J Korean Med Sci.
2022 Jul;37(28):e222. 10.3346/jkms.2022.37.e222.
Clinical Features and Risk Factors of Adrenal Insufficiency in Patients With Cancer Admitted to the HospitalistManaged Medical Unit
- Kwon MK
 1,2
1,2 - Kim J1,2
- Ahn J1,2,3
- Woo CY1,2
- Kim H1,2
- Oh HS1,2
- Lee M1,2
- Hwang S1,2
- Park KH1,2
- Lee YH1,2
- Yu J2
- Kang S2
- Son HJ1,2,4
- Affiliations
-
- 1Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Medical Hospitalist Unit, Asan Medical Center, Seoul, Korea
- 3Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea
- 4Department of Infectious Diseases, Uijeongbu Eulji Medical Center, University of Eulji College of Medicine, Uijeongbi, Korea
- KMID: 2531803
- DOI: http://doi.org/10.3346/jkms.2022.37.e222
Abstract
- Background
The symptoms of adrenal insufficiency (AI) overlap with the common effects of advanced cancer and chemotherapy. Considering that AI may negatively affect the overall prognosis of cancer patients if not diagnosed in a timely manner, we analyzed the incidence, risk factors, and predictive methods of AI in cancer patients.
Methods
We retrospectively analyzed the medical records of 184 adult patients with malignancy who underwent a rapid adrenocorticotrophic hormone stimulation test in the medical hospitalist units of a tertiary hospital. Their baseline characteristics and clinical features were evaluated, and the risk factors for AI were identified using logistic regression analysis.
Results
Of the study patients, 65 (35%) were diagnosed with AI, in whom general weakness (63%) was the most common symptom. Multivariate logistic regression showed that eosinophilia (adjusted odds ratio [aOR], 4.28; 95% confidence interval [CI], 1.10–16.63; P = 0.036), history of steroid use (aOR, 2.37; 95% CI, 1.10–5.15; P = 0.028), and history of megestrol acetate use (aOR, 2.71; 95% CI, 1.38–5.33; P = 0.004) were associated with AI. Baseline cortisol levels of 6.2 μg/dL and 12.85 μg/dL showed a specificity of 95.0% and 95.4% for AI diagnosis, respectively.
Conclusion
AI was found in about one-third of patients with cancer who showed general symptoms that may be easily masked by cancer or chemotherapy, suggesting that clinical suspicion of AI is important while treating cancer patients. History of corticosteroids or megestrol acetate were risk factors for AI and eosinophilia was a pre-test predictor of AI. Baseline cortisol level appears to be a useful adjunct marker for AI.
Figure
-
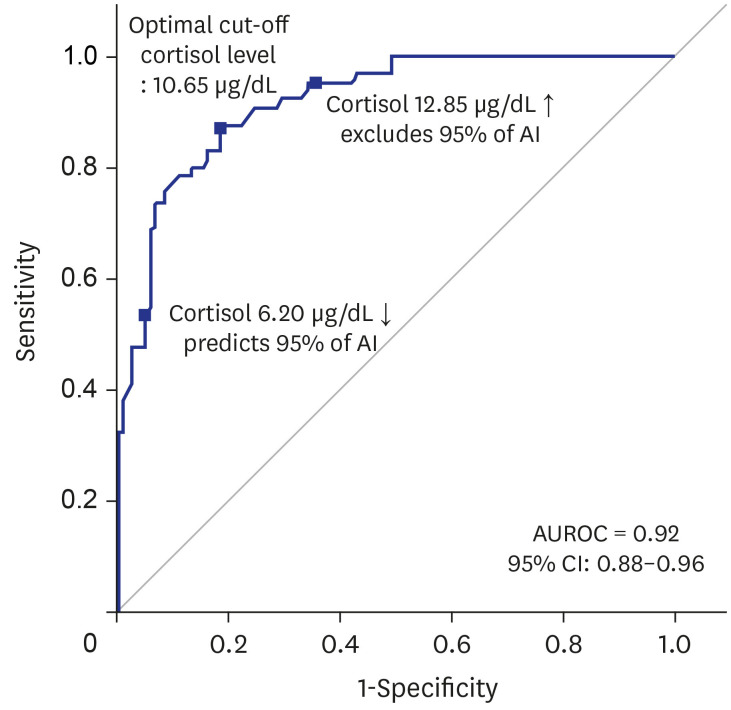
Fig. 1 Receiver operating characteristic curve of baseline cortisol for predicting adrenal insufficiency in hospitalized patients with malignancy.AI = adrenal insufficiency, AUROC = area under receiver operating characteristic, CI = confidence interval.
Cited by 1 articles
-
Time to Care for Adrenal Insufficiency in Cancer Patients
Jung Hee Kim
J Korean Med Sci. 2022;37(28):e232. doi: 10.3346/jkms.2022.37.e232.
Reference
-
1. Bergthorsdottir R, Leonsson-Zachrisson M, Odén A, Johannsson G. Premature mortality in patients with Addison’s disease: a population-based study. J Clin Endocrinol Metab. 2006; 91(12):4849–4853. PMID: 16968806.
Article2. Bensing S, Brandt L, Tabaroj F, Sjöberg O, Nilsson B, Ekbom A, et al. Increased death risk and altered cancer incidence pattern in patients with isolated or combined autoimmune primary adrenocortical insufficiency. Clin Endocrinol (Oxf). 2008; 69(5):697–704. PMID: 18727712.
Article3. Biddie SC, Conway-Campbell BL, Lightman SL. Dynamic regulation of glucocorticoid signalling in health and disease. Rheumatology (Oxford). 2012; 51(3):403–412. PMID: 21891790.
Article4. Laugesen K, Broersen LH, Hansen SB, Dekkers OM, Sørensen HT, Jorgensen JO. Management of endocrine disease: glucocorticoid-induced adrenal insufficiency: replace while we wait for evidence? Eur J Endocrinol. 2021; 184(4):R111–R122. PMID: 33449912.
Article5. Almeida MQ, Mendonca BB. Adrenal insufficiency and glucocorticoid use during the COVID-19 pandemic. Clinics (Sao Paulo). 2020; 75:e2022. PMID: 32555949.
Article6. Karangizi AH, Al-Shaghana M, Logan S, Criseno S, Webster R, Boelaert K, et al. Glucocorticoid induced adrenal insufficiency is common in steroid treated glomerular diseases - proposed strategy for screening and management. BMC Nephrol. 2019; 20(1):154. PMID: 31060510.
Article7. Redman BG, Pazdur R, Zingas AP, Loredo R. Prospective evaluation of adrenal insufficiency in patients with adrenal metastasis. Cancer. 1987; 60(1):103–107. PMID: 3581024.
Article8. Mitchell J, Barbosa G, Tsinberg M, Milas M, Siperstein A, Berber E. Unrecognized adrenal insufficiency in patients undergoing laparoscopic adrenalectomy. Surg Endosc. 2009; 23(2):248–254. PMID: 19037697.
Article9. Hirai H, Kuwana K, Kusano Y. Late onset adrenal insufficiency after adrenalectomy due to latent nonclassical 21-hydroxylase deficiency: a case report. Medicine (Baltimore). 2018; 97(33):e11888. PMID: 30113485.10. Percik R, Shlomai G, Tirosh A, Tirosh A, Leibowitz-Amit R, Eshet Y, et al. Isolated autoimmune adrenocorticotropic hormone deficiency: from a rare disease to the dominant cause of adrenal insufficiency related to check point inhibitors. Autoimmun Rev. 2020; 19(2):102454. PMID: 31838158.
Article11. Oray M, Abu Samra K, Ebrahimiadib N, Meese H, Foster CS. Long-term side effects of glucocorticoids. Expert Opin Drug Saf. 2016; 15(4):457–465. PMID: 26789102.
Article12. Munro V, Elnenaei M, Doucette S, Clarke DB, Imran SA. The effect of time of day testing and utility of 30 and 60 minute cortisol values in the 250 mcg ACTH stimulation test. Clin Biochem. 2018; 54:37–41. PMID: 29458002.
Article13. Reddy P. Clinical approach to adrenal insufficiency in hospitalised patients. Int J Clin Pract. 2011; 65(10):1059–1066. PMID: 21762316.
Article14. Kim J. The impact of hospitalist care in Korea. J Korean Med Sci. 2019; 34(25):e177. PMID: 31243936.
Article15. Kuang FL. Approach to patients with eosinophilia. Med Clin North Am. 2020; 104(1):1–14. PMID: 31757229.
Article16. Deng R, Bumbaca D, Pastuskovas CV, Boswell CA, West D, Cowan KJ, et al. Preclinical pharmacokinetics, pharmacodynamics, tissue distribution, and tumor penetration of anti-PD-L1 monoclonal antibody, an immune checkpoint inhibitor. MAbs. 2016; 8(3):593–603. PMID: 26918260.
Article17. Sunshine J, Taube JM. PD-1/PD-L1 inhibitors. Curr Opin Pharmacol. 2015; 23:32–38. PMID: 26047524.
Article18. Li B, Chan HL, Chen P. Immune checkpoint inhibitors: basics and challenges. Curr Med Chem. 2019; 26(17):3009–3025. PMID: 28782469.
Article19. Ahn SY, Kim HK, Kang HC, Kim M, Song GY, Jung SH, et al. Adrenal insufficiency in hospitalized patients with multiple myeloma. Leuk Lymphoma. 2021; 62(2):501–503. PMID: 33135942.
Article20. Yoon JH, Ahn SY, Jung SH, Lee JJ, Choi W, Park JY, et al. Prevalence and risk factors for adrenal insufficiency in patients with multiple myeloma receiving long-term chemotherapy including corticosteroids: a retrospective cohort study. Biomed Res Int. 2021; 2021:2330417. PMID: 34938804.
Article21. Mouloudi E, Katsanoulas K, Aslanidis TH, Lampiri CL, Papageorgiou CH, Tholioti TH, et al. Eosinophilia: an early marker of adrenal insufficiency in critically ill patients with septic shock? Greek e J Perioper Med. 2018; 17(a):61–70.22. Angelis M, Yu M, Takanishi D, Hasaniya NW, Brown MR. Eosinophilia as a marker of adrenal insufficiency in the surgical intensive care unit. J Am Coll Surg. 1996; 183(6):589–596. PMID: 8957461.23. Beishuizen A, Vermes I, Hylkema BS, Haanen C. Relative eosinophilia and functional adrenal insufficiency in critically ill patients. Lancet. 1999; 353(9165):1675–1676. PMID: 10335792.
Article24. Miller WL. The hypothalamic-pituitary-adrenal axis: a brief history. Horm Res Paediatr. 2018; 89(4):212–223. PMID: 29719288.
Article25. Paragliola RM, Papi G, Pontecorvi A, Corsello SM. Treatment with synthetic glucocorticoids and the hypothalamus-pituitary-adrenal axis. Int J Mol Sci. 2017; 18(10):E2201. PMID: 29053578.
Article26. Gjerstad JK, Lightman SL, Spiga F. Role of glucocorticoid negative feedback in the regulation of HPA axis pulsatility. Stress. 2018; 21(5):403–416. PMID: 29764284.
Article27. García-Castells AM, Argente-Pla M, García-Malpartida K, Querol-Ripoll R, Merino-Torres JF. Adrenal insufficiency induced by megestrol acetate: report of two cases. Endocrinol Nutr. 2015; 62(10):515–516. PMID: 26250842.
Article28. González Villarroel P, Fernández Pérez I, Páramo C, Gentil González M, Carnero López B, Vázquez Tuñas ML, et al. Megestrol acetate-induced adrenal insufficiency. Clin Transl Oncol. 2008; 10(4):235–237. PMID: 18411198.
Article29. Bulchandani D, Nachnani J, Amin A, May J. Megestrol acetate-associated adrenal insufficiency. Am J Geriatr Pharmacother. 2008; 6(3):167–172. PMID: 18775392.
Article30. Manosroi W, Phimphilai M, Khorana J, Atthakomol P. Diagnostic performance of basal cortisol level at 0900-1300h in adrenal insufficiency. PLoS One. 2019; 14(11):e0225255. PMID: 31738804.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Characteristics of Patients with Adrenal Insufficiency and Fever
- A Case of Adrenal Tuberculosis Combined with Tuberculous Peritonitis-Induced Adrenal Crisis
- Adrenal Insufficiency in Patients with Rotator Cuff Tear: Prevalence, Risk Factors and Influence on Outcome
- Secondary Adrenal Insufficiency Associated with Megestrol Acetate in a Patient with Lung Cancer
- Relative Adrenal Insufficiency in Postresuscitation Patients
