Symptomatic Change of an Intracranial Neuroepithelial Cyst 7 Years After Its Incidental Finding
- Affiliations
-
- 1Departments of Neurosurgery, Tokyo Metropolitan Neurological Hospital, Tokyo, Japan
- 2Department of Neurosurgery, The University of Tokyo Hospital, Tokyo, Japan
- 3Departments of Pathology, Tokyo Metropolitan Neurological Hospital, Tokyo, Japan
- KMID: 2525300
- DOI: http://doi.org/10.14791/btrt.2022.10.e14
Abstract
- A natural course of asymptomatic neuroepithelial cysts (NECs) is poorly understood due to its rarity.Herein we report a 23-year-old female patient of an asymptomatic NEC which grew in size from 1 cm to 5 cm and caused progressive symptoms seven years after its incidental finding. Partial resection of the cyst was performed for decompression and pathological examination and effectively achieved symptoms alleviation and regression of the cyst. Our case showed the importance of regular follow-up because NECs may show symptomatic change even in the late phase.
Figure
-
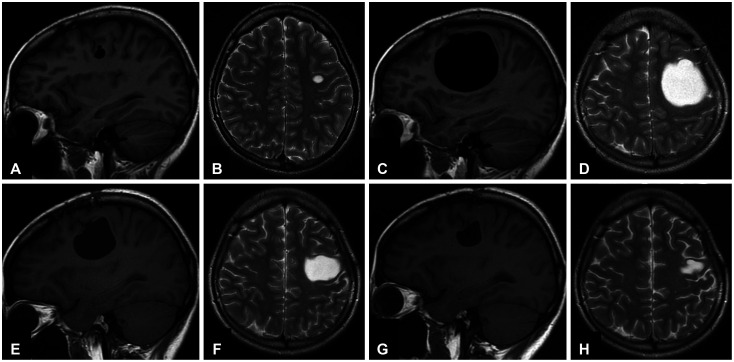
Fig. 1 Preoperative and postoperative MRI showing the growth and regression of a cyst. A and B: A sagittal (A) and axial (B) slice of a T1-weighted and T2-weighted image at the age of 16 years showing a small intra-axial cystic lesion with a septum in the frontal lobe. C and D: Preoperative sagittal (C) and axial (D) slice of a T1-weighted and T2-weighted image demonstrating an enlarged cystic lesion compressing the surrounding brain tissue. E-H: Postoperative T1-weighted sagittal image and T2-weighted axial image at 3 months (E and F) and 18 months (G and H) after surgery showing gradual regression of the cyst.
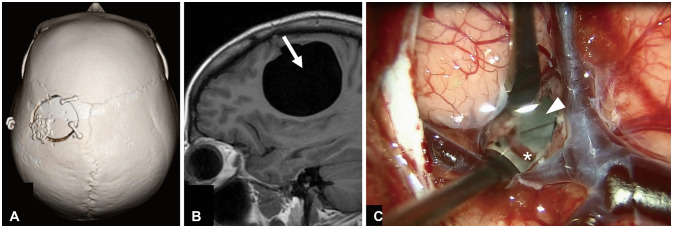
Fig. 2 Operative information and intraoperative findings. A: Three-dimensional reconstructed CT image presenting the craniotomy site. B: An arrow on a sagittal slice of MRI explains the direction of the surgical pathway. C: Intraoperative view under a microscope after a corticotomy showing the septum (arrowhead) and its feeding vessel (asterisk).
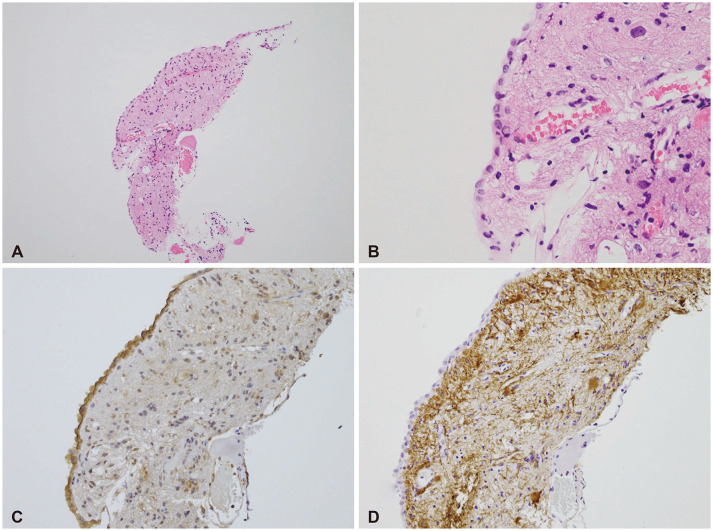
Fig. 3 Operative information and intraoperative findings. A and B: Low power view (A) and high power view (B) of surgical specimen with Hematoxylin-Eosin staining demonstrating a line of cuboidal cells, connective tissue, and vessels. C: Positive immunostaining for epithelial membrane antigen of the epithelial lining. D: Negative immunostaining for glial fibrillary acidic protein indicating the absence of a glial layer.
Reference
-
1. Robles LA, Paez JM, Ayala D, Boleaga-Duran B. Intracranial glioependymal (neuroglial) cysts: a systematic review. Acta Neurochir (Wien). 2018; 160:1439–1449. PMID: 29802560.
Article2. Morigaki R, Shinno K, Pooh KH, Nakagawa Y. Giant glioependymal cyst in an infant. J Neurosurg Pediatr. 2011; 7:175–178. PMID: 21284464.
Article3. Azzam NI, Timperley WR. Intracerebral cyst due to ectopic choroid plexus: case report. J Neurosurg. 1981; 55:651–653. PMID: 7277015.4. Asamoto S, Fukui Y, Nishiyama M, Ishikawa M, Fujita N, Nakamura S, et al. Diagnosis and surgical strategy for sacral meningeal cysts with check-valve mechanism: technical note. Acta Neurochir (Wien). 2013; 155:309–313. PMID: 23160631.
Article
