Thoracomyoplasty and perioperative negative wound pressure therapy for bronchopleural fistula after trans-sternal bronchial closure
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
- 2Department of Critical Care Medicine, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
- 3Division of Pulmonology, Department of Internal Medicine, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
- KMID: 2519456
- DOI: http://doi.org/10.4266/acc.2021.00626
Figure
-
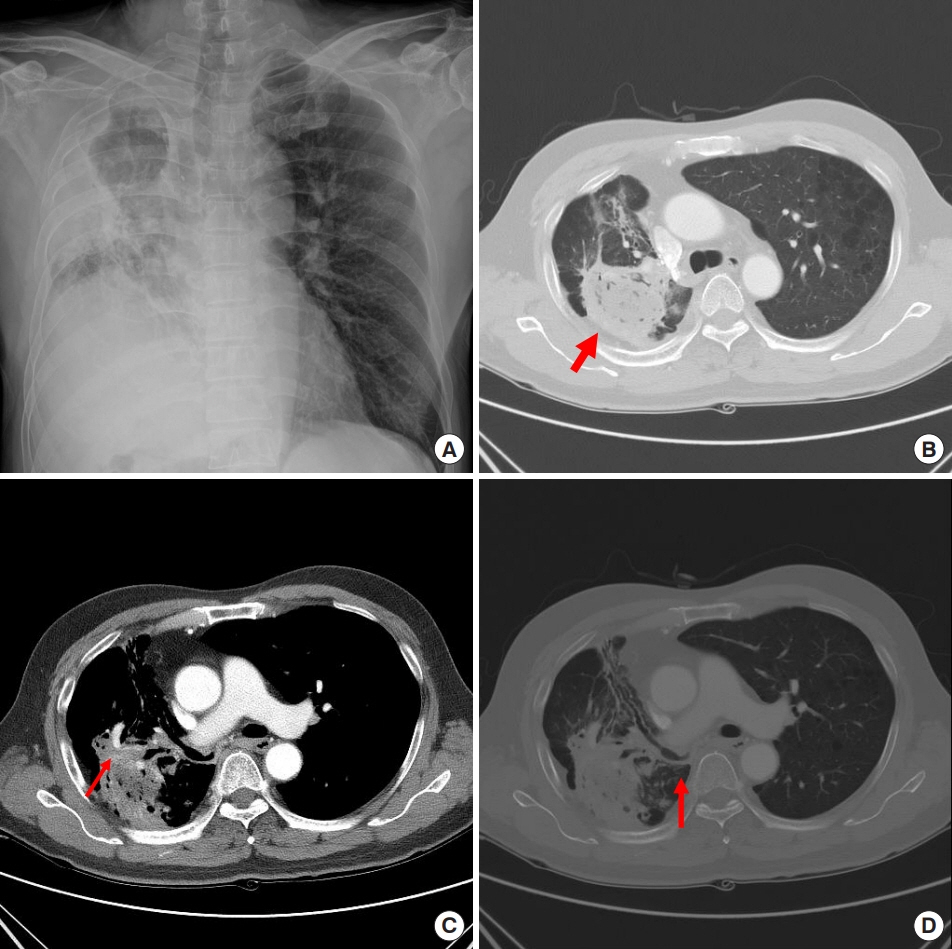
Figure 1. The chest images showed (A, B) the right-side fungal ball (red arrow) and (C) aneurysmal change of the bronchial artery (red arrow). (D) The right main pulmonary artery was divided with surgical material and only the right-side lower lobe bronchus was intact (red arrow).

Figure 2. Two months after the trans-sternal bronchial division operation, the patient complained of a massive amount of purulent sputum. (A, B) The chest images showed a long right-side bronchial stump (red arrow) and cavitary change of the right-side thoracic cavity. (C) The fungal ball (white arrow) was still inside. (D) Bronchoscopy showed surgical material at the right-side bronchial stump (white arrow) and opening (arrowhead).
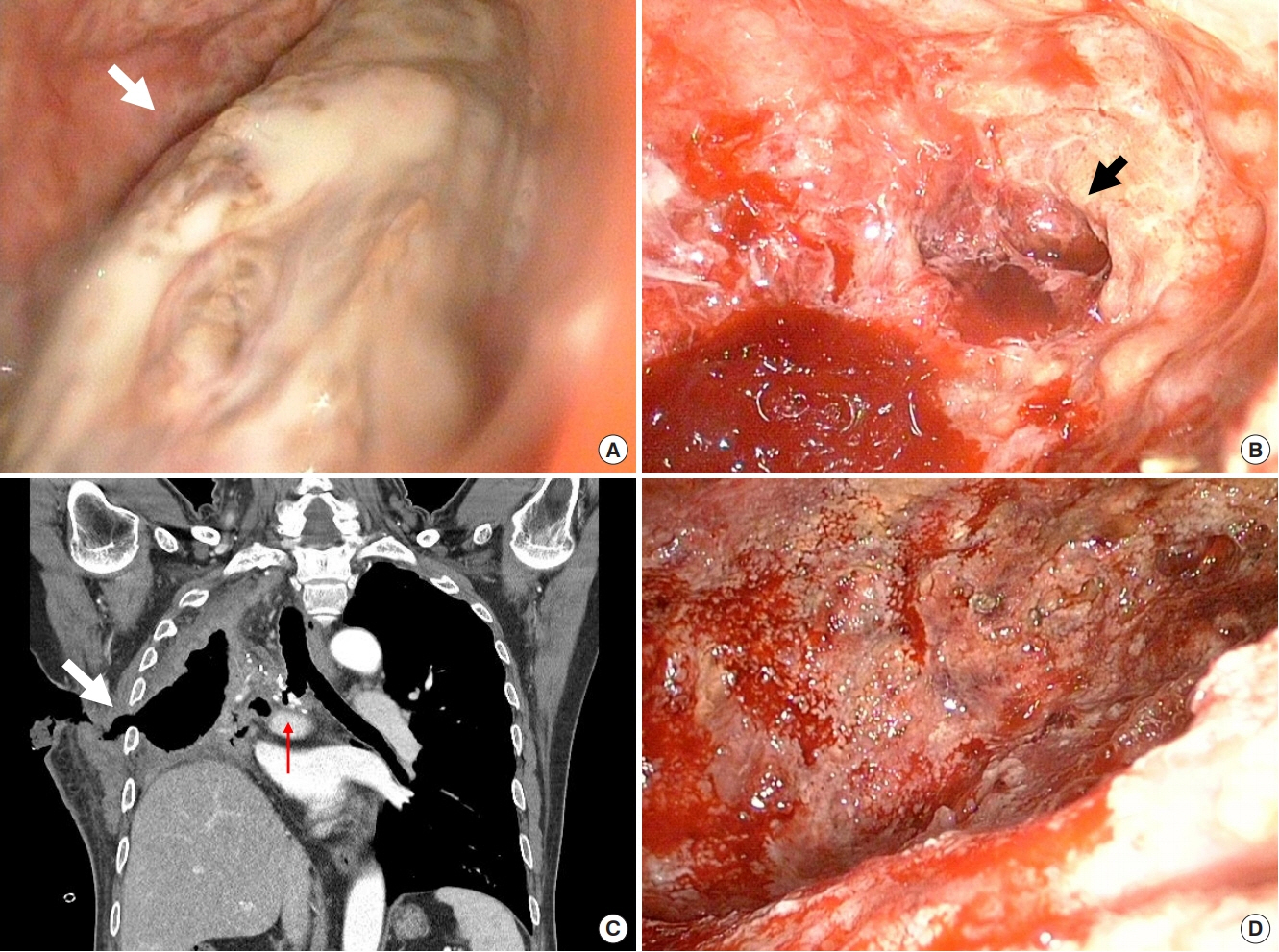
Figure 3. Video-assisted thoracoscopic exploration showed the fungal ball (white arrow) inside the right pulmonary cavity (A) and necrosis of the lung parenchyma (black arrow) after saline irrigation (B). (C) Chest computed tomography showed a bronchopleural fistula (red arrow) after trans-sternal trans-pericardial bronchial division and closure and an open wound (white arrow) of the chest wall after irrigation and drainage. (D) After exchanging a vacuum-assisted closure sponge under local anesthesia every 2 or 3 days, we performed follow-up pleural fluid culture every 3 days and found no bacterial growth.

Figure 4. (A) After performing a complete pneumonectomy, we closed the bronchopleural fistula (white arrow) using multiple interrupted sutures (asterisk). (B) A serratus anterior muscle flap (SA) was used to cover the shortened bronchial stump, and the latissimus dorsi (LD) with intercostal muscles was transferred to pack the intrathoracic dead space. (C) On post-pneumonectomy day 10, we confirmed in the operating room that the pleural cavity was clean. (D) The postoperative chest computed tomography showed a shortened right-side bronchial stump covered by the pedicled SA and LD packed into the thoracic cavity (white arrow). (E) One year later, the patient visited the outpatient department without recurrence.
Reference
-
1. Abruzzini P. Surgical treatment of fistulae of the main bronchus after pneumonectomy in tuberculosis (personal technic). Thoraxchirurgie. 1963; 10:259–64.2. Fournier I, Krueger T, Wang Y, Meyer A, Ris HB, Gonzalez M. Tailored thoracomyoplasty as a valid treatment option for chronic postlobectomy empyema. Ann Thorac Surg. 2012; 94:387–93.
Article3. Botianu PV, Botianu AM. Thoracomyoplasty in the treatment of empyema: current indications, basic principles, and results. Pulm Med. 2012; 2012:418514.
Article4. Hysi I, Rousse N, Claret A, Bellier J, Pinçon C, Wallet F, et al. Open window thoracostomy and thoracoplasty to manage 90 postpneumonectomy empyemas. Ann Thorac Surg. 2011; 92:1833–9.
Article5. Haghshenasskashani A, Rahnavardi M, Yan TD, McCaughan BC. Intrathoracic application of a vacuum-assisted closure device in managing pleural space infection after lung resection: is it an option? Interact Cardiovasc Thorac Surg. 2011; 13:168–74.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Postpneumonectomy Empyema with Bronchopleural Fistula Treated with Vacuum-assisted Closure Device
- Use of the Free Flap for Large Defect with Bronchopleural Fistula: Case Report
- Endobronchial Closure of Postoperative Bronchopleural Fistula Using Vascular Occluding Coils
- Various Bronchial Fistulas: Pitfalls and Usefulness on CT. A Pictorial Review
- Bronchopleural Fistula after Pneumonectomy: Autosuture Versus Manual Suture
