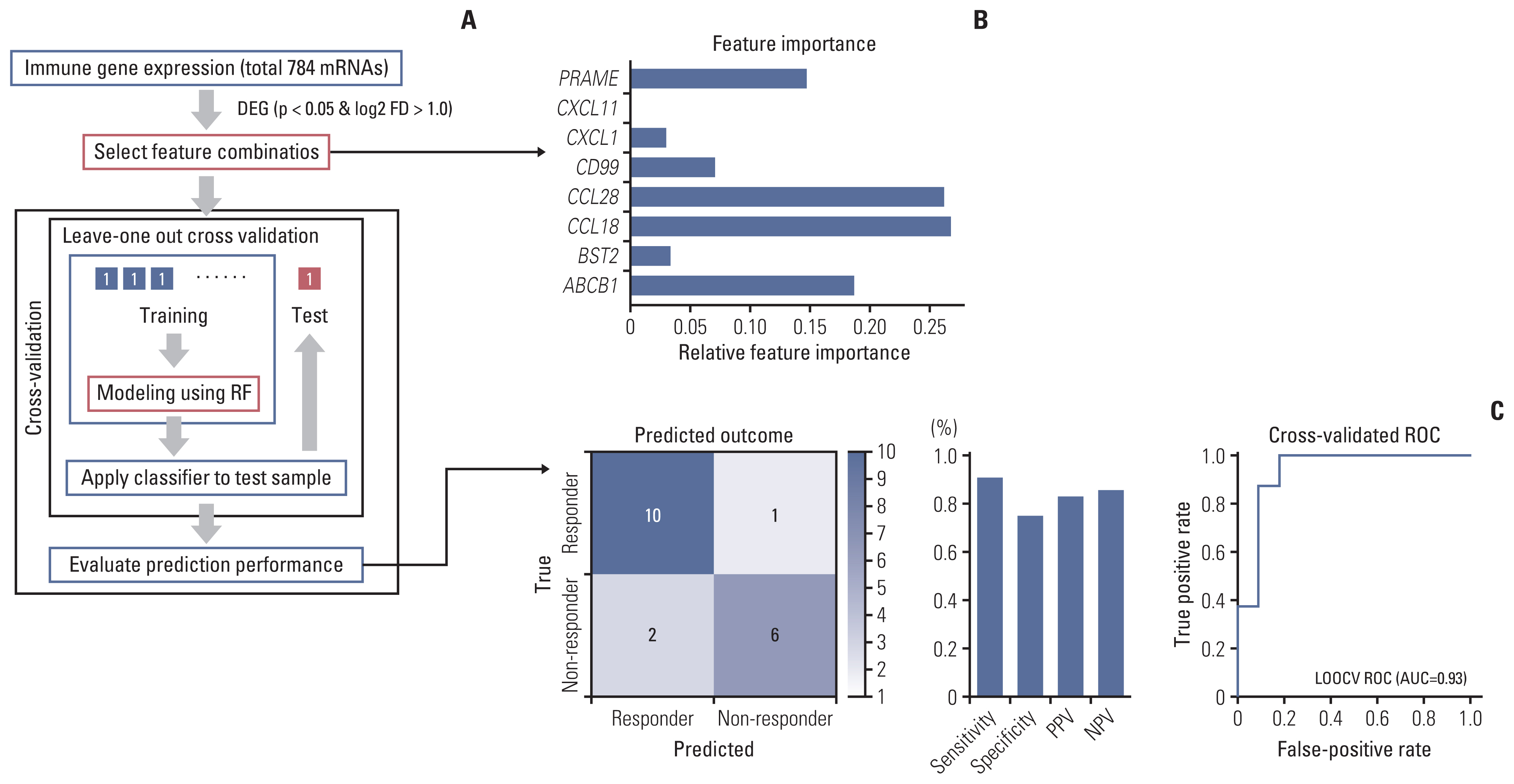
Fig. 5 Prediction modeling for treatment response to ICIs among patients with MSI-H CRCs. (A) Overview of the processes of prediction model building using RF based on immune-related gene expression and internal validation of the model using the LOOCV method. (B) Feature importance of input genes in modeling by RF. (C) Performance of the prediction model. AUC, area under the curve; CRC, colorectal cancer; DEG, differentially expressed genes; ICI, immune checkpoint inhibitor; LOOCV, leave-one-out cross-validation; MSI-H, microsatellite instability–high; NPV, negative predictive value; PPV, positive predictive value; RF, random forest; ROC, receiver operating characteristic.
Reference
-
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424.
Article2. Atreya CE, Yaeger R, Chu E. Systemic therapy for metastatic colorectal cancer: from current standards to future molecular targeted approaches. Am Soc Clin Oncol Educ Book. 2017; 37:246–56.
Article3. Venderbosch S, Nagtegaal ID, Maughan TS, Smith CG, Cheadle JP, Fisher D, et al. Mismatch repair status and BRAF mutation status in metastatic colorectal cancer patients: a pooled analysis of the CAIRO, CAIRO2, COIN, and FOCUS studies. Clin Cancer Res. 2014; 20:5322–30.4. National Comprehensive Cancer Network. Colon cancer (version 1, 2021) [Internet]. Plymouth Meeting, PA: National Comprehensive Cancer Network;c2021. [cited 2021 Jan 21]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf .5. Boland CR, Goel A. Microsatellite instability in colorectal cancer. Gastroenterology. 2010; 138:2073–87.
Article6. Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, et al. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med. 2015; 372:2509–20.7. Overman MJ, McDermott R, Leach JL, Lonardi S, Lenz HJ, Morse MA, et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol. 2017; 18:1182–91.
Article8. Andre T, Shiu KK, Kim TW, Jensen BV, Jensen LH, Punt C, et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N Engl J Med. 2020; 383:2207–18.
Article9. Kim JH, Kim SY, Baek JY, Cha YJ, Ahn JB, Kim HS, et al. A phase II study of avelumab monotherapy in patients with mismatch repair-deficient/microsatellite instability-high or POLE-mutated metastatic or unresectable colorectal cancer. Cancer Res Treat. 2020; 52:1135–44.10. Durvalumab for MSI-H or POLE mutated metastatic colorectal cancer [Internet]. Bethesda, MD: US National Library of Medicine;2020. [cited 2021 Jan 21]. Available from: https://ClinicalTrials.gov/show/NCT03435107 .11. Le DT, Kim TW, Van Cutsem E, Geva R, Jager D, Hara H, et al. Phase II open-label study of pembrolizumab in treatment-refractory, microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: KEYNOTE-164. J Clin Oncol. 2020; 38:11–9.
Article12. Kim JE, Chun SM, Hong YS, Kim KP, Kim SY, Kim J, et al. Mutation burden and I index for detection of microsatellite instability in colorectal cancer by targeted next-generation sequencing. J Mol Diagn. 2019; 21:241–50.
Article13. Cohen R, Buhard O, Cervera P, Hain E, Dumont S, Bardier A, et al. Clinical and molecular characterisation of hereditary and sporadic metastatic colorectal cancers harbouring microsatellite instability/DNA mismatch repair deficiency. Eur J Cancer. 2017; 86:266–74.
Article14. Guyot D’Asnieres De Salins A, Tachon G, Cohen R, Karayan-Tapon L, Junca A, Frouin E, et al. Discordance between immunochemistry of mismatch repair proteins and molecular testing of microsatellite instability in colorectal cancer. ESMO Open. 2021; 6:100120.
Article15. Agilent Technologies. Instructions for use: PD-L1 IHC 22C3 pharmDx. Santa Clara, CA: Agilent Technologies;2018.16. Funkhouser WK Jr, Lubin IM, Monzon FA, Zehnbauer BA, Evans JP, Ogino S, et al. Relevance, pathogenesis, and testing algorithm for mismatch repair-defective colorectal carcinomas: a report of the association for molecular pathology. J Mol Diagn. 2012; 14:91–103.
Article17. Alexander J, Watanabe T, Wu TT, Rashid A, Li S, Hamilton SR. Histopathological identification of colon cancer with microsatellite instability. Am J Pathol. 2001; 158:527–35.
Article18. Halvarsson B, Anderson H, Domanska K, Lindmark G, Nilbert M. Clinicopathologic factors identify sporadic mismatch repair-defective colon cancers. Am J Clin Pathol. 2008; 129:238–44.
Article19. Jenkins MA, Hayashi S, O’Shea AM, Burgart LJ, Smyrk TC, Shimizu D, et al. Pathology features in Bethesda guidelines predict colorectal cancer microsatellite instability: a population-based study. Gastroenterology. 2007; 133:48–56.
Article20. Havel JJ, Chowell D, Chan TA. The evolving landscape of biomarkers for checkpoint inhibitor immunotherapy. Nat Rev Cancer. 2019; 19:133–50.
Article21. Pages F, Mlecnik B, Marliot F, Bindea G, Ou FS, Bifulco C, et al. International validation of the consensus Immunoscore for the classification of colon cancer: a prognostic and accuracy study. Lancet. 2018; 391:2128–39.22. Coppola D, Nebozhyn M, Khalil F, Dai H, Yeatman T, Loboda A, et al. Unique ectopic lymph node-like structures present in human primary colorectal carcinoma are identified by immune gene array profiling. Am J Pathol. 2011; 179:37–45.
Article23. Berry RS, Xiong MJ, Greenbaum A, Mortaji P, Nofchissey RA, Schultz F, et al. High levels of tumor-associated neutrophils are associated with improved overall survival in patients with stage II colorectal cancer. PLoS One. 2017; 12:e0188799.
Article24. Mlecnik B, Bindea G, Angell HK, Maby P, Angelova M, Tougeron D, et al. Integrative analyses of colorectal cancer show immunoscore is a stronger predictor of patient survival than microsatellite instability. Immunity. 2016; 44:698–711.
Article25. Boissiere-Michot F, Lazennec G, Frugier H, Jarlier M, Roca L, Duffour J, et al. Characterization of an adaptive immune response in microsatellite-instable colorectal cancer. Oncoimmunology. 2014; 3:e29256.
Article26. Ayers M, Lunceford J, Nebozhyn M, Murphy E, Loboda A, Kaufman DR, et al. IFN-gamma-related mRNA profile predicts clinical response to PD-1 blockade. J Clin Invest. 2017; 127:2930–40.27. Stoll G, Pol J, Soumelis V, Zitvogel L, Kroemer G. Impact of chemotactic factors and receptors on the cancer immune infiltrate: a bioinformatics study revealing homogeneity and heterogeneity among patient cohorts. Oncoimmunology. 2018; 7:e1484980.28. Epping MT, Bernards R. A causal role for the human tumor antigen preferentially expressed antigen of melanoma in cancer. Cancer Res. 2006; 66:10639–42.
Article29. Schrock AB, Ouyang C, Sandhu J, Sokol E, Jin D, Ross JS, et al. Tumor mutational burden is predictive of response to immune checkpoint inhibitors in MSI-high metastatic colorectal cancer. Ann Oncol. 2019; 30:1096–103.30. Cristescu R, Mogg R, Ayers M, Albright A, Murphy E, Yearley J, et al. Pan-tumor genomic biomarkers for PD-1 checkpoint blockade-based immunotherapy. Science. 2018; 362:eaar3593.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Peripheral blood immune cell-based biomarkers in anti-PD-1/PD-L1 therapy
- PD-1: A Negative Regulator of Phagocytosis by Tumour-Associated Macrophages in Colon Cancer
- Characteristics of Immune-Related Thyroid Adverse Events in Patients Treated with PD-1/PD-L1 Inhibitors
- Evaluation of circulating PD-1 and PD-L1 as diagnostic biomarkers in dogs with tumors
- Is a Microsatellite Instability Still Useful for Tailored Treatment in Stage II and III Colon Cancer?
