Acute Crit Care.
2022 Feb;37(1):84-93. 10.4266/acc.2021.00129.
Clinical characteristics and outcomes of critically ill COVID-19 patients in Sfax, Tunisia
- Bahloul M
 1
1 - Kharrat S1
- Chtara K1
- Hafdhi M1
- Turki O1
- Baccouche N1
- Ammar R1
- Kallel N2
- Hsairi M3
- Chakroun-Walha O4
- Hamida CB1
- Chelly H1
- Mahfoudh KB2
- Karoui A3
- Karray H5
- Rekik N4
- Bouaziz M1
- Affiliations
-
- 1Department of Intensive Care, Habib Bourguiba University Hospital, Sfax University, Sfax, Tunisia
- 2Department of Radiology, Habib Bourguiba University Hospital, Sfax University, Sfax, Tunisia
- 3Department of Anesthesiology, Habib Bourguiba University Hospital, Sfax University, Sfax, Tunisia
- 4Department of Emergency Medicine, Habib Bourguiba University Hospital, Sfax University, Sfax, Tunisia
- 5Department of Microbiology, Habib Bourguiba University Hospital, Sfax University, Sfax, Tunisia
- KMID: 2527910
- DOI: http://doi.org/10.4266/acc.2021.00129
Abstract
- Background
Africa, like the rest of the world, has been impacted by the coronavirus disease 2019 (COVID-19) pandemic. However, only a few studies covering this subject in Africa have been published. Methods: We conducted a retrospective study of critically ill adult COVID-19 patients—all of whom had a confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection— admitted to the intensive care unit (ICU) of Habib Bourguiba University Hospital (Sfax, Tunisia). Results: A total of 96 patients were admitted into our ICU for respiratory distress due to COVID-19 infection. Mean age was 62.4±12.8 years and median age was 64 years. Mean arterial oxygen tension (PaO2)/fractional inspired oxygen (FiO2) ratio was 105±60 and ≤300 in all cases but one. Oxygen support was required for all patients (100%) and invasive mechanical ventilation for 38 (40%). Prone positioning was applied in 67 patients (70%). Within the study period, 47 of the 96 patients died (49%). Multivariate analysis showed that the factors associated with poor outcome were the development of acute renal failure (odds ratio [OR], 6.7; 95% confidence interval [CI], 1.75–25.9), the use of mechanical ventilation (OR, 5.8; 95% CI, 1.54–22.0), and serum cholinesterase (SChE) activity lower than 5,000 UI/L (OR, 5.0; 95% CI, 1.34–19). Conclusions: In this retrospective cohort study of critically ill patients admitted to the ICU in Sfax, Tunisia, for acute respiratory failure following COVID-19 infection, the mortality rate was high. The development of acute renal failure, the use of mechanical ventilation, and SChE activity lower than 5,000 UI/L were associated with a poor outcome.
Keyword
Figure
-
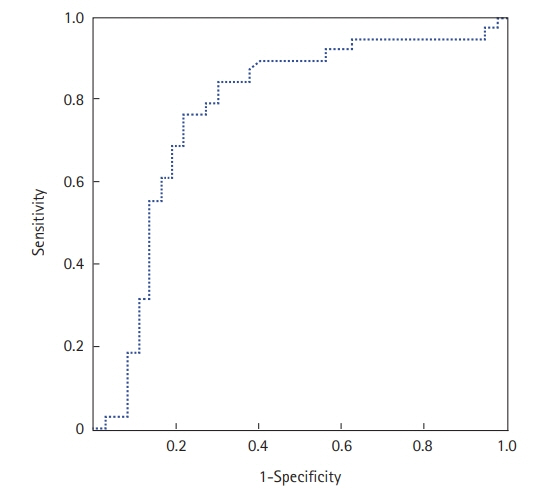
Figure 1. Receiver operating characteristic curve of serum cholinesterase (SChE) activity to predict mortality. The area under the curve was 0.77, indicating good ability of SChE to discriminate between survivors and non-survivors.
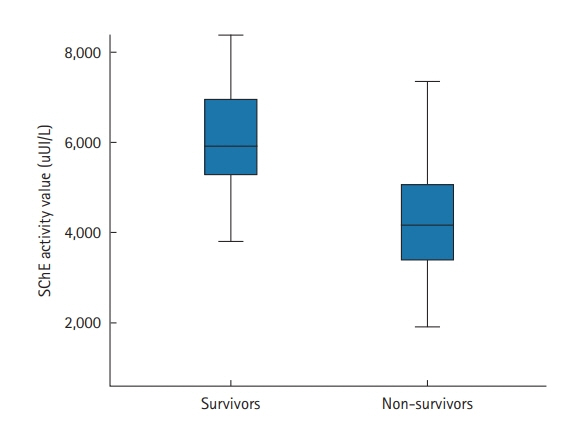
Figure 2. The lowest serum cholinesterase (SChE) activity value recorded according to outcomes. Black line, median; box, 25%–75%; error bar, range.
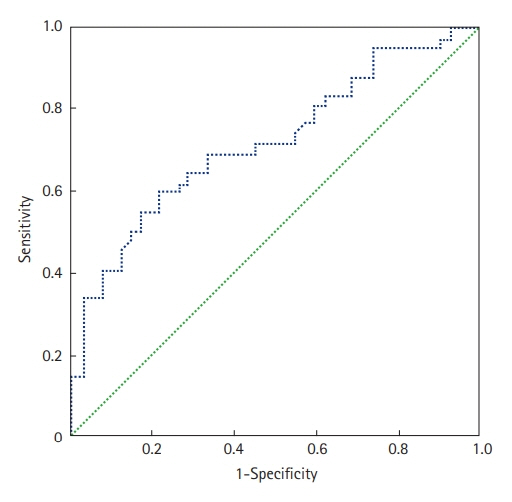
Figure 3. Receiver operating characteristic curve of C-reactive protein level to predict mortality. The area under the curve was 0.73.
Reference
-
1. Worldometer. Coronavirus update [Internet]. Worldometer;2020. [cited 2020 Jul 24]. Available from: https://www.worldometers.info/coronavirus/.2. Vetter P, Vu DL, L'Huillier AG, Schibler M, Kaiser L, Jacquerioz F. Clinical features of covid-19. BMJ. 2020; 369:m1470.
Article3. Chaddha U, Kaul V, Agrawal A. What is the true mortality in the critically ill patients with COVID-19? Indian J Crit Care Med. 2020; 24:383–4.
Article4. Olumade TJ, Uzairue LI. Clinical characteristics of 4499 COVID-19 patients in Africa: a meta-analysis. J Med Virol. 2021; 93:3055–61.
Article5. Abayomi A, Odukoya O, Osibogun A, Wright O, Adebayo B, Balogun M, et al. Presenting symptoms and predictors of poor outcomes among 2,184 patients with COVID-19 in Lagos State, Nigeria. Int J Infect Dis. 2021; 102:226–32.
Article6. El Vally A, Bollahi MA, Ould Ahmedou Salem MS, Deida J, Parola P, Basco L, et al. Retrospective overview of a COVID-19 outbreak in Mauritania. New Microbes New Infect. 2020; 38:100788.
Article7. Ibrahim OR, Suleiman BM, Abdullahi SB, Oloyede T, Sanda A, Gbadamosi MS, et al. Epidemiology of COVID-19 and predictors of outcome in Nigeria: a single-center study. Am J Trop Med Hyg. 2020; 103:2376–81.
Article8. Matangila JR, Nyembu RK, Telo GM, Ngoy CD, Sakobo TM, Massolo JM, et al. Clinical characteristics of COVID-19 patients hospitalized at Clinique Ngaliema, a public hospital in Kinshasa, in the Democratic Republic of Congo: a retrospective cohort study. PLoS One. 2020; 15:e0244272.
Article9. Bahloul M, Ketata W, Lahyeni D, Mayoufi H, Kotti A, Smaoui F, et al. Pulmonary capillary leak syndrome following COVID-19 virus infection. J Med Virol. 2021; 93:94–6.
Article10. Saida IB, Ennouri E, Nachi R, Meddeb K, Mahmoud J, Thabet N, et al. Very severe COVID-19 in the critically ill in Tunisia. Pan Afr Med J. 2020; 35(Suppl 2):136.
Article11. Hare SS, Rodrigues JCL, Nair A, Jacob J, Upile S, Johnstone A, et al. The continuing evolution of COVID-19 imaging pathways in the UK: a British Society of Thoracic Imaging expert reference group update. Clin Radiol. 2020; 75:399–404.
Article12. Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA. 1993; 270:2957–63.
Article13. Ferreira FL, Bota DP, Bross A, Mélot C, Vincent JL. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA. 2001; 286:1754–8.
Article14. World Health Organization. Obesity [Internet]. Geneva: World Health Organization;2020. [cited 2020 Jul 24]. Available from: https://www.who.int/topics/obesity/en/.15. Papazian L, Aubron C, Brochard L, Chiche JD, Combes A, Dreyfuss D, et al. Formal guidelines: management of acute respiratory distress syndrome. Ann Intensive Care. 2019; 9:69.
Article16. RECOVERY Collaborative Group, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, et al. Dexamethasone in hospitalized patients with COVID-19. N Engl J Med. 2021; 384:693–704.
Article17. Makkar P, Pastores SM. Respiratory management of adult patients with acute respiratory distress syndrome due to COVID-19. Respirology. 2020; 25:1133–5.
Article18. Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983; 148:839–43.
Article19. Lo Bianco G, Di Pietro S, Mazzuca E, et al. Multidisciplinary approach to the diagnosis and in-hospital management of COVID-19 infection: a narrative review. Front Pharmacol. 2020; 11:572168.
Article20. Agarwal N, Biswas B, Lohani P. Epidemiological determinants of COVID-19 infection and mortality: a study among patients presenting with severe acute respiratory illness during the pandemic in Bihar, India. Niger Postgrad Med J. 2020; 27:293–301.
Article21. Brown WA, Moore EM, Watters DA. Mortality of patients with COVID-19 who undergo an elective or emergency surgical procedure: a systematic review and meta-analysis. ANZ J Surg. 2021; 91:33–41.
Article22. Grasselli G, Greco M, Zanella A, Albano G, Antonelli M, Bellani G, et al. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern Med. 2020; 180:1345–55.23. Verma AA, Hora T, Jung HY, Fralick M, Malecki SL, Lapointe-Shaw L, et al. Characteristics and outcomes of hospital admissions for COVID-19 and influenza in the Toronto area. CMAJ. 2021; 193:E410–8.
Article24. Roedl K, Jarczak D, Thasler L, Bachmann M, Schulte F, Bein B, et al. Mechanical ventilation and mortality among 223 critically ill patients with coronavirus disease 2019: a multicentric study in Germany. Aust Crit Care. 2021; 34:167–75.
Article25. Name JJ, Souza AC, Vasconcelos AR, Prado PS, Pereira CP. Zinc, vitamin D and vitamin C: perspectives for COVID-19 with a focus on physical tissue barrier integrity. Front Nutr. 2020; 7:606398.
Article26. Kim MS, An MH, Kim WJ, Hwang TH. Comparative efficacy and safety of pharmacological interventions for the treatment of COVID-19: a systematic review and network meta-analysis. PLoS Med. 2020; 17:e1003501.
Article27. Zang X, Wang Q, Zhou H, Liu S, Xue X; COVID-19 Early Prone Position Study Group. Efficacy of early prone position for COVID-19 patients with severe hypoxia: a single-center prospective cohort study. Intensive Care Med. 2020; 46:1927–9.
Article28. Kang SH, Kim SW, Kim AY, Cho KH, Park JW, Do JY. Association between chronic kidney disease or acute kidney injury and clinical outcomes in COVID-19 patients. J Korean Med Sci. 2020; 35:e434.
Article29. Fabrizi F, Alfieri CM, Cerutti R, Lunghi G, Messa P. COVID-19 and acute kidney injury: a systematic review and meta-analysis. Pathogens. 2020; 9:1052.
Article30. Kolhe NV, Fluck RJ, Selby NM, Taal MW. Acute kidney injury associated with COVID-19: a retrospective cohort study. PLoS Med. 2020; 17:e1003406.
Article31. Nakajima K, Abe T, Saji R, Ogawa F, Taniguchi H, Yamaguchi K, et al. Serum cholinesterase associated with COVID-19 pneumonia severity and mortality. J Infect. 2021; 82:282–327.
Article32. Bahloul M, Baccouch N, Chtara K, Turki M, Turki O, Hamida CB, et al. Value of serum cholinesterase activity in the diagnosis of septic shock due to bacterial infections. J Intensive Care Med. 2017; 32:346–52.
Article33. Bardi T, Pintado V, Gomez-Rojo M, Escudero-Sanchez R, Azzam Lopez A, Diez-Remesal Y, et al. Nosocomial infections associated to COVID-19 in the intensive care unit: clinical characteristics and outcome. Eur J Clin Microbiol Infect Dis. 2021; 40:495–502.
Article34. Musuuza JS, Watson L, Parmasad V, Putman-Buehler N, Christensen L, Safdar N. Prevalence and outcomes of co-infection and superinfection with SARS-CoV-2 and other pathogens: a systematic review and meta-analysis. PLoS One. 2021; 16:e0251170.
Article35. Bassetti M, Kollef MH, Timsit JF. Bacterial and fungal superinfections in critically ill patients with COVID-19. Intensive Care Med. 2020; 46:2071–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Impact of prone position on outcomes of COVID-19 patients with spontaneous breathing
- Gravity-induced ischemia in the brain and prone positioning for COVID-19 patients breathing spontaneously: still far from the truth!
- Characteristics of Critically Ill COVID-19 Patients in Busan, Republic of Korea
- Experience of Treating Critically Ill COVID-19 Patients in Daegu, South Korea
- How We Have Treated Severe to Critically Ill Patients With Coronavirus Disease 2019 in Korea
