Endoscopic Ultrasound-Guided Gastroenterostomy for Afferent Loop Syndrome
- Affiliations
-
- 1Division of Gastroenterology and Hepatobiliary and Pancreatic Diseases, Department of Internal Medicine, Hyogo College of Medicine, Hyogo, Japan
- 2Division of Gastroenterology, Department of Internal Medicine, Kobe University Graduate School of Medicine, Kobe, Japan
- KMID: 2522700
- DOI: http://doi.org/10.5946/ce.2021.234
Abstract
- Afferent loop syndrome (ALS) is a mechanical obstruction of the afferent limbs after gastrectomy with gastrojejunostomy reconstruction. Patients with cancer recurrence require immediate and less invasive treatment because of their poor condition. Percutaneous transhepatic/transluminal drainage (PTD) and endoscopic enteral stenting offer reasonable palliative treatment for malignant ALS but are not fully satisfactory in terms of patient quality of life (QoL) and stent patency. Endoscopic ultrasound-guided gastroenterostomy (EUS-GE) using a lumen-apposing metal stent may address these shortcomings. Clinical data from 11 reports showed that all patients who had undergone EUS-GE had positive technical and clinical outcomes. The adverse event rate was 11.4%, including only mild or moderate abdominal pain, with no severe adverse events. Indirect comparative studies indicated that patients who had undergone EUS-GE had a significantly superior QoL, a higher clinical success rate, and a lower reintervention rate than those who had undergone PTD or endoscopic enteral stenting. Although the evidence is limited, EUS-GE may be considered as a first-line treatment for malignant ALS because it has better clinical outcomes than other less invasive treatments, such as PTD or endoscopic enteral stenting. Further prospective randomized control trials are necessary to establish EUS-GE as a standard treatment for ALS.
Keyword
Figure
-
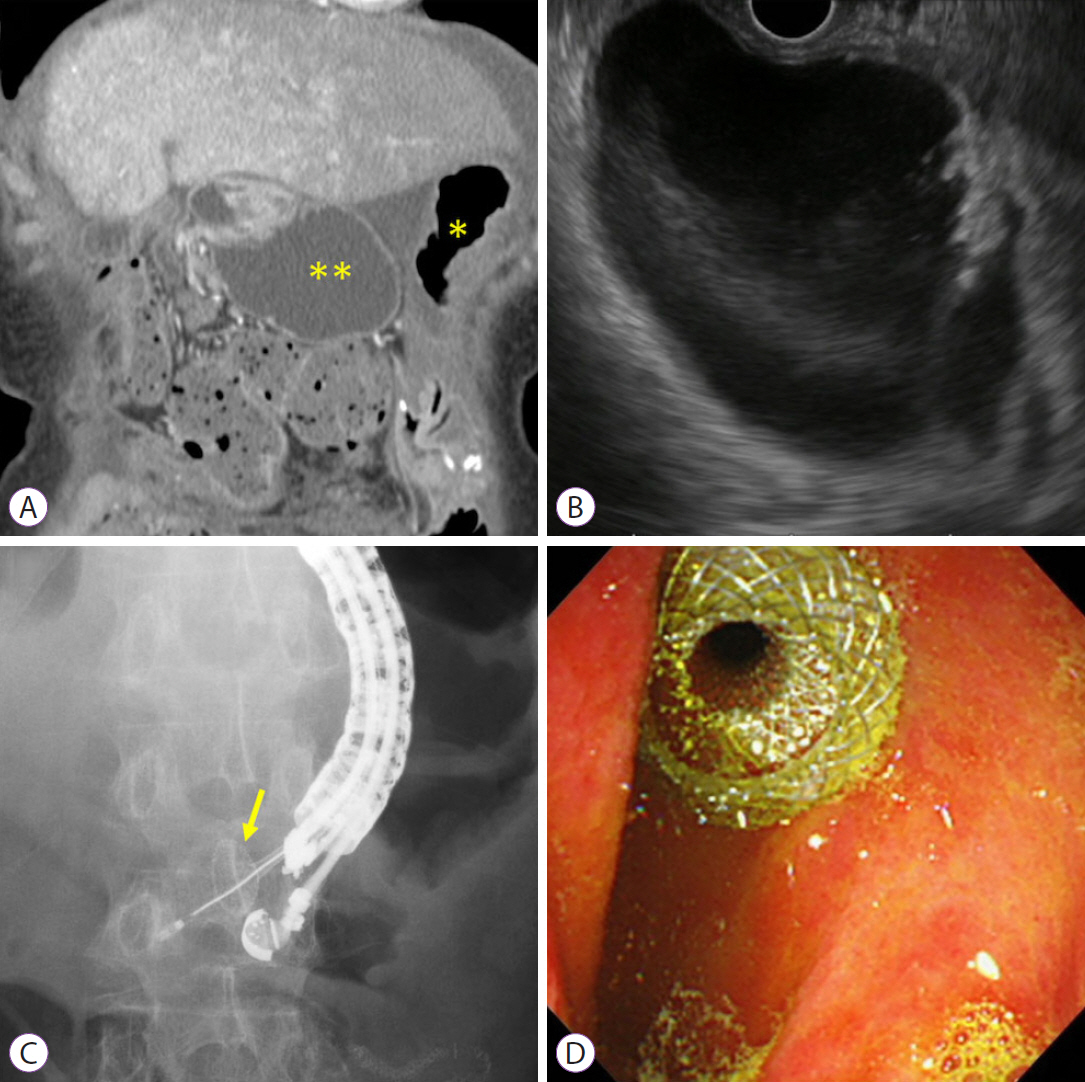
Fig. 1. Endoscopic ultrasound-guided gastroenterostomy using an EC-LAMS. (A) Contrast-enhanced computed tomography reveals that the dilated afferent limbs are associated with a recurrence of pancreatic cancer (*, stomach; **, dilated afferent limbs). (B) EUS shows dilatation of the afferent limbs from the stomach. (C) The dilated afferent limbs are punctured using an EC-LAMS, and the distal flange is then deployed under EUS guidance (yellow arrow: distal flange). (D) The proximal flange is deployed under endoscopic imaging. EC-LAMS, electrocautery-enhanced lumen-apposing metal stent; EUS, endoscopic ultrasound.
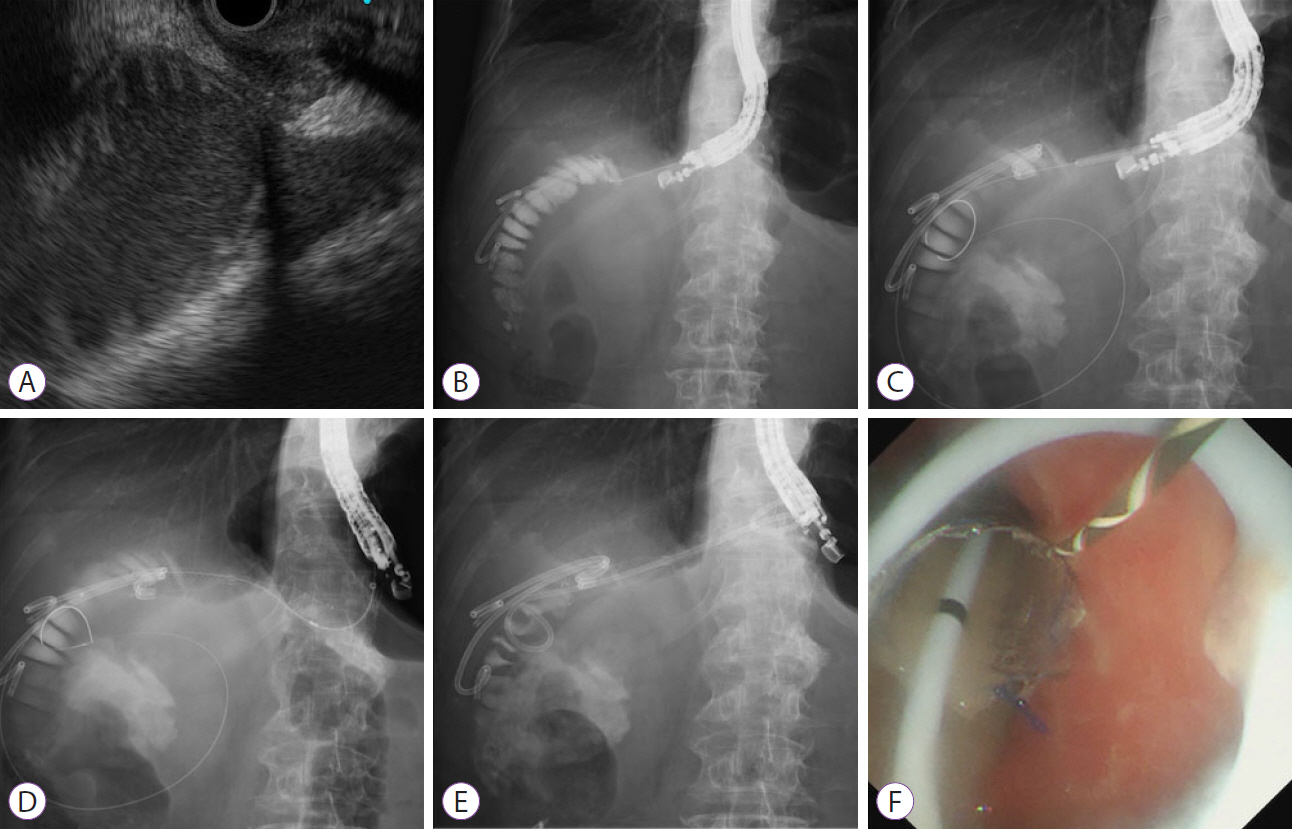
Fig. 2. Endoscopic ultrasound-guided gastroenterostomy using a fully covered self-expandable metal stent combined with a large loop double-pigtail stent. (A) On the endoscopic ultrasound image, the dilated afferent limbs can be visualized from the stomach. (B) The dilated afferent limbs are punctured using a 19-G needle, and a contrast medium is injected. (C) A guidewire is inserted to the afferent limbs, and the fistula is dilated using a balloon catheter. (D) A fully covered self-expandable metal stent is deployed to appose the afferent limbs and stomach. (E, F) A large loop double-pigtail plastic stent is placed through the fully covered self-expandable metal stent.
Reference
-
1. Pannala R, Brandabur JJ, Gan SI, et al. Afferent limb syndrome and delayed GI problems after pancreaticoduodenectomy for pancreatic cancer: single-center, 14-year experience. Gastrointest Endosc. 2011; 74:295–302.
Article2. Song KB, Yoo D, Hwang DW, et al. Comparative analysis of afferent loop obstruction between laparoscopic and open approach in pancreaticoduodenectomy. J Hepatobiliary Pancreat Sci. 2019; 26:459–466.
Article3. Blouhos K, Boulas KA, Tsalis K, Hatzigeorgiadis A. Management of afferent loop obstruction: reoperation or endoscopic and percutaneous interventions? World J Gastrointest Surg. 2015; 7:190–195.
Article4. Yane K, Katanuma A, Hayashi T, et al. Enteral self-expandable metal stent placement for malignant afferent limb syndrome using single-balloon enteroscope: report of five cases. Endosc Int Open. 2018; 6:E1330–E1335.
Article5. Sasaki T, Yamada I, Matsuyama M, Sasahira N. Enteral stent placement for malignant afferent loop obstruction by the through-the-scope technique using a short-type single-balloon enteroscope. Endosc Int Open. 2018; 6:E806–E811.
Article6. Shimatani M, Takaoka M, Tokuhara M, et al. Through-the-scope self-expanding metal stent placement using newly developed short double-balloon endoscope for the effective management of malignant afferent-loop obstruction. Endoscopy. 2016; 48(Suppl 1 UCTN):E6–E67.
Article7. Minaga K, Kitano M, Takenaka M. Through-the-scope enteral metal stent placement using a short-type single-balloon enteroscope for malignant surgically reconstructed jejunal stenosis (with video). Dig Endosc. 2016; 28:758.
Article8. Kanno Y, Ohira T, Harada Y, et al. Metal stent placement in the afferent loop obstructed by peritoneal metastases-experience of five cases. Clin Endosc. 2018; 51:299–303.
Article9. Brewer Gutierrez OI, Irani SS, Ngamruengphong S, et al. Endoscopic ultrasound-guided entero-enterostomy for the treatment of afferent loop syndrome: a multicenter experience. Endoscopy. 2018; 50:891–895.
Article10. Tonozuka R, Tsuchiya T, Mukai S, Nagakawa Y, Itoi T. Endoscopic ultrasonography-guided gastroenterostomy techniques for treatment of malignant gastric outlet obstruction. Clin Endosc. 2020; 53:510–518.
Article11. Sakai A, Shiomi H, Masuda A, Kobayashi T, Yamada Y, Kodama Y. Clinical management for malignant afferent loop obstruction. World J Gastrointest Oncol. 2021; 13:684–692.
Article12. Termsinsuk P, Chantarojanasiri T, Pausawasdi N. Diagnosis and treatment of the afferent loop syndrome. Clin J Gastroenterol. 2020; 13:660–668.
Article13. Grisé K, McFadden D. Anastomotic technique influences outcomes after partial gastrectomy for adenocarcinoma. Am Surg. 2001; 67:948–950.
Article14. Bolton JS, Conway WC. Postgastrectomy syndromes. Surg Clin North Am. 2011; 91:1105–1122.
Article15. Kim KH, Lee HB, Kim SH, Kim MC, Jung GJ. Role of percutaneous transhepatic biliary drainage in patients with complications after gastrectomy. Int Surg. 2015; May. 29. [Epub]. https://doi.org/10.9738/INTSURG-D-15-00117.1.
Article16. Sato Y, Inaba Y, Murata S, et al. Percutaneous drainage for afferent limb syndrome and pancreatic fistula via the blind end of the jejunal limb after pancreatoduodenectomy or bile duct resection. J Vasc Interv Radiol. 2015; 26:566–572.
Article17. Moriura S, Ikeda S, Kimura A, Iwatsuka Y, Ikezawa T, Naiki K. Jaundice due to afferent loop obstruction following hepatectomy for a hilar cholangiocarcinoma. Abdom Imaging. 1996; 21:226–227.
Article18. Kim HJ, Park JY, Bang S, Park SW, Lee YC, Song SY. Self-expandable metal stents for recurrent malignant obstruction after gastric surgery. Hepatogastroenterology. 2009; 56:914–917.19. Sakai A, Shiomi H, Iemoto T, et al. Endoscopic self-expandable metal stent placement for malignant afferent loop obstruction after pancreaticoduodenectomy: a case series and review. Clin Endosc. 2020; 53:491–496.
Article20. Matsumoto K, Kato H, Tomoda T, et al. A case of acute afferent loop syndrome treated by transgastric drainage with EUS. Gastrointest Endosc. 2013; 77:132–133.
Article21. Wannhoff A, Ruh N, Meier B, Riecken B, Caca K. Endoscopic gastrointestinal anastomoses with lumen-apposing metal stents: predictors of technical success. Surg Endosc. 2021; 35:1997–2004.
Article22. Itoi T, Baron TH, Khashab MA, et al. Technical review of endoscopic ultrasonography-guided gastroenterostomy in 2017. Dig Endosc. 2017; 29:495–502.
Article23. Yamamoto K, Tsuchiya T, Tanaka R, et al. Afferent loop syndrome treated by endoscopic ultrasound-guided gastrojejunostomy, using a lumen-apposing metal stent with an electrocautery-enhanced delivery system. Endoscopy. 2017; 49:E270–E272.
Article24. Ikeuchi N, Itoi T, Tsuchiya T, Nagakawa Y, Tsuchida A. One-step EUS-guided gastrojejunostomy with use of lumen-apposing metal stent for afferent loop syndrome treatment. Gastrointest Endosc. 2015; 82:166.
Article25. Shiomi H, Kobayashi T, Sakai A, et al. Endoscopic ultrasound-guided gastrojejunostomy using fully covered metal stent combined with large-loop double-pigtail stent for malignant afferent loop syndrome. Endoscopy. 2019; 51:E303–E304.
Article26. Taunk P, Cosgrove N, Loren DE, Kowalski T, Siddiqui AA. Endoscopic ultrasound-guided gastroenterostomy using a lumen-apposing self-expanding metal stent for decompression of afferent loop obstruction. Endoscopy. 2015; 47(Suppl 1 UCTN):E395–E396.
Article27. Shah A, Khanna L, Sethi A. Treatment of afferent limb syndrome: novel approach with endoscopic ultrasound-guided creation of a gastrojejunostomy fistula and placement of lumen-apposing stent. Endoscopy. 2015; 47(Suppl 1 UCTN):E309–E310.
Article28. De Bie C, Bronswijk M, Vanella G, et al. EUS-guided hepaticogastrostomy for patients with afferent loop syndrome: a comparison with EUS-guided gastroenterostomy or percutaneous drainage. Surg Endosc. 2021; Apr. 28. [Epub]. https://doi.org/10.1007/s00464-021-08520-z.
Article29. Benallal DC, Hoibian S, Caillol F, et al. EUS-guided gastroenterostomy for afferent loop syndrome treatment stent. Endosc Ultrasound. 2018; 7:418–419.
Article30. Sakamoto Y, Hijioka S, Maruki Y, et al. Endoscopic ultrasound-guided gastroenterostomy using a metal stent for the treatment of afferent loop syndrome. Endoscopy. 2019; 51:E153–E155.
Article31. Lajin M, Catalano MF, Khan NM, Lajin I. Endoscopic ultrasound-guided gastrojejunostomy using a 2-cm lumen-apposing metal stent to treat benign afferent loop syndrome. Endoscopy. 2019; 51:695–696.
Article32. Skinner M, Popa D, Neumann H, Wilcox CM, Mönkemüller K. ERCP with the overtube-assisted enteroscopy technique: a systematic review. Endoscopy. 2014; 46:560–572.
Article33. Kedia P, Sharaiha RZ, Kumta NA, Kahaleh M. Internal EUS-directed transgastric ERCP (EDGE): game over. Gastroenterology. 2014; 147:566–568.
Article34. Bukhari M, Kowalski T, Nieto J, et al. An international, multicenter, comparative trial of EUS-guided gastrogastrostomy-assisted ERCP versus enteroscopy-assisted ERCP in patients with Roux-en-Y gastric bypass anatomy. Gastrointest Endosc. 2018; 88:486–494.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Afferent Loop Syndrome Treated by Endoscopic Drainage Procedure using Nasogastric Tube
- The Role of Endoscopic Management in Afferent Loop Syndrome
- Endoscopic Management of Afferent Loop Syndrome after a Pylorus Preserving Pancreatoduodenecotomy Presenting with Obstructive Jaundice and Ascending Cholangitis
- Acute Abdomen Caused by Complicated Afferent Loop Syndrome after Gastrectomy
- Afferent loop syndrome: role of sonography and CT
