Clinical Usefulness of Virtual Ablation Guided Catheter Ablation of Atrial Fibrillation Targeting Restitution Parameter-Guided Catheter Ablation: CUVIA-REGAB Prospective Randomized Study
- Choi Y
 1
1 - Lim B2
- Yang SY2
- Yang SH2
- Kwon OS2
- Kim D2
- Kim YG3
- Park JW2
- Yu HT2
- Kim TH2
- Yang PS4
- Uhm JS2
- Shim J3
- Kim SH1
- Sung JH4
- Choi Ji3
- Joung B2
- Lee MH2
- Kim YH3
- Oh YS1
- Pak HN2
- for the CUVIA-REGAB Investigators
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Seoul St. Mary Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Department of Cardiology, Yonsei University College of Medicine, Yonsei University Health System, Seoul, Korea
- 3Department of Cardiology, Korea University Cardiovascular Center, Korea University, Seoul, Korea
- 4Department of Cardiology, Bundang CHA Hospital, CHA College of Medicine, Seoul, Korea
- KMID: 2532935
- DOI: http://doi.org/10.4070/kcj.2022.0113
Abstract
- Background and Objectives
We investigated whether extra-pulmonary vein (PV) ablation targeting a high maximal slope of the action potential duration restitution curve (Smax) improves the rhythm outcome of persistent atrial fibrillation (PeAF) ablation.
Methods
In this open-label, multi-center, randomized, and controlled trial, 178 PeAF patients were randomized with 1:1 ratio to computational modeling-guided virtual Smax ablation (V-Smax) or empirical ablation (E-ABL) groups. Smax maps were generated by computational modeling based on atrial substrate maps acquired during clinical procedures in sinus rhythm. Smax maps were generated during the clinical PV isolation (PVI). The V-Smax group underwent an additional extra-PV ablation after PVI targeting the virtual high Smax sites.
Results
After a mean follow-up period of 12.3±5.2 months, the clinical recurrence rates (25.6% vs. 23.9% in the V-Smax and the E-ABL group, p=0.880) or recurrence appearing as atrial tachycardia (11.1% vs. 5.7%, p=0.169) did not differ between the 2 groups. The postablation cardioversion rate was higher in the V-Smax group than E-ABL group (14.4% vs. 5.7%, p=0.027). Among antiarrhythmic drug-free patients (n=129), the AF freedom rate was 78.7% in the V-Smax group and 80.9% in the E-ABL group (p=0.776). The total procedure time was longer in the V-Smax group (p=0.008), but no significant difference was found in the major complication rates (p=0.497) between the groups.
Conclusions
Unlike a dominant frequency ablation, the computational modeling-guided V-Smax ablation did not improve the rhythm outcome of the PeAF ablation and had a longer procedure time.
Keyword
Figure
-
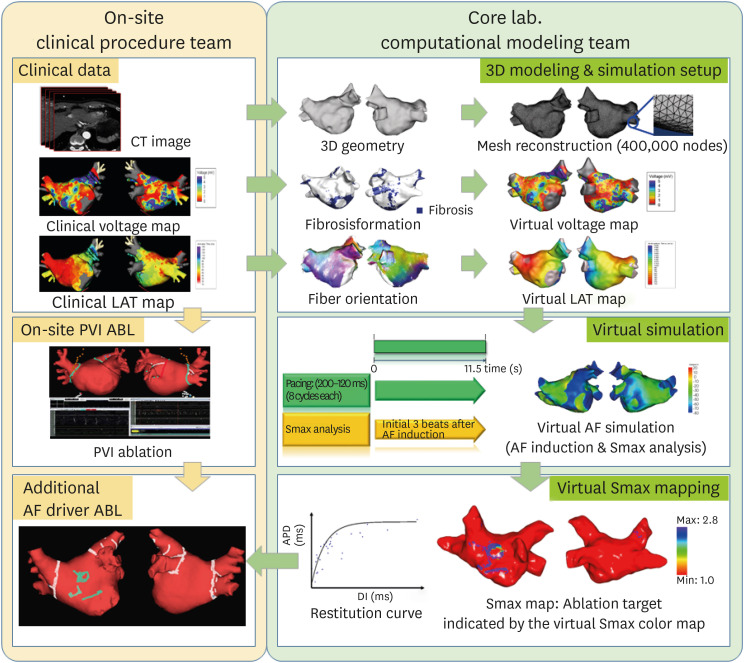
Figure 1 Study process in the V-Smax group.ABL = ablation; AF = atrial fibrillation; CT = computed tomography; LAT = local activation time; PVI = pulmonary vein isolation; 3D = 3-dimensional.

Figure 2 Study enrollment. Included patients were randomly assigned to receive virtual rotor guided ablation or empirical ablation therapy.AF = atrial fibrillation; AFCA = atrial fibrillation catheter ablation; E-ABL = empirical ablation; PVI = pulmonary vein isolation; V-Smax = virtual high maximal slope of the action potential duration restitution curve simulation.
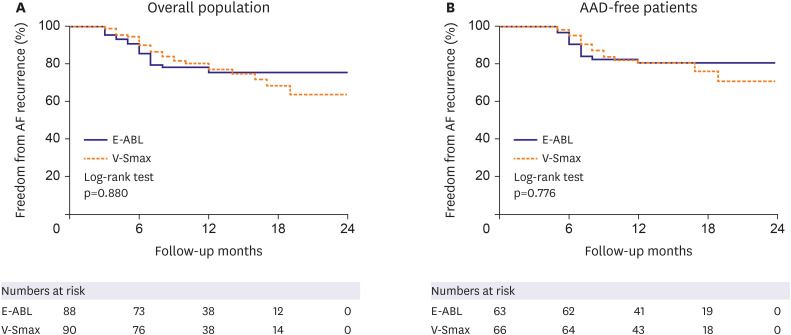
Figure 3 Freedom from AF recurrence in the 2 groups. (A) AF freedom in overall patients. (B) AF freedom in AAD-free patients at 3 months after AFCA.AAD = antiarrhythmic drug; AF = atrial fibrillation; AFCA = atrial fibrillation catheter ablation; E-ABL = empirical ablation; V-Smax = virtual high maximal slope of the action potential duration restitution curve simulation.
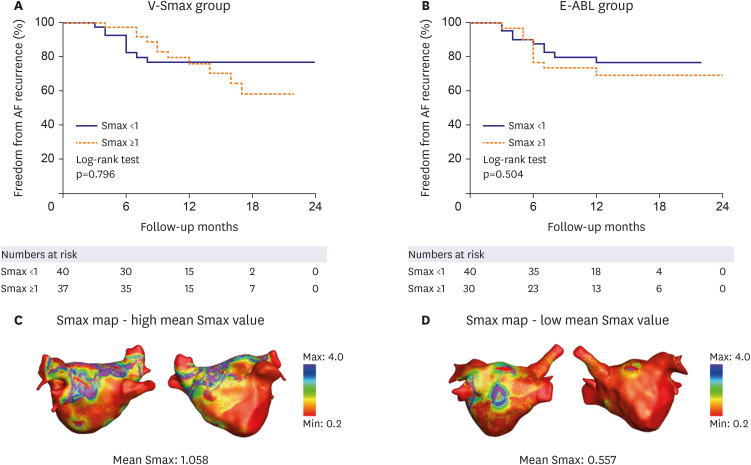
Figure 4 Subgroup analysis according to the Smax level. (A) Freedom from AF in patients with Smax <1 and Smax ≥1 in the V-Smax group. (B) Freedom from AF in patients with Smax <1 and Smax ≥1 in the E-ABL group. Representative virtual Smax maps in patients with high Smax (C) and low Smax (D) values.AF = atrial fibrillation; E-ABL = empirical ablation; V-Smax = virtual high maximal slope of the action potential duration restitution curve simulation.
Reference
-
1. Kannel WB, Abbott RD, Savage DD, McNamara PM. Epidemiologic features of chronic atrial fibrillation: the Framingham study. N Engl J Med. 1982; 306:1018–1022. PMID: 7062992.2. Packer DL, Mark DB, Robb RA, et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. 2019; 321:1261–1274. PMID: 30874766.3. Kim D, Yang PS, Sung JH, et al. Less dementia after catheter ablation for atrial fibrillation: a nationwide cohort study. Eur Heart J. 2020; 41:4483–4493. PMID: 33022705.4. Verma A, Jiang CY, Betts TR, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015; 372:1812–1822. PMID: 25946280.5. Pak HN, Park JW, Yang SY, et al. Cryoballoon versus high-power, short-duration radiofrequency ablation for pulmonary vein isolation in patients with paroxysmal atrial fibrillation: a single-center, prospective, randomized study. Circ Arrhythm Electrophysiol. 2021; 14:e010040. PMID: 34465132.6. Lee JM, Shim J, Park J, et al. The electrical isolation of the left atrial posterior wall in catheter ablation of persistent atrial fibrillation. JACC Clin Electrophysiol. 2019; 5:1253–1261. PMID: 31753429.7. Narayan SM, Krummen DE, Shivkumar K, Clopton P, Rappel WJ, Miller JM. Treatment of atrial fibrillation by the ablation of localized sources: CONFIRM (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation) trial. J Am Coll Cardiol. 2012; 60:628–636. PMID: 22818076.8. Kim IS, Lim B, Shim J, et al. Clinical usefulness of computational modeling-guided persistent atrial fibrillation ablation: updated outcome of multicenter randomized study. Front Physiol. 2019; 10:1512. PMID: 31920716.9. Shim J, Hwang M, Song JS, et al. Virtual in-silico modeling guided catheter ablation predicts effective linear ablation lesion set for longstanding persistent atrial fibrillation: multicenter prospective randomized study. Front Physiol. 2017; 8:792. PMID: 29075201.10. Baek YS, Kwon OS, Lim B, et al. Clinical outcomes of computational virtual mapping-guided catheter ablation in patients with persistent atrial fibrillation: a multicenter prospective randomized clinical trial. Front Cardiovasc Med. 2021; 8:772665. PMID: 34957255.11. Krummen DE, Bayer JD, Ho J, et al. Mechanisms of human atrial fibrillation initiation: clinical and computational studies of repolarization restitution and activation latency. Circ Arrhythm Electrophysiol. 2012; 5:1149–1159. PMID: 23027797.12. Narayan SM, Kazi D, Krummen DE, Rappel WJ. Repolarization and activation restitution near human pulmonary veins and atrial fibrillation initiation: a mechanism for the initiation of atrial fibrillation by premature beats. J Am Coll Cardiol. 2008; 52:1222–1230. PMID: 18926325.13. Qu Z, Weiss JN, Garfinkel A. Cardiac electrical restitution properties and stability of reentrant spiral waves: a simulation study. Am J Physiol. 1999; 276:H269–H283. PMID: 9887041.14. Weiss JN, Garfinkel A, Karagueuzian HS, Qu Z, Chen PS. Chaos and the transition to ventricular fibrillation: a new approach to antiarrhythmic drug evaluation. Circulation. 1999; 99:2819–2826. PMID: 10351978.15. Kim BS, Kim YH, Hwang GS, et al. Action potential duration restitution kinetics in human atrial fibrillation. J Am Coll Cardiol. 2002; 39:1329–1336. PMID: 11955851.16. Lim B, Kim J, Hwang M, et al. In situ procedure for high-efficiency computational modeling of atrial fibrillation reflecting personal anatomy, fiber orientation, fibrosis, and electrophysiology. Sci Rep. 2020; 10:2417. PMID: 32051487.17. Kim TH, Uhm JS, Kim JY, Joung B, Lee MH, Pak HN. Does additional electrogram-guided ablation after linear ablation reduce recurrence after catheter ablation for longstanding persistent atrial fibrillation? A prospective randomized study. J Am Heart Assoc. 2017; 6:6.18. Marrouche NF, Wilber D, Hindricks G, et al. Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: the DECAAF study. JAMA. 2014; 311:498–506. PMID: 24496537.19. Lim B, Hwang M, Song JS, et al. Effectiveness of atrial fibrillation rotor ablation is dependent on conduction velocity: an in-silico 3-dimensional modeling study. PLoS One. 2017; 12:e0190398. PMID: 29287119.20. Li C, Lim B, Hwang M, et al. The spatiotemporal stability of dominant frequency sites in in-silico modeling of 3-dimensional left atrial mapping of atrial fibrillation. PLoS One. 2016; 11:e0160017. PMID: 27459377.21. Hwang I, Park JW, Kwon OS, et al. Spatial changes in the atrial fibrillation wave-dynamics after using antiarrhythmic drugs: a computational modeling study. Front Physiol. 2021; 12:733543. PMID: 34630153.22. Park JW, Lim B, Hwang I, et al. Restitution slope affects the outcome of dominant frequency ablation in persistent atrial fibrillation: CUVIA-AF2 post-hoc analysis based on computational modeling study. Fron Cardiovasc Med. 2022; 9:838646.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Large Circular Ring Catheter Ablation Versus Anatomically Guided Ablation of Atrial Fibrillation: Back to the Future for Successful Catheter Ablation of Atrial Fibrillation?
- A Case of Chronic Radiodermatitis following Radiofrequency Catheter Ablation for Atrial Fibrillation
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
- The Mechanism of and Preventive Therapy for Stroke in Patients with Atrial Fibrillation
- Catheter Ablation of Atrial Fibrillation
