Comparison between Anterior Cervical Decompression with Fusion and Posterior Cervical Fusion with Wide Facetectomy for Treatment of Severe Bony Foraminal Stenosis
- Affiliations
-
- 1Department of Neurosurgery, Kyungpook National University Hospital, Daegu, Korea
- 2Department of Neurosurgery, School of Medicine, Kyungpook National University, Daegu, Korea
- 3Department of Neurosurgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 4Department of Neurosurgery, Dongtan Sacred Heart Hospital, University of Hallym University, Hwaseong, Korea
- KMID: 2517688
- DOI: http://doi.org/10.3340/jkns.2020.0263
Abstract
Objective
: To compare the anterior cervical discectomy and fusion (ACDF) and posterior cervical fusion (PCF) with wide facetectomy in the treatment of parallel-shaped bony foraminal stenosis (FS).
Methods
: Thirty-six patients underwent surgery due to one-or-two levels of parallel-shaped cervical FS. ACDF was performed in 16 patients, and PCF using CPS was performed in 20 patients. All patients were followed up at 1, 3, 6, and 12 months postoperatively. Standardized outcome measures such as Numeric rating scale (NRS) score for arm/neck pain and Neck disability index (NDI) were evaluated. Cervical radiographs were used to compare the C2–7 Cobb’s angle, segmental angle, and fusion rates.
Results
: There was an improvement in NRS scores after both approaches for radicular arm pain (mean change -6.78 vs. -8.14, p=0.012), neck pain (mean change -1.67 vs. -4.36, p=0.038), and NDI score (-19.69 vs. -18.15, p=0.794). The segmental angle improvement was greater in the ACDF group than in the posterior group (9.4°±2.7° vs. 3.3°±5.1°, p=0.004). However, there was no significant difference in C2–7 Cobb angle between groups (16.2°±7.9° vs. 14.8°±8.5°, p=0.142). As a complication, dysphagia was observed in one case of the ACDF group.
Conclusion
: In the treatment of parallel-shaped bony FS up to two surgical levels, segmental angle improvement was more favorable in patients who underwent ACDF. However, PCF with wide facetectomy using CPS should be considered as an alternative treatment option in cases where the anterior approach is burdensome.
Figure
-

Fig. 1. The shape of narrowed foramen on axial computed tomography scans. A : Parallel-shaped foraminal stenosis (FS) on the intervertebral level. The entire path of foramen was narrowed from the entrance zone to the exit zone. B : In contrast to parallel-shaped FS, V-shaped FS becomes wider at the exit zone.

Fig. 2. A 70-year-old man with tingling in both arms and left elbow flexion weakness. Severe parallel shape foraminal stenosis (FS) was seen on preoperative computed tomography (cT) imaging, with the left FS being more pronounced. A : Preoperative sagittal cT image show the c5–6, c6–7 foramen. B : Preoperative axial cT image of the c5–6 level foramen. c : Sagittal cT image of 12 months after c5–6 and c6–7 wide facetectomy (Ponte osteotomy) with fusion. cervical pedical screws were inserted into both sides of c6 and c7, and lateral mass screws were inserted into both sides of the c5. d : Axial cT image of the c5–6 level 12 months after surgery. Both sides of the c6 superior articular processes were removed, and the entire path of c5–6 foramen was widened.
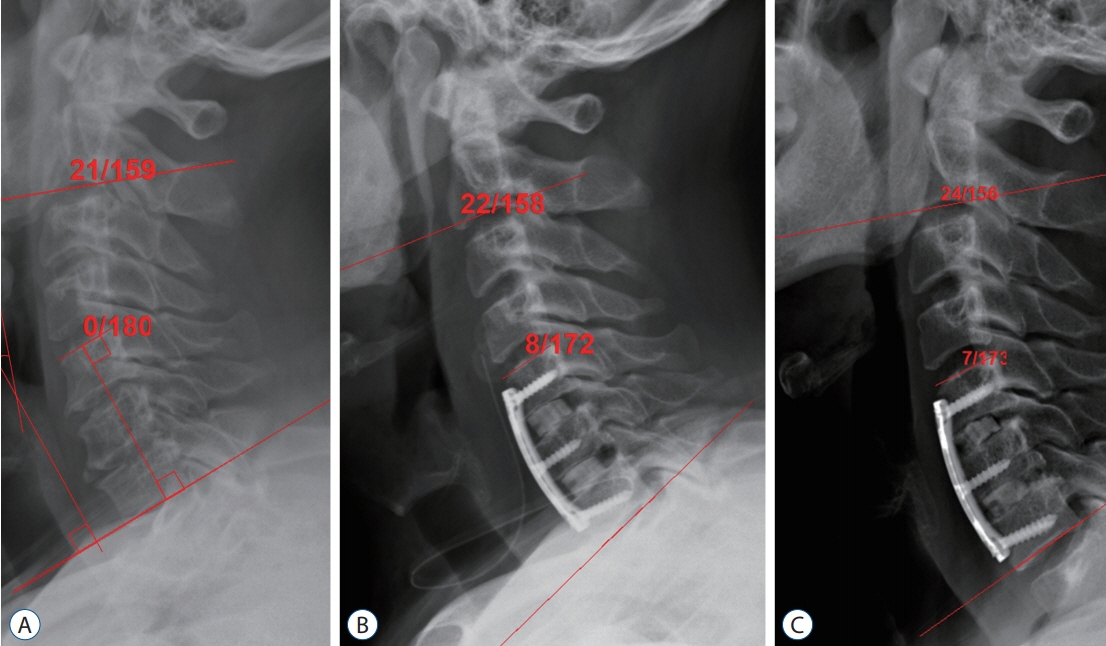
Fig. 3. A lateral cervical X-ray of a patient in a neutral position shows the c2–7 cobb angle measurement between the lower border of the c2 body and the lower border of the c7 body. The segmental angle measurement is made between the lower border of the distal instrumented vertebral body and the upper border of the proximal instrumented vertebral body. A : Preoperative image. B : Immediate postoperative image. The segmental angle of surgical index level increased after anterior cervical decompression, c5–6–7. c : X-ray image of 12 months after surgery. The segmental angle and c2–7 cobb angle remained well after 12 months.

Fig. 4. An illustration showing an exposed screw tip or thread of a lateral mass screw during resection of the superior and inferior articular process. In cases of wide facetectomy (red dashed line), the lateral mass screw is partially exposed, but the trajectory of the cervical pedicle screw is not affected by it.
Reference
-
References
1. Abumi K. Cervical spondylotic myelopathy: posterior decompression and pedicle screw fixation. Eur Spine J 24 Suppl. 2:186–196. 2015.
Article2. Abumi K, Ito M, Sudo H. Reconstruction of the subaxial cervical spine using pedicle screw instrumentation. Spine (Phila Pa 1976). 37:E349–E356. 2012.
Article3. Ames CP, Smith JS, Scheer JK, Shaffrey CI, Lafage V, Deviren V, et al. A standardized nomenclature for cervical spine soft-tissue release and osteotomy for deformity correction: clinical article. J Neurosurg Spine. 19:269–278. 2013.
Article4. Bartolomei J, Sonntag V. Anterior approach including cervical corpectomy. In : Winn HR, Youmans JR, editors. Youmans Neurological Surgery. ed 5. Philadelphia: Saunders;2004. p. 4431–4445.5. Chon H, Park JH. Cervical vertebral body fracture with ankylosing spondylitis treated with cervical pedicle screw: a fracture body overlapping reduction technique. J Clin Neurosci. 41:150–153. 2017.
Article6. Cunningham BW, Sefter JC, Shono Y, McAfee PC. Static and cyclical biomechanical analysis of pedicle screw spinal constructs. Spine (Phila Pa 1976). 18:1677–1688. 1993.
Article7. Dodwad SJ, Dodwad SN, Prasarn ML, Savage JW, Patel AA, Hsu WK. Posterior cervical foraminotomy: indications, technique, and outcomes. Clin Spine Surg. 29:177–185. 2016.8. Fessler RG, Khoo LT. Minimally invasive cervical microendoscopic foraminotomy: an initial clinical experience. Neurosurgery. 51(5 Suppl):S37–S45. 2002.
Article9. Gu BS, Choi SJ, Yoo B, Han KH, Park JK, Lee YS, et al. An incidental finding of a radiopaque pill following cervical spinal surgery in a Parkinson’s disease patient. Korean J Spine. 12:153–155. 2015.
Article10. Gu BS, Park JH, Seong HY, Jung SK, Roh SW. Feasibility of posterior cervical foraminotomy in cervical foraminal stenosis: prediction of surgical outcomes by the foraminal shape on preoperative computed tomography. Spine (Phila Pa 1976). 42:E267–E271. 2017.11. Gutman G, Rosenzweig DH, Golan JD. Surgical treatment of cervical radiculopathy: meta-analysis of randomized controlled trials. Spine (Phila Pa 1976). 43:E365–E372. 2018.12. Hasegawa K, Hirano T, Shimoda H, Homma T, Morita O. Indications for cervical pedicle screw instrumentation in nontraumatic lesions. Spine (Phila Pa 1976). 33:2284–2289. 2008.
Article13. Heo Y, Lee SB, Lee BJ, Jeong SK, Rhim SC, Roh SW, et al. The learning curve of subaxial cervical pedicle screw placement: how can we avoid neurovascular complications in the initial period? Oper Neurosurg (Hagerstown). 17:603–607. 2019.
Article14. Johnston TL, Karaikovic EE, Lautenschlager EP, Marcu D. Cervical pedicle screws vs. lateral mass screws: uniplanar fatigue analysis and residual pullout strengths. Spine J. 6:667–672. 2006.
Article15. Kang MS, Choi KC, Lee CD, Shin YH, Hur SM, Lee SH. Effective cervical decompression by the posterior cervical foraminotomy without discectomy. J Spinal Disord Tech. 27:271–276. 2014.
Article16. Kerry G, Hammer A, Ruedinger C, Ranaie G, Steiner HH. Microsurgical posterior cervical foraminotomy: a study of 181 cases. Br J Neurosurg. 31:39–44. 2017.
Article17. Kim HB, Lee MK, Lee YS, Sohn JY, Jung SK, Park JH. An assessment of the medial angle of inserted subaxial cervical pedicle screw during surgery: practical use of preoperative CT scanning and intraoperative X-rays. Neurol Med Chir (Tokyo). 57:159–165. 2017.
Article18. Lee DH, Cho JH, Baik JM, Joo YS, Park S, Min WK, et al. Does additional uncinate resection increase pseudarthrosis following anterior cervical discectomy and fusion? Spine (Phila Pa 1976). 43:97–104. 2018.
Article19. Lee JK, Jung SK, Lee YS, Jeon SR, Roh SW, Rhim SC, et al. Analysis of the fusion and graft resorption rates, as measured by computed tomography, 1 year after posterior cervical fusion using a cervical pedicle screw. World Neurosurg. 99:171–178. 2017.
Article20. Lee S, Jung SK, Kim HB, Roh SW, Jeon SR, Park JH. Postoperative non-pathological fever following posterior cervical fusion surgery : is laminoplasty a better preventive method than laminectomy? J Korean Neurosurg Soc. 63:487–494. 2020.
Article21. Lee S, Seo J, Lee MK, Jeon SR, Roh SW, Rhim SC, et al. Widening of the safe trajectory range during subaxial cervical pedicle screw placement: advantages of a curved pedicle probe and laterally located starting point without creating a funnel-shaped hole. J Neurosurg Spine. 27:150–157. 2017.
Article22. Lee SH, Lee JS, Sung SK, Son DW, Lee SW, Song GS. The effect of uncinate process resection on subsidence following anterior cervical discectomy and fusion. J Korean Neurosurg Soc. 60:550–559. 2017.
Article23. Nakagawa H, Saito K, Mitsugi T, Yagi K, Kanno A. Microdiscectomy and foraminotomy in cervical spondylotic myelopathy and radiculopathy: anterior versus posterior, microendoscopic surgery versus mini-open microsurgery. World Neurosurg. 81:292–293. 2014.
Article24. Pakzaban P. Ultrasonic total uncinectomy: a novel technique for complete anterior decompression of cervical nerve roots. Neurosurgery 10 Suppl. 4:535–541. discussion 541. 2014.
Article25. Park JH, Jeon SR, Roh SW, Kim JH, Rhim SC. The safety and accuracy of freehand pedicle screw placement in the subaxial cervical spine: a series of 45 consecutive patients. Spine (Phila Pa 1976). 39:280–285. 2014.
Article26. Park JH, Roh SW, Rhim SC. A single-stage posterior approach with open reduction and pedicle screw fixation in subaxial cervical facet dislocations. J Neurosurg Spine. 23:35–41. 2015.
Article27. Park JH, Roh SW, Rhim SC. Response. J Neurosurg Spine. 24:673. 2016.28. Polly DW Jr, Klemme WR, Cunningham BW, Burnette JB, Haggerty CJ, Oda I. The biomechanical significance of anterior column support in a simulated single-level spinal fusion. J Spinal Disord. 13:58–62. 2000.
Article29. Rho YJ, Choe WJ. Double crush syndrome caused by cervical spondylosis and vertebral artery loop. Eur Spine J. 28:292–296. 2019.
Article30. Roh SW, Kim DH, Cardoso AC, Fessler RG. Endoscopic foraminotomy using MED system in cadaveric specimens. Spine (Phila Pa 1976). 25:260–264. 2000.
Article31. Tan LA, Riew KD, Traynelis VC. Cervical spine deformity-part 3: posterior techniques, clinical outcome, and complications. Neurosurgery. 81:893–898. 2017.
Article32. Zeidman SM, Ducker TB. Posterior cervical laminoforaminotomy for radiculopathy: review of 172 cases. Neurosurgery. 33:356–362. 1993.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior Facetectomy with Fusion Using a Pedicle Screw for Parallelshaped Cervical Foraminal Stenosis
- Treatment of Ossification of Posterior Longitudinal Ligament in Cervical Spine with Anterior Fusion and Anterior Decompression: Report of 3 Cases
- Anterior Decompression and Fusion for the Treatment of Cervical Myelopathy Caused by Ossification of the Posterior Longitudinal Ligament: A Narrative Review
- Comparison of the Morphometric Changes in the Cervical Foramen: Anterior Cervical Discectomy and Fusion versus Posterior Foraminotomy
- Posterior Decompression and Fusion in Patients with Multilevel Lumbar Foraminal Stenosis: A Comparison of Segmental Decompression and Wide Decompression
