2021 Clinical Practice Guidelines for Diabetes: Pharmacotherapy and the Korean Diabetes Association Support System
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2526208
- DOI: http://doi.org/10.4093/jkd.2021.22.4.250
Abstract
- The most important change introduced in the pharmacotherapy session for the 2021 Clinical Practice Guidelines for Diabetes is the recommendation of two different strategies according to the patient’s condition. One approach is to optimize the blood glucose levels, while the other approach is to reduce adverse cardiovascular events or mortality, especially in patients with comorbidities (e.g., heart failure, atherosclerotic cardiovascular disease, or chronic kidney disease). We suggest four algorithms that take into account the patient’s condition (algorithms 1 to 4). The Korean Diabetes Association (KDA) developed a web-based clinical decision support system, known as the KDA support system (KDASS), which helps with the diagnosis of diabetes or gestational diabetes and whether to use glucose-lowering agents according to the patient’s condition.
Keyword
Figure
-
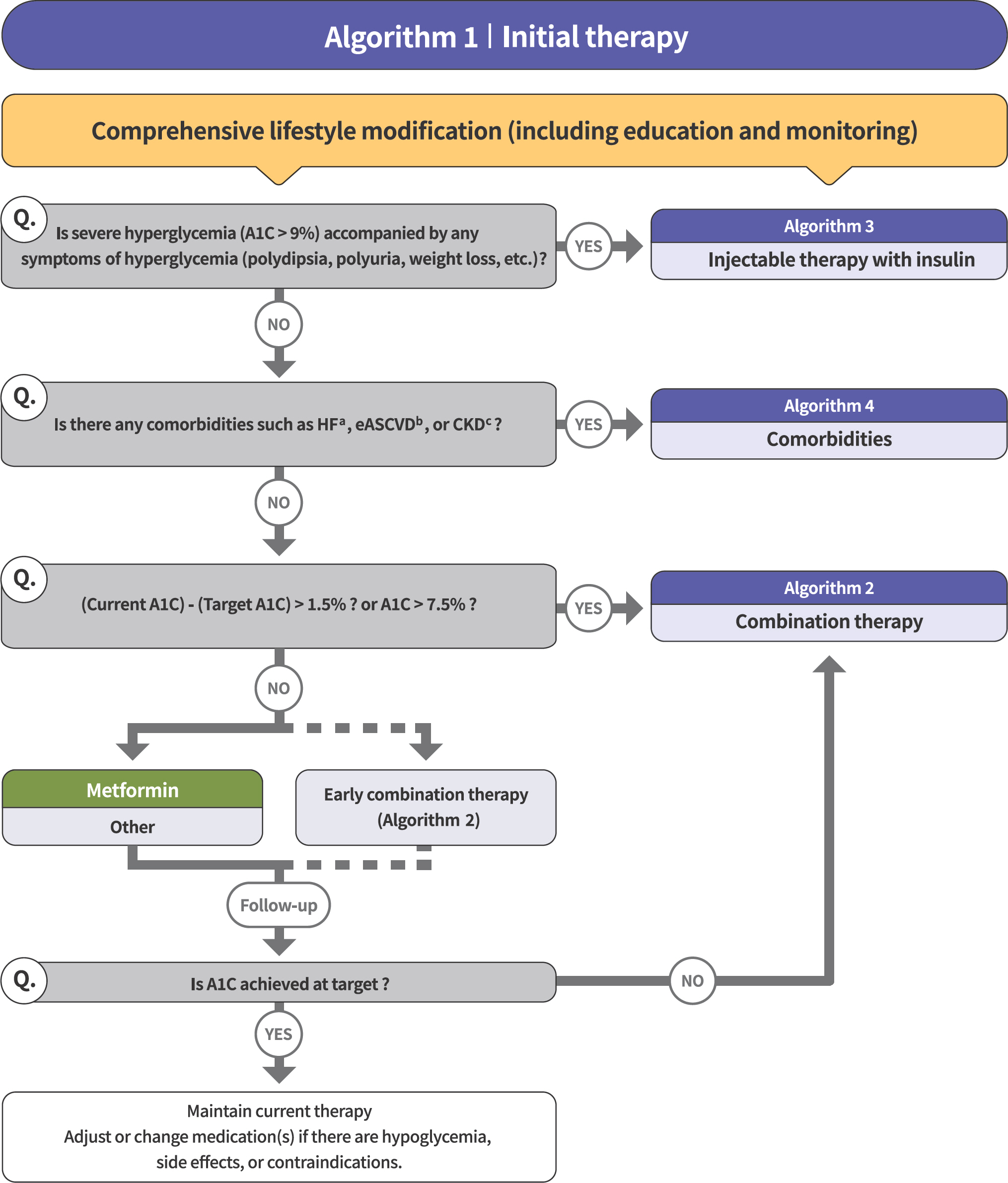
Fig. 1. Treatment algorithm 1 (initial therapy) for patients with type 2 diabetes mellitus (T2DM). The algorithm strat-ifies the strategy of glycemic control for T2DM based on initial glycosylated hemoglobin (A1C) levels and underlying comorbidities. For newly diagnosed T2DM, begin with comprehensive lifestyle modification (LSM) at the time of diagnosis and monitor continuously. If the initial severe hyperglycemia (A1C level > 9.0%) is accompanied by symptoms of hyperglycemia (polydipsia, polyuria, weight loss, etc.), insulin treatment should be prioritized (algorithm 3). If heart failure (HF), established atherosclerotic cardiovascular disease (eASCVD), or chronic kidney disease (CKD) are present, follow algorithm 4. If glycemic target is not achieved within 3 months after LSM, then glucose-lowering agent should be initiated promptly. If the current A1C is 1.5% higher than that of the target A1C or the current A1C level is > 7.5%, follow algorithm 2 (combination therapy). If the A1C level is 7.5% or less, metformin monotherapy is recommended as a first-line therapy. However, if there are contraindications or intolerable side effects related to metformin use, a different class of medications can be considered. Instead of metformin monotherapy, early combination therapy could be considered to reduce the risk of failure of glycemic control in some patients with newly diagnosed T2DM.
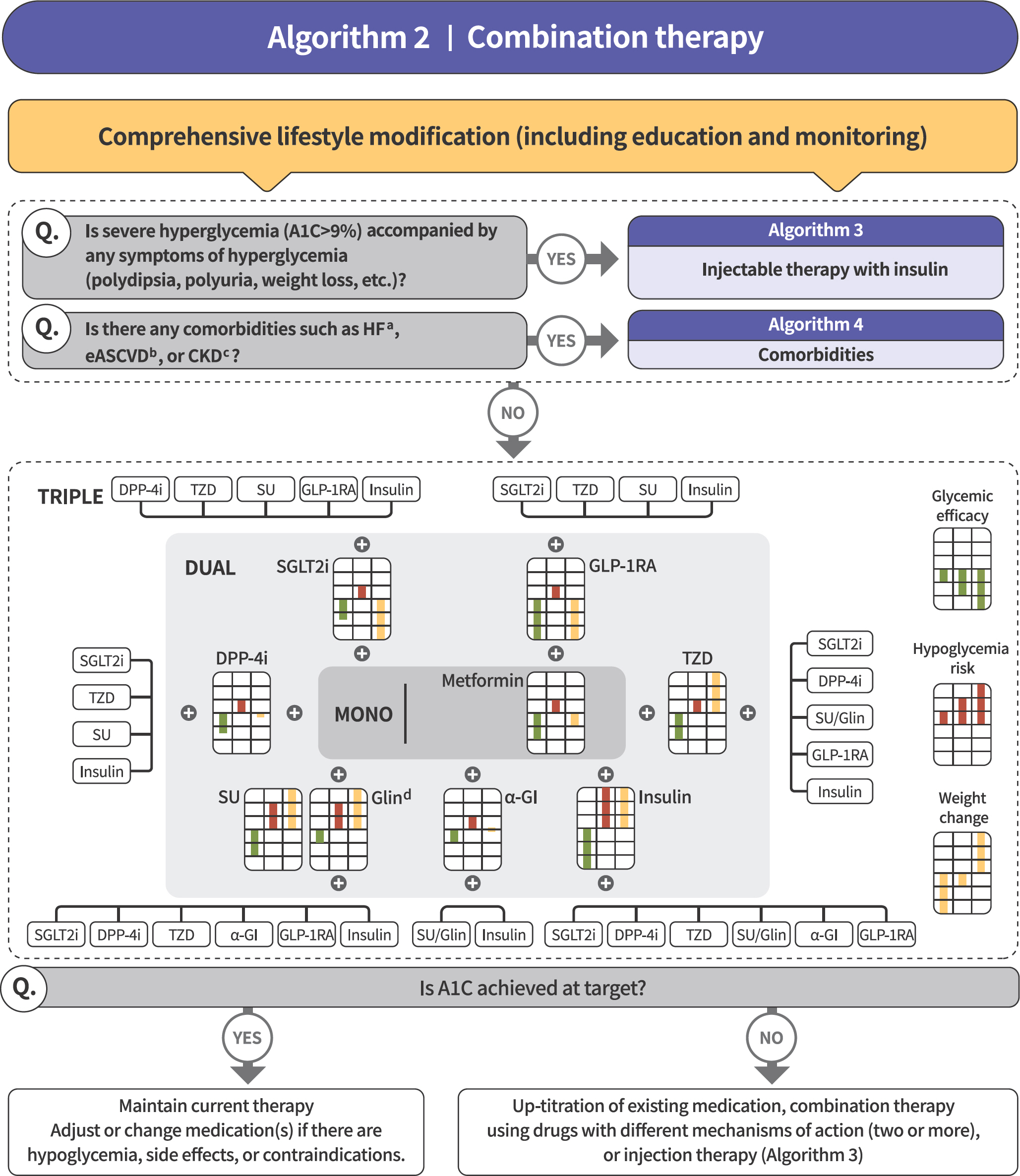
Fig. 2. Treatment algorithm 2 (combination therapy) for patients with type 2 diabetes mellitus (T2DM). If the current glycosylated hemoglobin (A1C) is 1.5% higher than that of the target A1C or the current A1C level is > 7.5%, combination therapy is recommended. If the target A1C level has not been achieved, the up-titration of existing medication, combination therapy using medications with different mechanisms of action, or use of injectable medication should actively be considered as soon as possible. When choosing glucose-lowering agents, consider glucose-lowering efficacy, hypoglycemia risk or weight change, side effects, treatment acceptability, age, personal value of life, and cost. The characteristics of glucose-lowering agents are expressed as a bar scale. Each color shows glycemic efficacy (green), hypoglycemia risk (red), and body weight change (yellow).
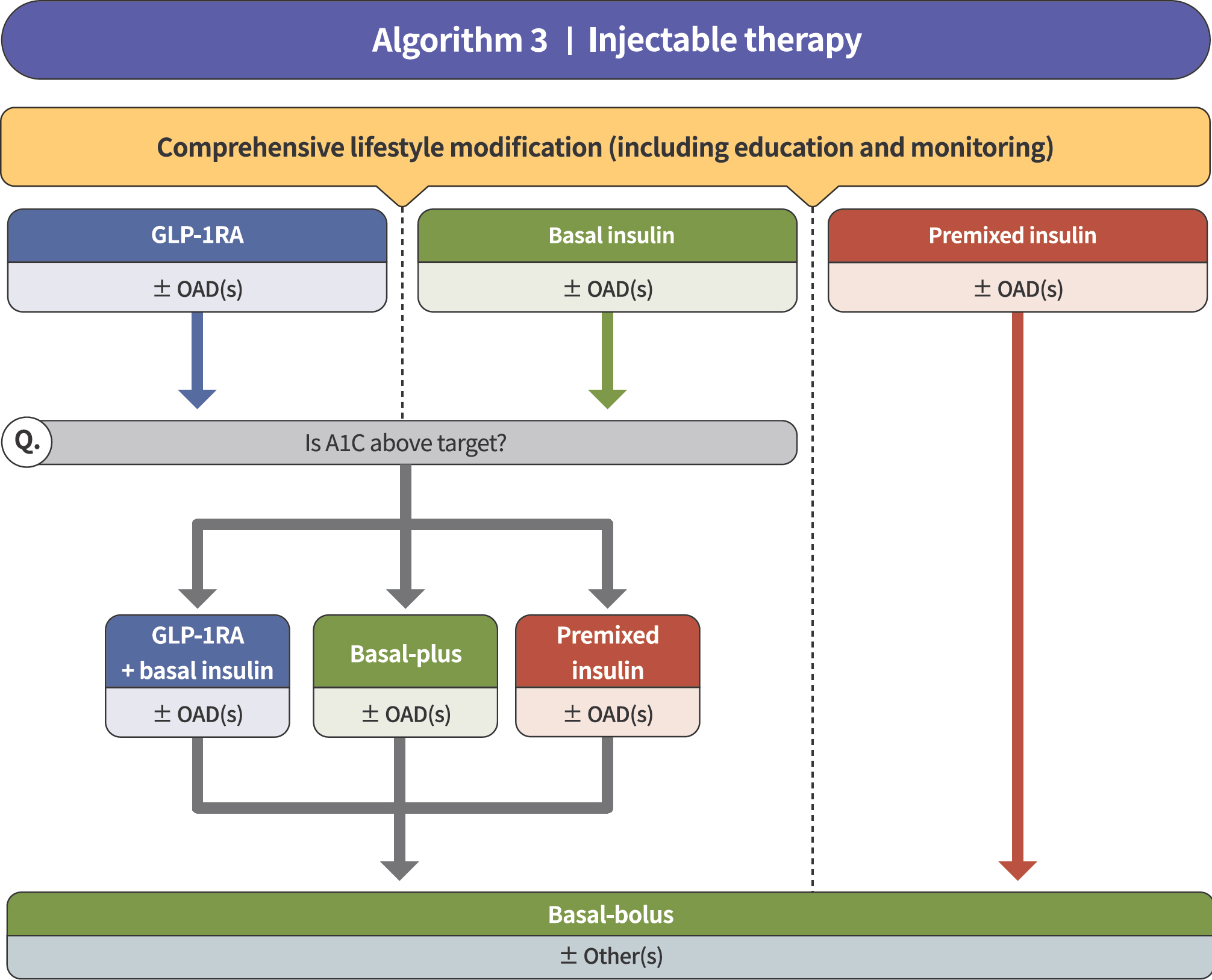
Fig. 3. Treatment algorithm 3 (injectable therapy) for patients with type 2 diabetes mellitus (T2DM). If the glycosylated hemoglobin (A1C) level is > 9.0% and symptomatic hyperglycemia or metabolic decompensation is present, insulin therapy can be initiated with or without oral anti-diabetic drug (OAD) in patients with T2DM. Injectable therapy (glucagon-like peptide-1 receptor agonist [GLP-1RA] or insulin) is recommended when potent glucose-lowering efficacy is required. The addition of GLP-1RA, basal insulin, or premixed insulin is recommended equally. If A1C target is not achieved with GLP-1RA or basal insulin-based therapy, free or fixed-ratio combination therapy of GLP-1RA and basal insulin could be considered. Intensification of insulin therapy with premixed insulin twice daily, basal-plus, or basal-bolus is also recommended to enhance blood glucose control.
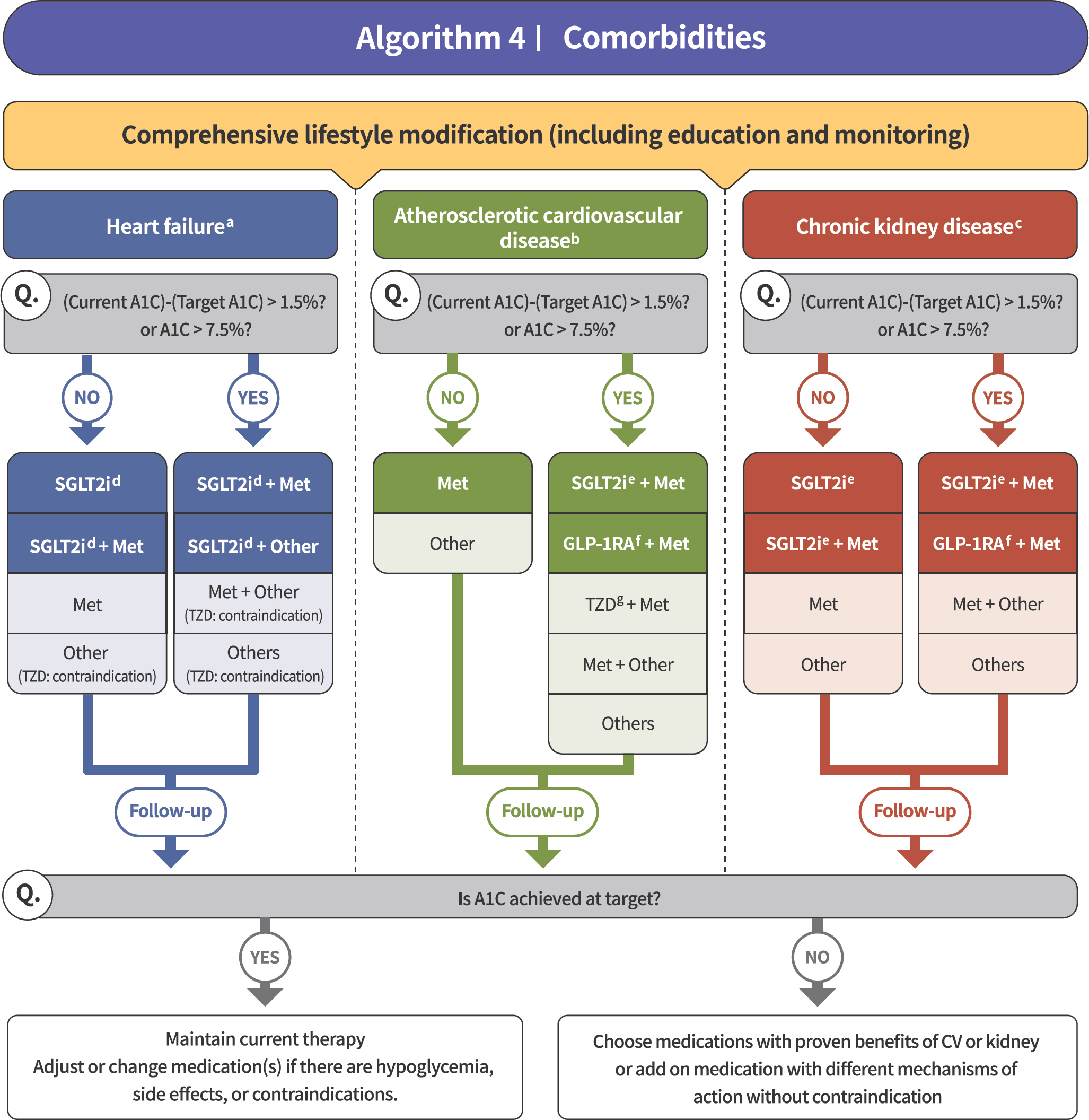
Fig. 4. Treatment algorithm 4 (comorbidities) for patients with type 2 diabetes mellitus who have heart failure (HF), established atherosclerotic cardiovascular disease (eASCVD), or chronic kidney disease (CKD). If patients have underlying above comorbidities, glucose-lowering agents, including sodium-glucose cotransporter 2 (SGLT2) inhibitor or gluca-gon-like peptide-1 receptor agonist (GLP1-RA), are the preferred choice. For patients with HF, glucose-lowering agents, including SGLT2 inhibitors with proven cardiovascular (CV) benefits, should be prioritized. Regimens that include SGLT2 inhibitors or GLP-1RAs with proven CV benefits should be prioritized for combination therapy in patients with eASCVD. For patients with albuminuria or reduced estimated glomerular filtration rate (eGFR), glucose-lowering agents, including SGLT2 inhibitors with proven renal and CV benefits, should be prioritized.
Reference
-
1.Hur KY., Moon MK., Park JS., Kim SK., Lee SH., Yun JS, et al. 2021 Clinical Practice Guidelines for Diabetes Mellitus of the Korean Diabetes Association. Diabetes Metab J. 2021. 45:461–81.
Article2.Stratton IM., Adler AI., Neil HA., Matthews DR., Manley SE., Cull CA, et al. Association of glycaemia with macro-vascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000. 321:405–12.
Article3.Kramer CK., Zinman B., Retnakaran R. Short-term intensive insulin therapy in type 2 diabetes mellitus: a system-atic review and meta-analysis. Lancet Diabetes Endocrinol. 2013. 1:28–34.
Article4.Tsapas A., Avgerinos I., Karagiannis T., Malandris K., Manol-opoulos A., Andreadis P, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a system-atic review and network meta-analysis. Ann Intern Med. 2020. 173:278–86.5.Moon MK. 2021 clinical practice guidelines for diabetes: management of cardiovascular risk. J Korean Diabetes. 2021. 22:259–67.
Article6.Kim NH. 2021 Korean Diabetes Association clinical practice guidelines for diabetes: diabetic kidney disease. J Korean Diabetes. 2021. 22:268–73.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 2021 Clinical Practice Guidelines for Diabetes Mellitus in Korea
- 2021 Korean Diabetes Association Clinical Practice Guidelines for Diabetes: Diabetic Kidney Disease
- 2023 Clinical Practice Guidelines for Diabetes
- 2023 Clinical Practice Guidelines for Diabetes: Recommendations for Pharmacological Treatment of Type 2 Diabetes
- 2021 Clinical Practice Guidelines for Diabetes: Management of Cardiovascular Risk
