Morphometric characteristics of the aorta and heart in situs inversus totalis
- Affiliations
-
- 1Department of Normal Anatomy, Danylo Halytsky Lviv National Medical University, Lviv, Ukraine
- 2Ukrainian-Polish Heart Center “Lviv”, Lviv, 3 Lviv Regional Clinical Hospital, Lviv, Ukraine
- KMID: 2531214
- DOI: http://doi.org/10.5115/acb.21.252
Abstract
- Situs inversus totalis is a rare condition of visceral transposition in thoracic and abdominal cavities. Computed tomography (CT)-based morphometric analysis of the cardiovascular system prior to the surgery helps to describe vessel topography and size, choose the right surgical insertion site, avoid vessel trauma, and prevent hemorrhage during surgical intervention. We present a case report of situs inversus totalis detected incidentally in a 74-year-old male with the acute abdominal syndrome. Appropriate detailed aorta measurements are used to choose an adequate size of the aortic prosthesis during open surgical repair or endovascular aneurysm repair. An accurate assessment of the vessels on CT scans assists in consideration of the catheter diameter and the most reliable cannulation site. Vessel size correlates with morphological conditions (kinking, stenosis, occlusion), which may be considered a risk of organ malperfusion. The anatomical analysis prior to surgery in different anatomical variations may ensure patient safety and predict complications.
Keyword
Figure
-
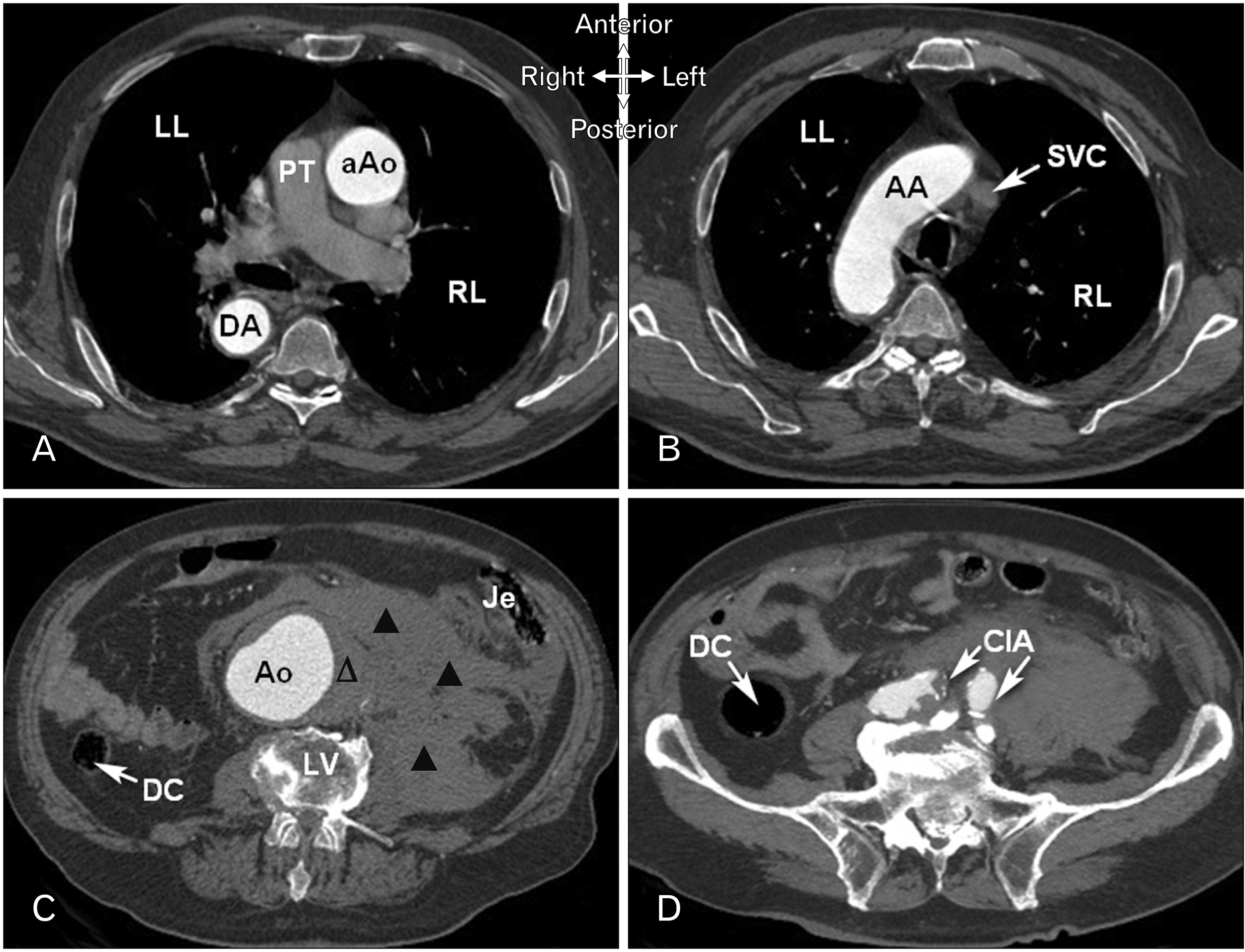
Fig. 1 Serial two-dimensional axial views showing slices of the aorta. (A) The series demonstrates the location of the ascending aorta (aAo) to the right of the pulmonary trunk (PT). The aAo is located to the left of the vertebral column; the descending aorta (DA) is located to the right of the vertebral column. (B) The aortic arch (AA) is to the right of the superior vena cava (SVC). (C) Computed tomography image of the abdomen under the renal arteries level. Abdominal aortic aneurysm (Ao) located in the center with intravascular thrombus on the left (∆) with dissection and retroperitoneal hematoma (▲); lumbar vertebra (LV); right-sidedness of the jejunum (Je); right-sidedness of the DC. (D) Common iliac artery (CIA) with saccular partially thrombosed aneurysm right-sidedness DC. DC, descending colon; RL, right lung; LL, left lung.
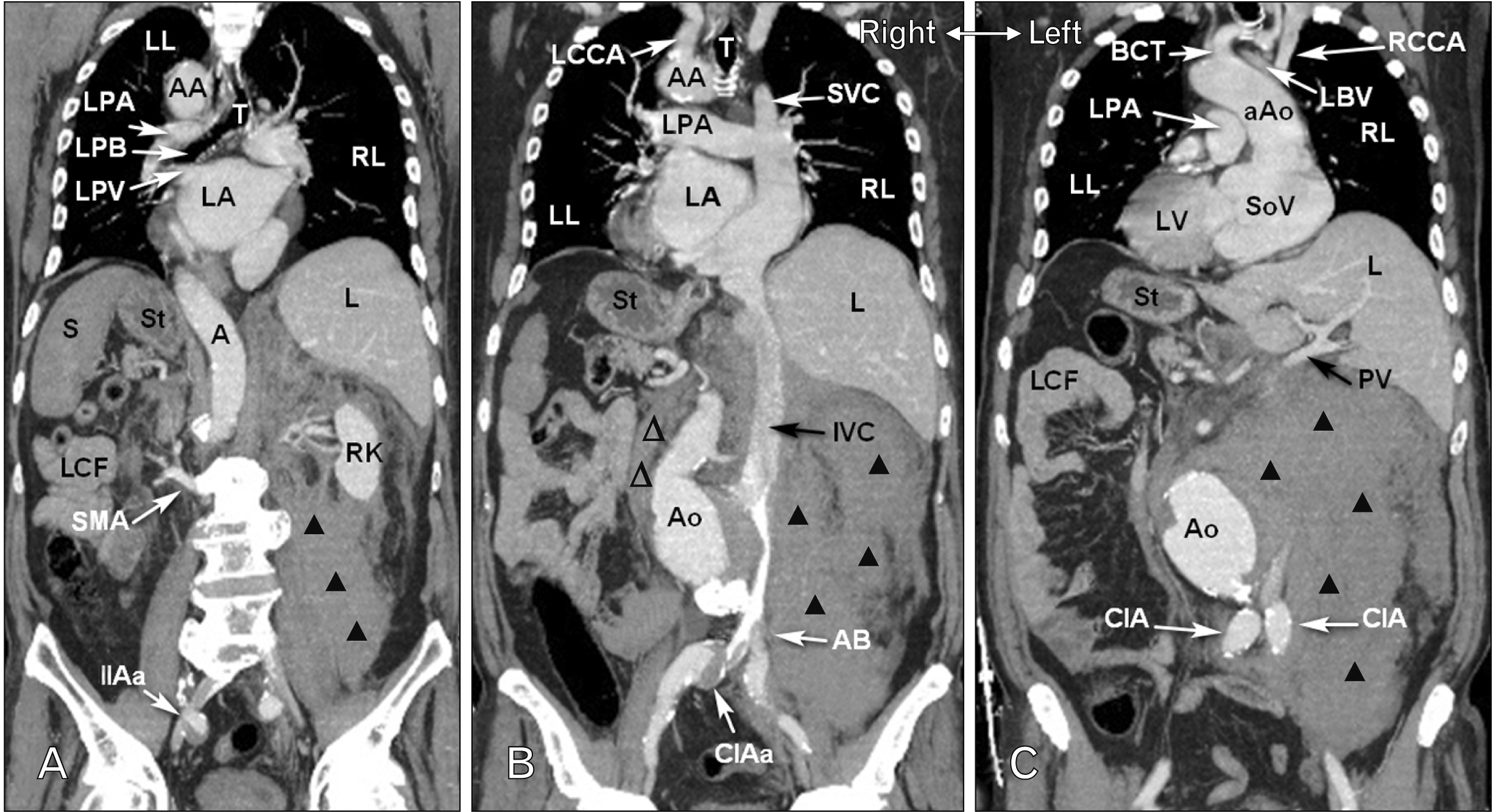
Fig. 2 (A–C) A curved multiplanar reformatted view demonstrates the full course of the aorta in situs inversus totalis. Right-left inversion of viscera in thoracic cavity and abdominal cavity. (A) Retroperitoneal hematoma (▲). (B) Intravascular thrombus (∆) in the abdominal aortic aneurysm (Ao); retroperitoneal hematoma (▲). T, trachea; AA, aortic arch; LPA, left pulmonary artery; LPB, left primary bronchus; LPV, left pulmonary vein; LA, left atrium; RL, right lung; LL, left lung; A, abdominal aorta; S, spleen; St, stomach; L, liver; LCF, left colic flexure (splenic); SMA, superior mesenteric artery; RK, right kidney; IIAa, internal iliac artery aneurysm; LCCA, left common carotid artery; SVC, superior vena cava; IVC, inferior vena cava; AB, aorta bifurcation to iliac arteries; CIAa, common iliac artery aneurysm. LV, left ventricle; SoV, sinuses of Valsalva; aAo, ascending aorta; BCT, brachiocephalic trunk; LBV, left brachiocephalic vein; RCCA, right common carotid artery; PV, portal vein; CIA, common iliac artery.
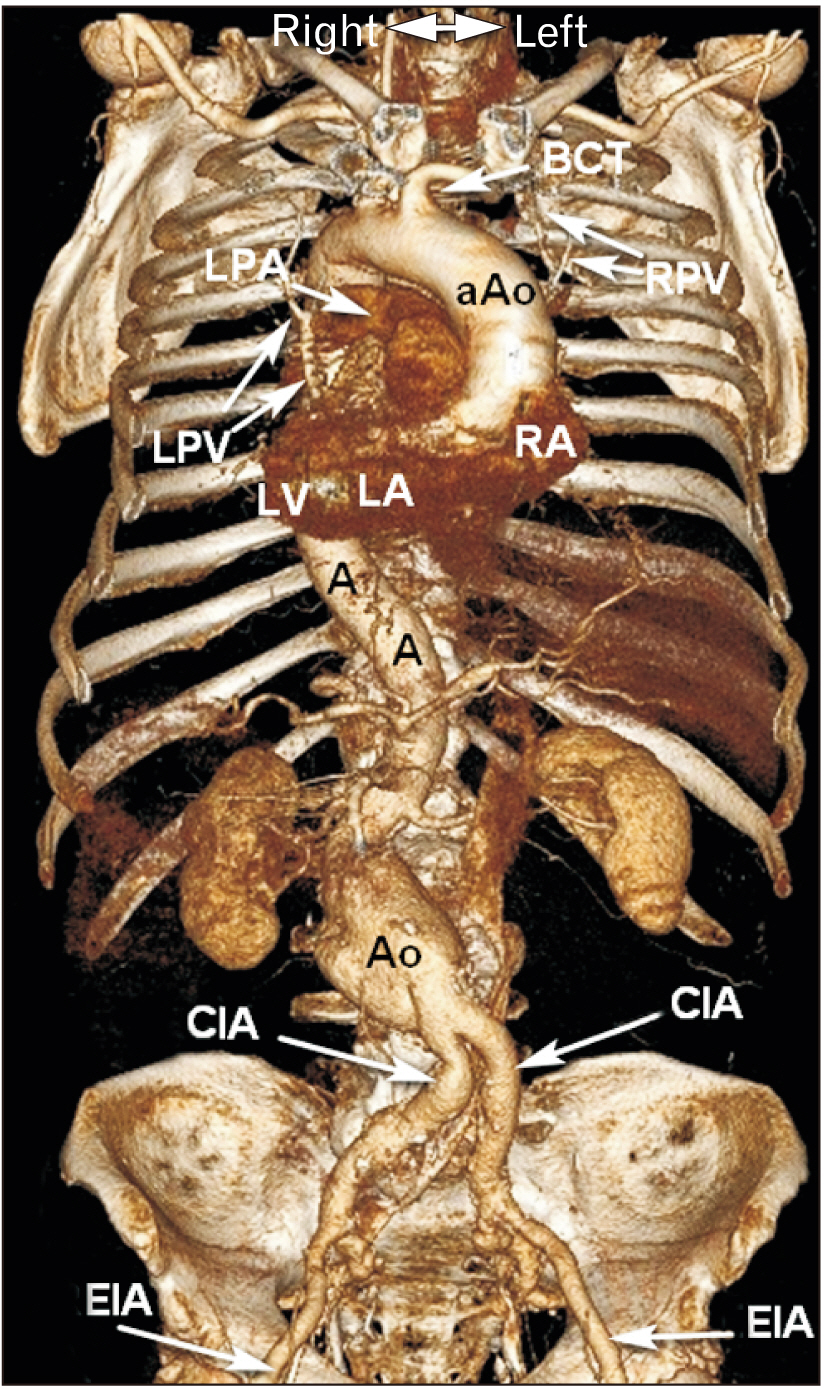
Fig. 3 Volumetric rendering demonstrates dextrocardia and the full course of the aorta till the bifurcation in situs inversus totalis. aAo, ascending aorta; LV, left ventricle; RA, right atrium; BCT, brachiocephalic trunk; LPA, left pulmonary artery; RPA, right pulmonary artery; A, abdominal aorta; Ao, abdominal aortic aneurysm; CIA, common iliac artery; EIA, external iliac artery.
Cited by 1 articles
-
Vascular anatomy and their variations in Situs inversus totalis using postmortem computed tomographic angiography
Dawa Zangpo, Hironobu Nakane, Morio Iino
Anat Cell Biol. 2023;56(1):155-159. doi: 10.5115/acb.22.213.
Reference
-
References
1. Huss-Bawab J, Szymanski LJ. 2018; Situs inversus totalis. Acad Forensic Pathol. 8:957–63. DOI: 10.1177/1925362118821495. PMID: 31240085. PMCID: PMC6491533.
Article2. Tsoucalas G, Thomaidis V, Fiska A. 2019; Situs inversus totalis: always recall the uncommon. Clin Case Rep. 7:2575–6. DOI: 10.1002/ccr3.2433. PMID: 31893103. PMCID: PMC6935672. PMID: 16b1ea8adec040b5973b54fb0a83fca5.
Article3. Ramavathu KVM. 2021; Imaging findings in a case of situs inversus totalis. BJR Case Rep. 7:20200202. DOI: 10.1259/bjrcr.20200202. PMID: 35047197. PMCID: PMC8749394.
Article4. Swarhib M, Das S, Htwe O. 2013; A case of situs inversus totalis: embryological and clinical considerations. Int Med J. 20:264–5.5. Riera Hernández C, Pérez Ramírez P, Esteban Gracia C, Jiménez Olivera MA, Llagostera Pujol S. 2015; Situs inversus totalis and abdominal aortic aneurysm: surgical repair of an extremely uncommon association. Int J Surg Case Rep. 10:216–8. DOI: 10.1016/j.ijscr.2015.04.007. PMID: 25884612. PMCID: PMC4430184.
Article6. Liu Y, Wu L, Chen Y, Li D, Jiang J, Zhong W, Cao Y. 2017; Delayed diagnosis of abdominal pain in patient with situs inversus totalis in emergency department: a case report. Medicine (Baltimore). 96:e9028. DOI: 10.1097/MD.0000000000009028. PMID: 29245291. PMCID: PMC5728906.7. Elfanagely O, Elfanagely Y, Pratt A. 2021; A rare anatomical variation complicating a diffuse abdominal pain presentation: a case report of colonic perforation in situs inversus totalis. Int J Surg Case Rep. 87:106456. DOI: 10.1016/j.ijscr.2021.106456. PMID: 34597972. PMCID: PMC8488479.
Article8. Chan YC, Ting AC, Qing KX, Cheng SW. 2010; Successful endovascular infrarenal aneurysm repair in a patient with situs inversus totalis. Ann Vasc Surg. 24:1134.e5–7. DOI: 10.1016/j.avsg.2010.02.044. PMID: 20472388.
Article9. Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, Evangelista A, Falk V, Frank H, Gaemperli O, Grabenwöger M, Haverich A, Iung B, Manolis AJ, Meijboom F, Nienaber CA, Roffi M, Rousseau H, Sechtem U, Sirnes PA, Allmen RS, Vrints CJ. 2014; 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 35:2873–926. Erratum in: Eur Heart J 2015;36: 2779. DOI: 10.1093/eurheartj/ehv178. PMID: 26129948.10. Sadler T. 2017; Establishing the embryonic axes: prime time for teratogenic insults. J Cardiovasc Dev Dis. 4:15. DOI: 10.3390/jcdd4030015. PMID: 29367544. PMCID: PMC5715709.
Article11. Komutrattananont P, Mahakkanukrauh P, Das S. 2019; Morphology of the human aorta and age-related changes: anatomical facts. Anat Cell Biol. 52:109–14. DOI: 10.5115/acb.2019.52.2.109. PMID: 31338225. PMCID: PMC6624342.
Article12. Wang LJ, Prabhakar AM, Kwolek CJ. 2018; Current status of the treatment of infrarenal abdominal aortic aneurysms. Cardiovasc Diagn Ther. 8(Suppl 1):S191–9. DOI: 10.21037/cdt.2017.10.01. PMID: 29850431. PMCID: PMC5949587.
Article13. Téllez-Beltrán D, González-Muñoz A, Barón-Cifuentes V, Pradilla-Gómez JM. 2020; Abdominal aortic aneurysm in a patient with situs inversus totalis. Cir Cir. 88(Suppl 1):79–82. DOI: 10.24875/CIRU.20001581. PMID: 32963397.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Neonatal Duodenal Obstruction Associated with Situs Inversus Totalis: A Case Report
- Single Port Laparoscopic Cholecystectomy in a Patient with Situs Inversus Totalis: A Case Report
- Laparoscopic cholecystectomy in a case of situs inversus totalis: a review of technical challenges and adaptations
- Laparoscopic Low Anterior Resection in a Rectal Cancer Patient with Situs Inversus Totalis: A Case Report
- A Case of Pregnancy Complicated by Situs Inversus Totalis Fetus in Overt Diabetic Woman
