Steroid injection using tendon excursion for trigger finger: introduction to injection methods and analysis of treatment results
- Affiliations
-
- 1Department of Orthopedic Surgery, Inha University Hospital, Incheon, Korea
- KMID: 2526646
- DOI: http://doi.org/10.12790/ahm.21.0134
Abstract
- Purpose
Local corticosteroid injections are routinely used as first-line treatment for trigger finger. However, accurate delivery of steroids into the tendon sheath is important for the effectiveness of the treatment and the prevention of complications. This study aimed to introduce our steroid injection technique for trigger finger, which uses tendon excursion of the flexor tendon, and evaluate the clinical outcomes in patients who were treated with this technique.
Methods
A total of 171 patients with trigger finger who were treated with steroid injections were retrospectively reviewed. The efficacy of injection and complications were investigated. The evaluation of the efficacy was classified into “good,” “fair,” and “poor.” The results were analyzed according to the type of finger and the Quinnell grading system.
Results
The total efficacy was 83.6% (good/fair, 143 digits; poor, 28 digits). The treatment success rate for Quinnell grade IV was 43.8% (7 of 16), which was significantly lower than those of Quinnell grades II and III, which were 88.9% (88 of 99) and 87.5% (49 of 56), respectively (II vs. IV, p=0.004; III vs. IV, p=0.010). In four fingers (excluding the thumb), the success rate was significantly higher than that of the thumb (88.2% vs. 75.4%, p=0.048).
Conclusion
The steroid injection technique using tendon excursion showed excellent results and low complication rates. In particular, the second to fourth fingers and low-grade fingers showed more effective results.
Figure
-

Fig. 1. Photograph demonstrating the injection technique using tendon excursion in trigger finger. (A) Palpitate the metacarpal neck. (B) With the affected finger in a flexed position, insert a 26-gauge needle aiming at 45°. (C) Ask the patient to flex and extend the finger to ascertain that the needle tip is not in the tendon. (D) Inject and feel the fluid thrill.
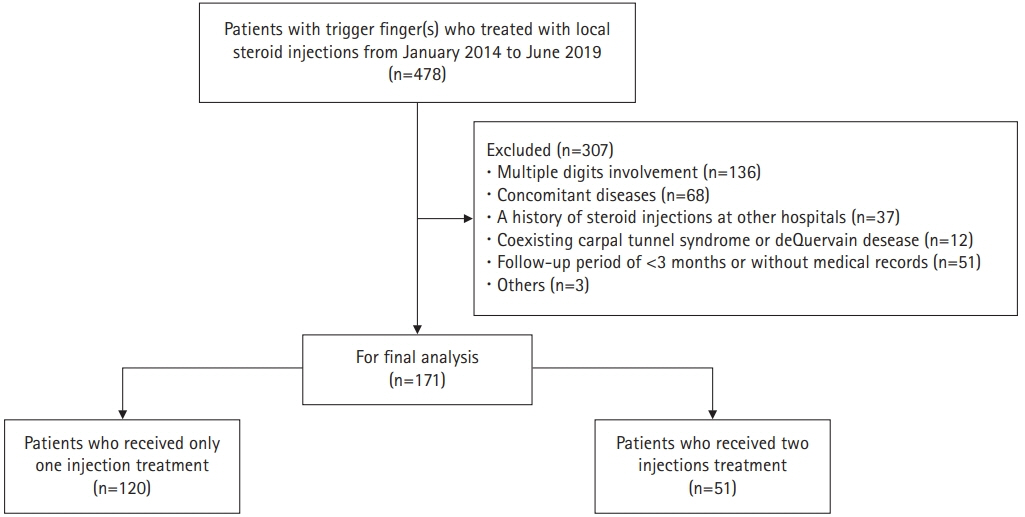
Fig. 2. Flowchart of patient selection for this study.
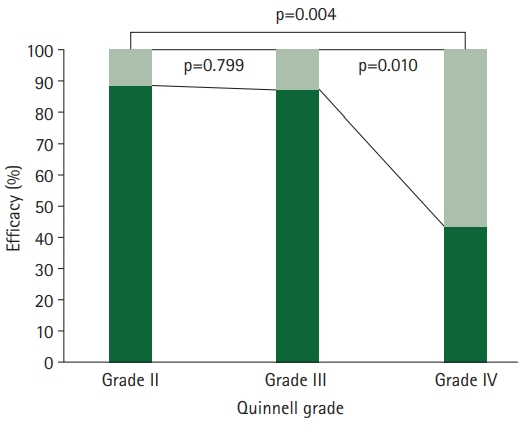
Fig. 3. Comparison of the efficacy of steroid injections by Quinnell grading.

Fig. 4. A 56-year-old female patient with right trigger thumb developed complications after the second steroid injection. The photograph shows skin depigmentation and fat atrophy of the right thumb.

Fig. 5. Diagram showing the needle tip position during tendon excursion. (A) Insertion of the needle tip up to the tendon in the bevel-up state. (B) Rotation of the needle tip 180° to bevel down. (C) View of the needle entering into the flexor sheath after tendon excursion but not passing through the tendon substance.

Fig. 6. Cross-sectional view showing three possible positions of the needle tip in the A1 pulley. (A) Intratendinous injection, (B) intrasheath injection, and (C) extrasheath injection.
Reference
-
References
1. Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am. 2006; 31:135–46.
Article2. Huisstede BM, Hoogvliet P, Coert JH, Fridén J; European HANDGUIDE Group. Multidisciplinary consensus guideline for managing trigger finger: results from the European HANDGUIDE Study. Phys Ther. 2014; 94:1421–33.
Article3. Lunsford D, Valdes K, Hengy S. Conservative management of trigger finger: a systematic review. J Hand Ther. 2019; 32:212–21.
Article4. Howard LD Jr, Pratt DR, Bunnell S. The use of compound F (hydrocortone) in operative and non-operative conditions of the hand. J Bone Joint Surg Am. 1953; 35-A:994–1002.
Article5. Anderson B, Kaye S. Treatment of flexor tenosynovitis of the hand (‘trigger finger’) with corticosteroids: a prospective study of the response to local injection. Arch Intern Med. 1991; 151:153–6.
Article6. Benson LS, Ptaszek AJ. Injection versus surgery in the treatment of trigger finger. J Hand Surg Am. 1997; 22:138–44.
Article7. Murphy D, Failla JM, Koniuch MP. Steroid versus placebo injection for trigger finger. J Hand Surg Am. 1995; 20:628–31.
Article8. Nichols AW. Complications associated with the use of corticosteroids in the treatment of athletic injuries. Clin J Sport Med. 2005; 15:370–5.
Article9. Akhtar S, Burke FD. Study to outline the efficacy and illustrate techniques for steroid injection for trigger finger and thumb. Postgrad Med J. 2006; 82:763–6.
Article10. Kamhin M, Engel J, Heim M. The fate of injected trigger fingers. Hand. 1983; 15:218–20.
Article11. Fowler JR, Ogrich L, Evangelista P, Schaffer AA. Assessing injection techniques in the treatment of trigger finger. Mod Plast Surg. 2012; 2:83–6.12. Amiri Aref H, Fatemeh S, Mohammad Hosein K. Comparison between corticosteroid injection and surgery in the treatment of trigger finger. J Transl Int Med. 2015; 2:132–5.
Article13. Notta A. Recherches sur une affection particuliere des gaines tendineuses de la main, caracterisee par le developement de une nodosite sur la trajet des tendons flechisseurs des doigts et par l'empechment de leurs mouvements. Arch Gen Med. 1850; 24:142–61.14. Freiberg A, Mulholland RS, Levine R. Nonoperative treatment of trigger fingers and thumbs. J Hand Surg Am. 1989; 14:553–8.
Article15. Franko OI, Winters TM, Tirrell TF, Hentzen ER, Lieber RL. Moment arms of the human digital flexors. J Biomech. 2011; 44:1987–90.
Article16. Balasubramaniam P, Prathap K. The effect of injection of hydrocortisone into rabbit calcaneal tendons. J Bone Joint Surg Br. 1972; 54:729–34.
Article17. Lin YC, Shieh SJ. Extensor-pollicis-longus or -brevis tendon rupture after corticosteroid injection. Formos J Surg. 2016; 49:15–9.
Article18. Fitzgerald BT, Hofmeister EP, Fan RA, Thompson MA. Delayed flexor digitorum superficialis and profundus ruptures in a trigger finger after a steroid injection: a case report. J Hand Surg Am. 2005; 30:479–82.
Article19. Shinomiya R, Sunagawa T, Nakashima Y, Yoshizuka M, Adachi N. Impact of corticosteroid injection site on the treatment success rate of trigger finger: a prospective study comparing ultrasound-guided true intra-sheath and true extra-sheath injections. Ultrasound Med Biol. 2016; 42:2203–8.
Article20. Mardani-Kivi M, Karimi-Mobarakeh M, Babaei Jandaghi A, Keyhani S, Saheb-Ekhtiari K, Hashemi-Motlagh K. Intra-sheath versus extra-sheath ultrasound guided corticosteroid injection for trigger finger: a triple blinded randomized clinical trial. Phys Sportsmed. 2018; 46:93–7.
Article21. Brinks A, Koes BW, Volkers AC, Verhaar JA, Bierma-Zeinstra SM. Adverse effects of extra-articular corticosteroid injections: a systematic review. BMC Musculoskelet Disord. 2010; 11:206.
Article22. Godey SK, Bhatti WA, Watson JS, Bayat A. A technique for accurate and safe injection of steroid in trigger digits using ultrasound guidance. Acta Orthop Belg. 2006; 72:633–4.23. Nikolaou VS, Malahias MA, Kaseta MK, Sourlas I, Babis GC. Comparative clinical study of ultrasound-guided A1 pulley release vs open surgical intervention in the treatment of trigger finger. World J Orthop. 2017; 8:163–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment and Rehabilitation for Ruptured Flexor Digitorum Profundus Tendon after Steroid Injection in Trigger Finger and Carpal Tunnel Syndrome
- The Efficacy of Steroid Injection in the Treatment of Trigger Finger
- Risk of the Repeated Local Steroid Injection: Rupture of the Extensor Mechanism at Zone V
- Morphological alterations of the tendon and pulley on ultrasound after intrasynovial injection of betamethasone for trigger digit
- Trigger Finger of a Distal A2 Pulley
