Revascularization Strategies in Patients With ST-Segment Elevation Myocardial Infarction and Multivessel Disease: Is FFR-Guided Strategy Still Valuable?
- Affiliations
-
- 1Division of Cardiovascular Medicine, Department of Internal Medicine, University of Iowa Carver College of Medicine, Iowa City, IA, USA
- 2Department of Internal Medicine and Cardiovascular Center, Seoul National University Hospital, Seoul, Korea
- 3Division of Cardiology, Department of Internal Medicine, Heart Center, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Korea
- 4Division of Cardiology, Department of Internal Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2528022
- DOI: http://doi.org/10.4070/kcj.2021.0416
Abstract
- Several studies have shown the benefit of complete revascularization (CR) over culprit-only percutaneous coronary intervention (PCI) in patients with ST-segment elevated myocardial infarction (STEMI) and multivessel disease (MVD). Nevertheless, optimal strategy to select targets for non-culprit PCI has not been clarified. In this paper, we critically discuss and compare the safety and efficacy of different strategies for CR in patients with STEMI and MVD using a Bayesian network meta-analysis including all previous randomized controlled trials (RCTs). In Bayesian network meta-analysis of 13 RCTs, culprit-only PCI was associated with higher risk of major adverse cardiac events (MACE), compared with angiography-guided or fractional flow reserve (FFR)-guided CR strategies. However, there was no significant difference between angiography-guided and FFR-guided CR strategies in the risk of MACE and its individual components including all-cause death, cardiac death, myocardial infarction (MI), and revascularization. These evidence support that both angiography-guided and FFR-guided complete revascularization strategies would be reasonable treatment option in patients with STEMI and MVD. If the non-culprit lesion is severe on visual assessment, angiography-guided PCI can be considered. If the non-culprit lesion is intermediate in severity or unclear based on visual assessment, FFR-guided strategy can be used as a reliable and objective tool, providing similar benefits with less stents compared with an angiographyguided strategy. Further RCT is needed to evaluate direct comparison between angiographyguided and FFR-guided CR strategies in patients with STEMI and MVD. Ongoing FRAMEAMI trial (NCT02715518) will provide more evidence regarding this issue.
Keyword
Figure
-
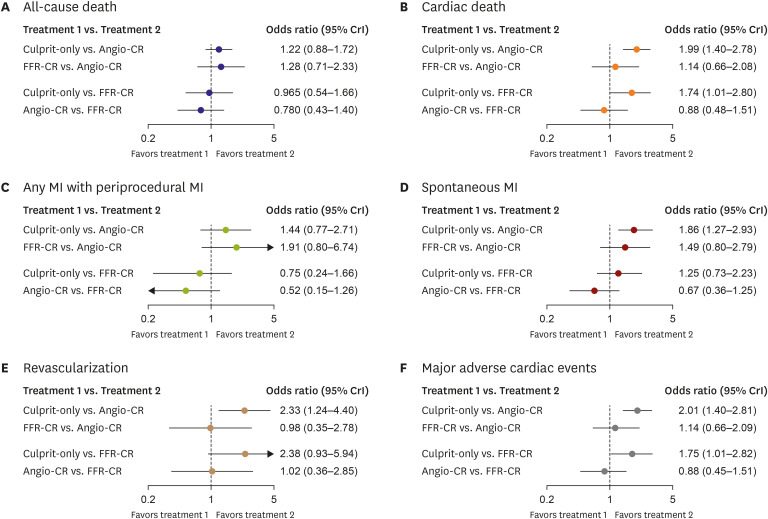
Figure 1 Network meta-analysis comparing culprit-only PCI, FFR-guided, and angiography-guided CR.(A-F) Results from network meta-analysis using the Bayesian extension of the hierarchical random-effects model are presented.ACS = acute coronary syndrome; Angio-CR = angiography-guided complete revascularization; Culprit-only = culprit-only percutaneous coronary intervention; CR = complete revascularization; CrI = credible interval; CVA = cerebrovascular accident; DM = diabetes mellitus; DS = diameter stenosis; EF = ejection fraction; FFR = fractional flow reserve; FFR-CR = fractional flow reserve-guided complete revascularization; HF = heart failure; ID = ischemia-driven; MI = myocardial infarction; NR = not reported; QCA = quantitative coronary angiography; RR = repeat revascularization; VD = vessel disease.
Reference
-
1. Mehta SR, Wood DA, Storey RF, et al. Complete revascularization with multivessel PCI for myocardial infarction. N Engl J Med. 2019; 381:1411–1421. PMID: 31475795.
Article2. Gershlick AH, Banning AS, Parker E, et al. Long-term follow-up of complete versus lesion-only revascularization in STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol. 2019; 74:3083–3094. PMID: 31856964.
Article3. Smits PC, Abdel-Wahab M, Neumann FJ, et al. Fractional flow reserve-guided multivessel angioplasty in myocardial infarction. N Engl J Med. 2017; 376:1234–1244. PMID: 28317428.
Article4. Engstrøm T, Kelbæk H, Helqvist S, et al. Complete revascularisation versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3—PRIMULTI): an open-label, randomised controlled trial. Lancet. 2015; 386:665–671. PMID: 26347918.
Article5. Puymirat E, Cayla G, Simon T, et al. Multivessel PCI Guided by FFR or angiography for myocardial infarction. N Engl J Med. 2021; 385:297–308. PMID: 33999545.
Article6. Di Mario C, Mara S, Flavio A, et al. Single vs multivessel treatment during primary angioplasty: results of the multicentre randomised HEpacoat for cuLPrit or multivessel stenting for Acute Myocardial Infarction (HELP AMI) study. Int J Cardiovasc Intervent. 2004; 6:128–133. PMID: 16146905.
Article7. Dambrink JH, Debrauwere JP, van ’t Hof AW, et al. Non-culprit lesions detected during primary PCI: treat invasively or follow the guidelines? EuroIntervention. 2010; 5:968–975. PMID: 20542783.
Article8. Politi L, Sgura F, Rossi R, et al. A randomised trial of target-vessel versus multi-vessel revascularisation in ST-elevation myocardial infarction: major adverse cardiac events during long-term follow-up. Heart. 2010; 96:662–667. PMID: 19778920.
Article9. Ghani A, Dambrink JH, van ’t Hof AW, Ottervanger JP, Gosselink AT, Hoorntje JC. Treatment of non-culprit lesions detected during primary PCI: long-term follow-up of a randomised clinical trial. Neth Heart J. 2012; 20:347–353. PMID: 22622701.
Article10. Wald DS, Morris JK, Wald NJ, et al. Randomized trial of preventive angioplasty in myocardial infarction. N Engl J Med. 2013; 369:1115–1123. PMID: 23991625.
Article11. Gershlick AH, Khan JN, Kelly DJ, et al. Randomized trial of complete versus lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol. 2015; 65:963–972. PMID: 25766941.
Article12. Hlinomaz AO, Groch L, Poloková K, et al. Multivessel coronary disease diagnosed at the time of primary PCI for STEMI: complete revascularisation versus conservative strategy. Prague-13 trial. Kardiol Rev Int Med. 2015; 17:214–220.13. Zhang J, Wang Q, Yang H, et al. Evaluation of different revascularization strategies for patients with acute myocardial infarction with lesions of multiple coronary arteries after primary percutaneous coronary intervention and its economic evaluation. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015; 27:169–174. PMID: 25757964.14. Hamza M, Mahmoud N, Elgendy IY. A randomized trial of complete versus culprit-only revascularization during primary percutaneous coronary intervention in diabetic patients with acute ST elevation myocardial infarction and multi vessel disease. J Interv Cardiol. 2016; 29:241–247. PMID: 27245121.
Article15. Calviño-Santos R, Estévez-Loureiro R, Peteiro-Vázquez J, et al. Angiographically guided complete revascularization versus selective stress echocardiography-guided revascularization in patients with ST-segment-elevation myocardial infarction and multivessel disease: the CROSS-AMI randomized clinical trial. Circ Cardiovasc Interv. 2019; 12:e007924. PMID: 31554422.
Article16. Smits PC, Laforgia PL, Abdel-Wahab M, et al. Fractional flow reserve-guided multivessel angioplasty in myocardial infarction: three-year follow-up with cost benefit analysis of the Compare-Acute trial. EuroIntervention. 2020; 16:225–232. PMID: 32250250.
Article17. Calviño-Santos R, Estévez-Loureiro R, Peteiro-Vázquez J, et al. Angiographically guided complete revascularization versus selective stress echocardiography-guided revascularization in patients with ST-segment-elevation myocardial infarction and multivessel disease: the CROSS-AMI randomized clinical trial. Circ Cardiovasc Interv. 2019; 12:e007924. PMID: 31554422.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Status of Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Coronary Artery Disease
- Clinical Significance of Predischarge Treadmill Exercise Test in Patients with Acute Myocardial Infarction
- Immediate multivessel revascularization may increase cardiac death and myocardial infarction in patients with ST-elevation myocardial infarction and multivessel coronary artery disease: data analysis from real world practice
- Revascularization for Left Main and Multivessel Coronary Artery Disease: Current Status and Future Prospects after the EXCEL and NOBLE Trials
- Staged Complete Revascularization in ST-Segment Elevation Myocardial Infarction Should Be the Treatment of Choice Compared to Primary Complete Revascularization
