Adenosine Deaminase 2 Deficiency Caused by Biallele Variants Including Splicing Variant: The First Case in Korea
- Affiliations
-
- 1Department of Pediatrics, Seoul National University Hospital, Seoul, Korea
- 2GENOME INSIGHT Inc., Korea
- 3Graduate School of Medical Science and Engineering, Korea Advanced Institute of Science and Technology, Daejeon, Korea
- 4Hospital Medicine Center, Seoul National University Hospital, Seoul, Korea
- KMID: 2533626
- DOI: http://doi.org/10.4078/jrd.21.0046
Abstract
- Deficiency of adenosine deaminase 2 (DADA2) is an autoinflammatory disease caused by pathogenic variants of the ADA2 gene and has similar clinical features to polyarteritis nodosa (PAN). We, herein, report a case of DADA2 in Korea that was diagnosed in a patient with childhood-onset PAN. The patient had a truncal ataxia and facial palsy caused by thalamic infarction at 34 months of age. Livedo reticularis with Raynaud phenomenon and abdominal pain with fever were followed. Radiologic examination showed multiple infarctions in brain and kidney. She was diagnosed with PAN using skin biopsy and angiography. She had severe hemorrhagic strokes despite medical treatments. Her disease activity was controlled after adding a tumor necrosis factor-α inhibitor. Molecular analysis revealed compound heterozygous pathogenic variants of ADA2 gene. This is the first case of DADA2 in Korea. Genetic analysis for ADA2 gene should be considered in patients with childhood-onset PAN.
Figure
-
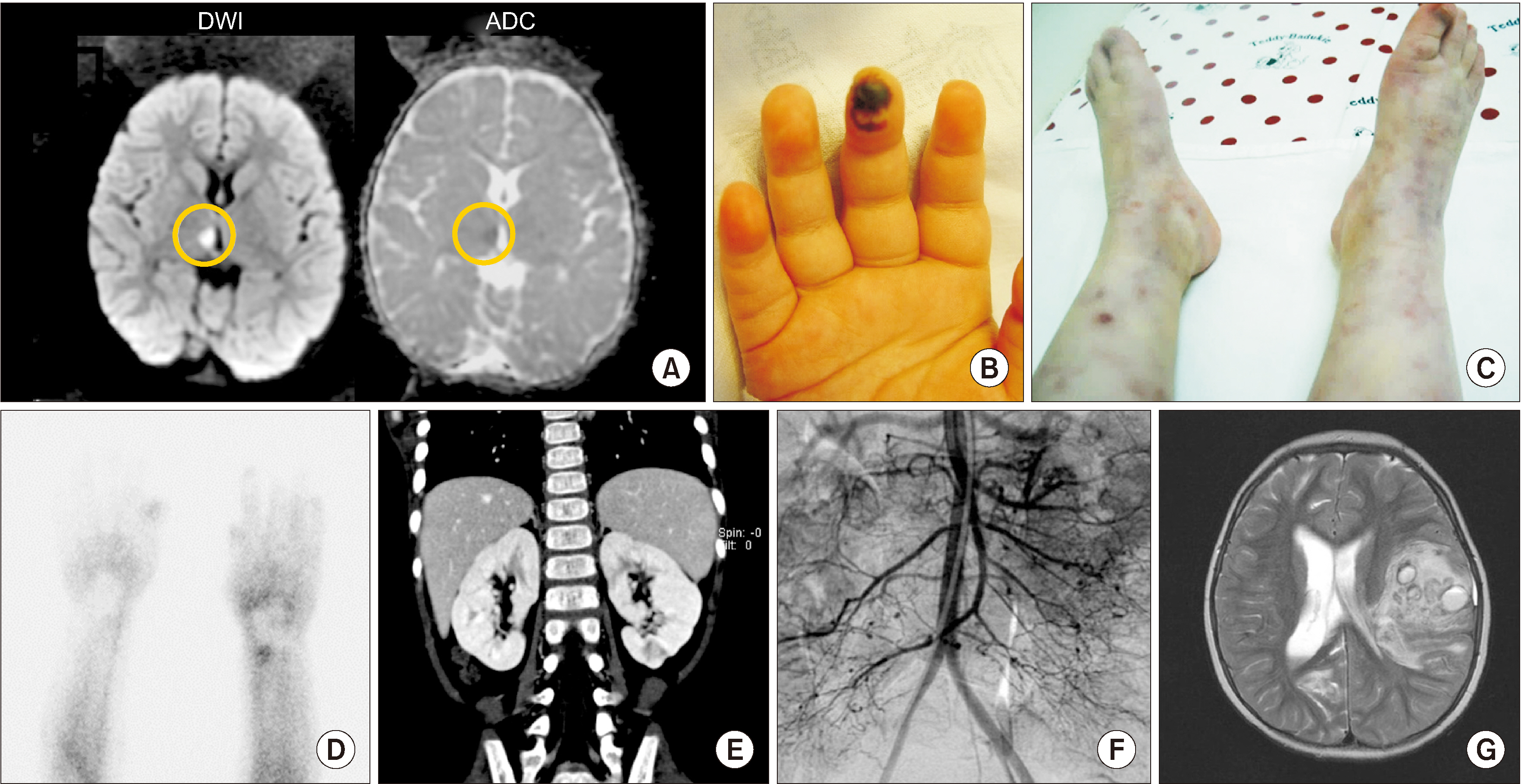
Fig. 1 Skin manifestations and radiological findings. (A) The first magnetic resonance imaging (MRI) for brain revealed high signal intensity in diffusion weighted image (DWI), low signal intensity in apparent diffusion coefficient (ADC) on the right thalamus (yellow circle) which was conducted when the 1st neurologic symptoms; truncal ataxia, facial palsy with ptosis on the left side occurred. (B) Digital gangrene was observed on right 3rd finger. (C) Retiform purpura and livedo reticularis were shown on both lower legs with coldness. (D) Raynaud scan by 99mTc showed defects of digital blood flow on both hands, especially right the 2nd to 4th fingers and left 3rd and 4th fingers. (E) On computed tomography, several wedge-shaped focal, low attenuated lesions were observed in both kidneys and appeared to be infarctions. (F) Angiography showed multiple aneurysms in the superior mesenteric artery, inferior mesenteric artery, both renal, and splenic artery’s small branch. (G) The T2-weighted image of brain MRI showed a large amount of intracerebral hemorrhage which affects midline shifting and ventricular size at the age of 5 years.

Fig. 2 Main medical events and treatments. The patient had multiple infarctions including brain even though she received various immunosuppressive agents, but these events did not occur after tumor necrosis factor-α inhibitor (infliximab) therapy was commenced at the age of 13 years. The arrows indicate the administration of each drug. The horizontal arrow means a continuation of medication and the vertical arrow means pulse therapy. The administration method and dose of each drug are as follows. Prednisolone per oral (PO), Methylprednisolone pulse therapy intravenously (IV), Cyclophosphamide: pulse therapy IV and PO, Anticoagulant: low molecular heparin IV, warfarin PO, Azathioprine: PO, Lipo-Prostaglandin E1 (PGE-1-lipo): IV, Methotrexate: PO, Infliximab: IV, Intravenous immunoglobulin G.

Fig. 3 Results for genetic analysis. (A) The patient's pedigree. Compound heterozygous variants of ADA2 gene were inherited from her father (c753G>A, p.Pro251Pro) and mother (c.1069G>A, p.Ala357Thr), which lead to abnormal splicing and missense mutation, respectively (B). The patient has compound heterozygote variant exon 4 (c753G>A , p.Pro251Pro) and exon 7 (c.1069G>A, p.Ala357Thr). Integrative genomics viewer (IGV) for analysis of whole genome sequencing showed that these variants were inherited from her parents. (C) IGV for analysis of RNA sequencing showed retained intron, which was produced by non-decayed adenine. (D) Sashimi plot on IGV for RNA sequencing analysis showed mRNA splicing on patient and healthy control. Retained intron was observed on intron 4 in this patient. (E) Allele from her father has adenine on 753th nucleotide of the patient on DNA analysis. However, in RNA sequencing analysis, about 33% of adenine was decayed by nonsense-mediated mRNA decay (NMD) to reduce errors in gene expression and remnant 22% of adenine processes mRNA on RNA sequencing called retained intron.
Reference
-
1. Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2013; 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 65:1–11. DOI: 10.1002/art.37715. PMID: 23045170.
Article2. Navon Elkan P, Pierce SB, Segel R, Walsh T, Barash J, Padeh S, et al. 2014; Mutant adenosine deaminase 2 in a polyarteritis nodosa vasculopathy. N Engl J Med. 370:921–31. DOI: 10.1056/NEJMoa1307362. PMID: 24552285.
Article3. Iudici M, Quartier P, Pagnoux C, Merlin E, Agard C, Aouba A, et al. 2018; Childhood- versus adult-onset polyarteritis nodosa results from the French Vasculitis Study Group registry. Autoimmun Rev. 17:984–9. DOI: 10.1016/j.autrev.2018.08.001. PMID: 30114520.
Article4. Zhou Q, Yang D, Ombrello AK, Zavialov AV, Toro C, Zavialov AV, et al. 2014; Early-onset stroke and vasculopathy associated with mutations in ADA2. N Engl J Med. 370:911–20. DOI: 10.1056/NEJMoa1307361. PMID: 24552284. PMCID: PMC4193683.5. Meyts I, Aksentijevich I. 2018; Deficiency of adenosine deaminase 2 (DADA2): updates on the phenotype, genetics, pathogenesis, and treatment. J Clin Immunol. 38:569–78. DOI: 10.1007/s10875-018-0525-8. PMID: 29951947. PMCID: PMC6061100.
Article6. Lee PY. 2018; Vasculopathy, immunodeficiency, and bone marrow failure: the intriguing syndrome caused by deficiency of adenosine deaminase 2. Front Pediatr. 6:282. DOI: 10.3389/fped.2018.00282. PMID: 30406060. PMCID: PMC6200955.
Article7. Pinto B, Deo P, Sharma S, Syal A, Sharma A. 2021; Expanding spectrum of DADA2: a review of phenotypes, genetics, pathogenesis and treatment. Clin Rheumatol. 40:3883–96. DOI: 10.1007/s10067-021-05711-w. PMID: 33791889.
Article8. Human A, Pagnoux C. 2019; Diagnosis and management of ADA2 deficient polyarteritis nodosa. Int J Rheum Dis. 22 Suppl 1:69–77. DOI: 10.1111/1756-185X.13283. PMID: 29624883.
Article9. Lightfoot RW Jr, Michel BA, Bloch DA, Hunder GG, Zvaifler NJ, McShane DJ, et al. 1990; The American College of Rheumatology 1990 criteria for the classification of polyarteritis nodosa. Arthritis Rheum. 33:1088–93. DOI: 10.1002/art.1780330805. PMID: 1975174.
Article10. Westendorp WF, Nederkoorn PJ, Aksentijevich I, Hak AE, Lichtenbelt KD, Braun KP. 2015; Unexplained early-onset lacunar stroke and inflammatory skin lesions: consider ADA2 deficiency. Neurology. 84:2092–3. DOI: 10.1212/WNL.0000000000001581. PMID: 25888558. PMCID: PMC4442100.
Article11. Ombrello AK, Qin J, Hoffmann PM, Kumar P, Stone D, Jones A, et al. 2019; Treatment strategies for deficiency of adenosine deaminase 2. N Engl J Med. 380:1582–4. DOI: 10.1056/NEJMc1801927. PMID: 30995379. PMCID: PMC7372950.
Article12. Chung SA, Gorelik M, Langford CA, Maz M, Abril A, Guyatt G, et al. 2021; 2021 American College of Rheumatology/Vasculitis Foundation guideline for the management of polyarteritis nodosa. Arthritis Rheumatol. 73:1384–93. DOI: 10.1002/art.41776. PMID: 34235883.
Article13. Huang Z, Li T, Nigrovic PA, Lee PY. 2020; Polyarteritis nodosa and deficiency of adenosine deaminase 2 - shared genealogy, generations apart. Clin Immunol. 215:108411. DOI: 10.1016/j.clim.2020.108411. PMID: 32276138. PMCID: PMC7387119.
Article14. Caorsi R, Penco F, Schena F, Gattorno M. 2016; Monogenic polyarteritis: the lesson of ADA2 deficiency. Pediatr Rheumatol Online J. 14:51. DOI: 10.1186/s12969-016-0111-7. PMID: 27609179. PMCID: PMC5015262.
Article15. Gibson KM, Morishita KA, Dancey P, Moorehead P, Drögemöller B, Han X, et al. 2019; Identification of novel adenosine deaminase 2 gene variants and varied clinical phenotype in pediatric vasculitis. Arthritis Rheumatol. 71:1747–55. DOI: 10.1002/art.40913. PMID: 31008556.
Article16. Rama M, Duflos C, Melki I, Bessis D, Bonhomme A, Martin H, et al. 2018; A decision tree for the genetic diagnosis of deficiency of adenosine deaminase 2 (DADA2): a French reference centres experience. Eur J Hum Genet. 26:960–71. DOI: 10.1038/s41431-018-0130-6. PMID: 29681619. PMCID: PMC6018671.
Article17. Baralle D, Baralle M. 2005; Splicing in action: assessing disease causing sequence changes. J Med Genet. 42:737–48. DOI: 10.1136/jmg.2004.029538. PMID: 16199547. PMCID: PMC1735933.
Article18. Cartegni L, Chew SL, Krainer AR. 2002; Listening to silence and understanding nonsense: exonic mutations that affect splicing. Nat Rev Genet. 3:285–98. DOI: 10.1038/nrg775. PMID: 11967553.
Article19. Crotti LB, Horowitz DS. 2009; Exon sequences at the splice junctions affect splicing fidelity and alternative splicing. Proc Natl Acad Sci U S A. 106:18954–9. DOI: 10.1073/pnas.0907948106. PMID: 19855008. PMCID: PMC2776460.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adenosine Deaminase Activities in Sera and Erythrocytes of Patients with Psoriasis
- Diagnostic value of adenosine deaminase and lysozyme activity in pleural effusion
- A study on the diagnostic value of cerebrospinal fluid adenosine deaminase activity in children with tuberculous meningitis
- Adenosine deaminase activity in bronchoalveolar lavage fluid in patients with pulmonary tuberculosis
- Adenosine Deaminase Activities in Sera and Erythrocytes of Leprosy Patients
