Ruptured Spinal Dermoid Cysts with Lipid Droplets into the Syrinx Cavity : Reports of Fourteen Cases
- Affiliations
-
- 1Department of Neurosurgery, The First Medical Centre, Chinese PLA General Hospital, Beijing, China
- 2Department of Neurosurgery, The Third Medical Centre, Chinese PLA General Hospital, Beijing, China
- KMID: 2529588
- DOI: http://doi.org/10.3340/jkns.2021.0159
Abstract
Objective
: Dermoid cysts are uncommon in spinal cord tumors, and the phenomenon of their spontaneous rupture into the syrinx cavity is quite rare. We aimed to analyze the imaging characteristics and etiologies, and propose some surgical strategies, for this uncommon phenomenon.
Methods
: We retrospectively reviewed 14 cases with spinal dermoid cysts that ruptured into the cervical and thoracic syrinx cavity. There were six male and eight female cases, aged 21 to 46 years, who had lipid droplets in the syrinx cavity from C1 to L3. The dermoid cysts were always located at the conus. Based on patients’ complaints, clinical manifestations, and imaging results, we adopted tumor excision and/or syrinx cavity aspiration in one stage or multiple stages.
Results
: Three patients had only a syrinx cavity aspiration surgery due to a history of dermoid cyst excision. Eight patients had dermoid cyst resection and syrinx cavity aspiration in one stage. One patient was operated upon in two stages due to the development of new symptoms at nine months follow-up. Two patients underwent only tumor resection since they did not show similar symptoms or signs caused by the cervicothoracic syrinx. The axial magnetic resonance imaging indicated that the lipid droplets were always not at the center but were eccentric. The clinical effect was satisfactory during the follow-up period in this group.
Conclusion
: The lipid droplets filled the spinal syrinx cavity, not entirely confined to the central canal. Based on the chief complaints and associated signs, we adopted different surgical strategies and had satisfactory clinical results.
Keyword
Figure
-
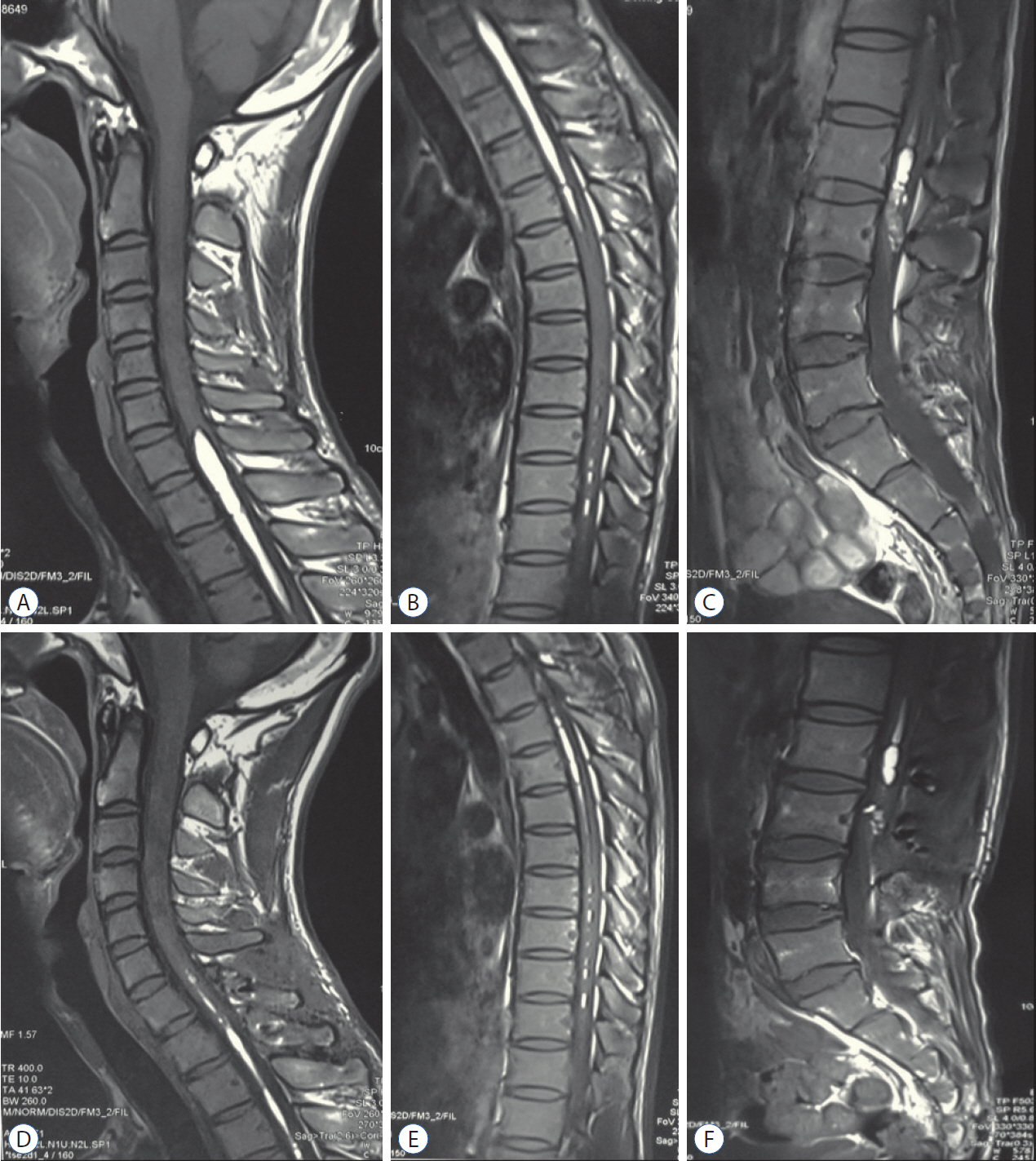
Fig. 1. Case 6. Preoperative magnetic resonance imaging (MRI) revealed a tethered conus lesion with heterogeneous hyperintense on lumbosacral T1-weighted images, and homogeneously spindle or linear signal on the cervical and thoracic spinal cord (A-C). Postoperative MRI showed subtotal resection of the conus dermoid cyst, and lipid droplets reduced significantly in the cervical and thoracic regions (D-F).
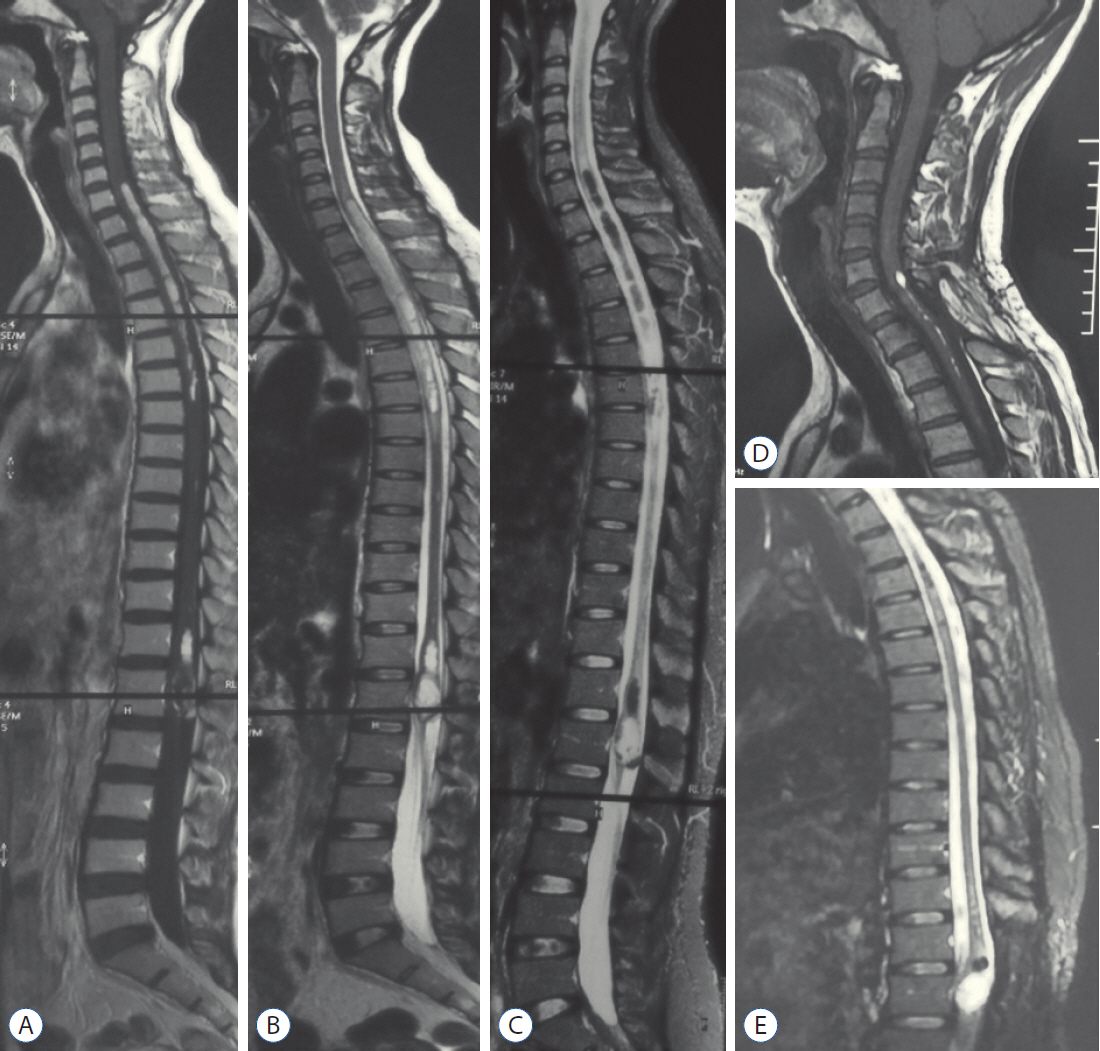
Fig. 2. Case 3. The preoperative whole spine magnetic resonance imaging images revealed C7-T6 intramedullary lipid droplets (short T1-weighted and long T2-weighted signal on A and B), which were suppressed on fat-suppressed sequences (C). The heterogeneous signals were seen at the level of conus medullaris, indicating a possible dermoid cyst. After conus tumor surgery at another clinical center, the patient was admitted to our hospital and had a T1 syrinx cavity aspiration surgery. The cervical intramedullary lipid droplets almost disappeared, and the conus dermoid cyst showed recurrent signs even though the patient did not have apparent symptoms at 72 months follow-up (D and E).

Fig. 3. Case 1. Preoperative magnetic resonance imaging (MRI) showed short-T1 cervical intramedullary lesion and mixed-signal lumbar dermoid cyst (A and B). Postoperative MRI revealed the tumor subtotal resection in one stage (C and D).

Fig. 4. Intraoperative views showed ivory lipid droplets flowed out (A; red arrow) after cervical spinal cord myelotomy; revealed yellowish dermoid cyst contents exposure (B; red arrow).
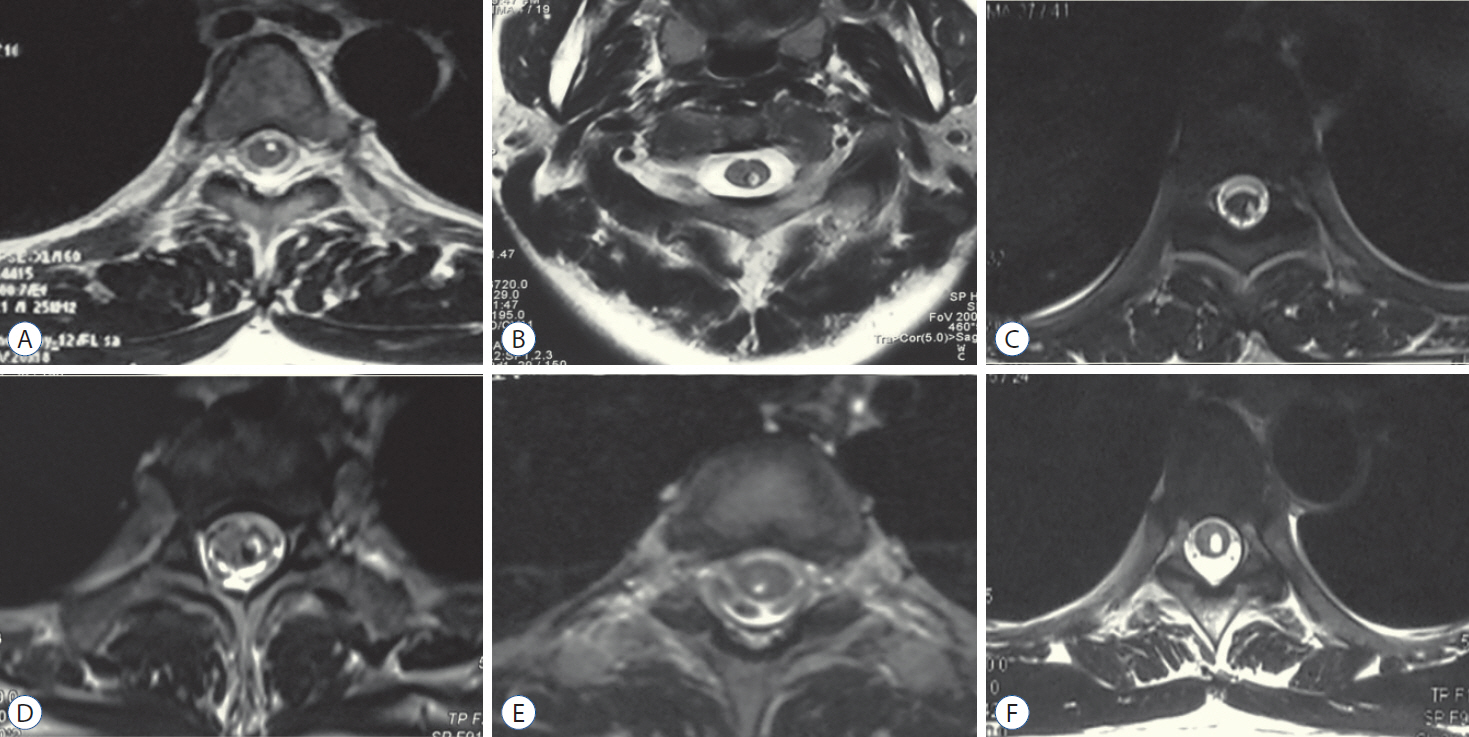
Fig. 5. A-F : The axial images indicated that the lipid droplets were always eccentric, not only confined to the central canal, and can be distributed in any direction.
Reference
-
References
1. Altay H, Kitiş O, Calli C, Yünten N. A spinal dermoid tumor that ruptured into the subarachnoidal space and syrinx cavity. Diagn Interv Radiol. 12:171–173. 2006.2. Bishnoi I, Bishnoi S, Gahlawat N, Bhardwaj L, Duggal G, Singal G, et al. Management of a rare case of intraventricular ruptured dermoid cyst and chemical meningitis. Br J Neurosurg. 19:1–4. 2018.
Article3. Calabrò F, Capellini C, Jinkins JR. Rupture of spinal dermoid tumors with spread of fatty droplets in the cerebrospinal fluid pathways. Neuroradiology. 42:572–579. 2000.
Article4. Falavigna A, Righesso O, Teles AR. Concomitant dermoid cysts of conus medullaris and cauda equina. Arq Neuropsiquiatr. 67(2A):293–296. 2009.
Article5. Fernández-de Thomas RJ, Vicenty-Padilla JC, Sánchez-Jiménez JG, Labat EJ, Carballo-Cuello CM, De Jesús O, et al. Obstructive hydrocephalus and chemical meningitis secondary to a ruptured spinal epidermoid cyst. World Neurosurg. 132:173–176. 2019.
Article6. Goyal A, Singh D, Singh AK, Gupta V, Sinha S. Spontaneous rupture of spinal dermoid cyst with disseminated lipid droplets in central canal and ventricles. J Neurosurg Sci. 48:63–65. 2004.7. Karaaslan B, Ülkü G, Ucar M, Demirdağ TB, İnan A, Börcek AÖ. Intramedullary dermoid cyst infection mimicking holocord tumor: should radical resection be mandatory?-a case report. Childs Nerv Syst. 32:2249–2253. 2016.
Article8. Karadag D, Karagülle AT, Erden A, Erden I. MR imaging of a ruptured intraspinal dermoid tumour with fat droplets in the central spinal canal. Australas Radiol. 46:444–446. 2002.
Article9. Kasliwal MK, Sinha S, Sharma BS, Garg A. Symptomatic central canal rupture heralding the presence of an asymptomatic conus dermoid. J Neurooncol. 84:39–40. 2007.
Article10. Kuyumcu G, Jhaveri M. Ruptured spinal dermoid cyst. Can J Neurol Sci. 44:601–602. 2017.
Article11. Liu T, Deng X, Xu Y, Xin Y. Spinal dermoid cyst with spontaneous rupture into the syrinx cavity alone. World Neurosurg. 118:e395–e404. 2018.
Article12. Petit-Lacour MC, Lasjaunias P, Iffenecker C, Benoudiba F, Hadj Rabia M, Hurth M, et al. Visibility of the central canal on MRI. Neuroradiology. 42:756–761. 2000.
Article13. Samii M, Klekamp J. Surgical results of 100 intramedullary tumors in relation to accompanying syringomyelia. Neurosurgery. 35:865–873. discussion 873. 1994.
Article14. Sanaullah M, Mumtaz S, Memon AA, Hashim AS, Bashir S. Intramedullary dermoid cyst with relatively atypical symptoms: a case report and review of the literature. J Med Case Rep. 7:104. 2013.
Article15. Scearce TA, Shaw CM, Bronstein AD, Swanson PD. Intraventricular fat from a ruptured sacral dermoid cyst: clinical, radiographic, and pathological correlation. Case report. J Neurosurg. 78:666–668. 1993.
Article16. Watanabe E, Tanaka K, Takeda N, Takayasu H, Yokota K, Watanabe M. Surgical technique to prevent spillage of cyst fluid during operation for cystic ovarian tumors. Pediatr Surg Int. 29:645–649. 2013.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ruptured Conus Medullaris Dermoid Cyst with Fat Droplets in the Central
- Three Cases of Dermoid Cysts of Auriculotemporal Area
- Ruptured Intracranial Dermoid Cyst Associated with Rupture of Cerebral Aneurysm
- Multiple Lumbar Intradural Dermoid Cysts without Spinal Dysraphism
- A Ruptured Dermoid Cyst of the Cavernous Sinus Extending into the Posterior Fossa
