Fetal development of the carotid canal with special reference to a contribution of the sphenoid bone and pharyngotympanic tube
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Tohoku University School of Medicine, Sendai, Japan
- 2Department of Anatomy, Tokyo Dental College, Tokyo, Japan
- 3Department of Anatomy and Embryology, School of Medicine, Complutense University of Madrid, Madrid, Spain
- 4Division of Internal Medicine, Cupid Clinic, Iwamizawa, Japan
- 5Akita University School of Medicine, Akita, Japan
- KMID: 2516910
- DOI: http://doi.org/10.5115/acb.20.310
Abstract
- The bony carotid canal is a tube-like bone with a rough surface in contrast to smooth surfaces of the other parts of the temporal bone petrosal portion (petrosa): it takes an impression of the additional, out-sourcing product. No study had been conducted to evaluate a contribution of the adjacent sphenoid and pharyngotympanic tube (PTT) to the carotid canal. We examined sagittal and horizontal histological sections of hemi-heads from 37 human fetuses at 10 to 37 weeks. At 10 to 18 weeks, the future carotid canal was identified as a wide loose space between the cartilaginous cochlea and the ossified or cartilaginous sphenoid elements (ala temporalis and pterygoid). A linear mesenchymal condensation extending between the cochlear wall and ala temporalis suggested the future antero-inferior margin of the carotid canal. This delineation was more clearly identified in later stages. After 25 weeks, 1) the growing pterygoid pushed the PTT upward and, in turn, the PTT pushed the internal carotid artery (ICA) upward toward the petrosa: 2) a membranous ossification occurs in the dense mesenchymal tissue, the latter of which took an appearance of an anterior process of the petrosa; 3) the bony process of the petrosa involved the ICA inside or posteriorly. The bony carotid canal was made with membranous ossification in the dense mesenchymal tissue between the petrosa and sphenoid. The mother tissue was detached from the sphenoid by the PTT. The ossification of the septum between the ICA and tympanic cavity seemed to continue after birth.
Figure
-
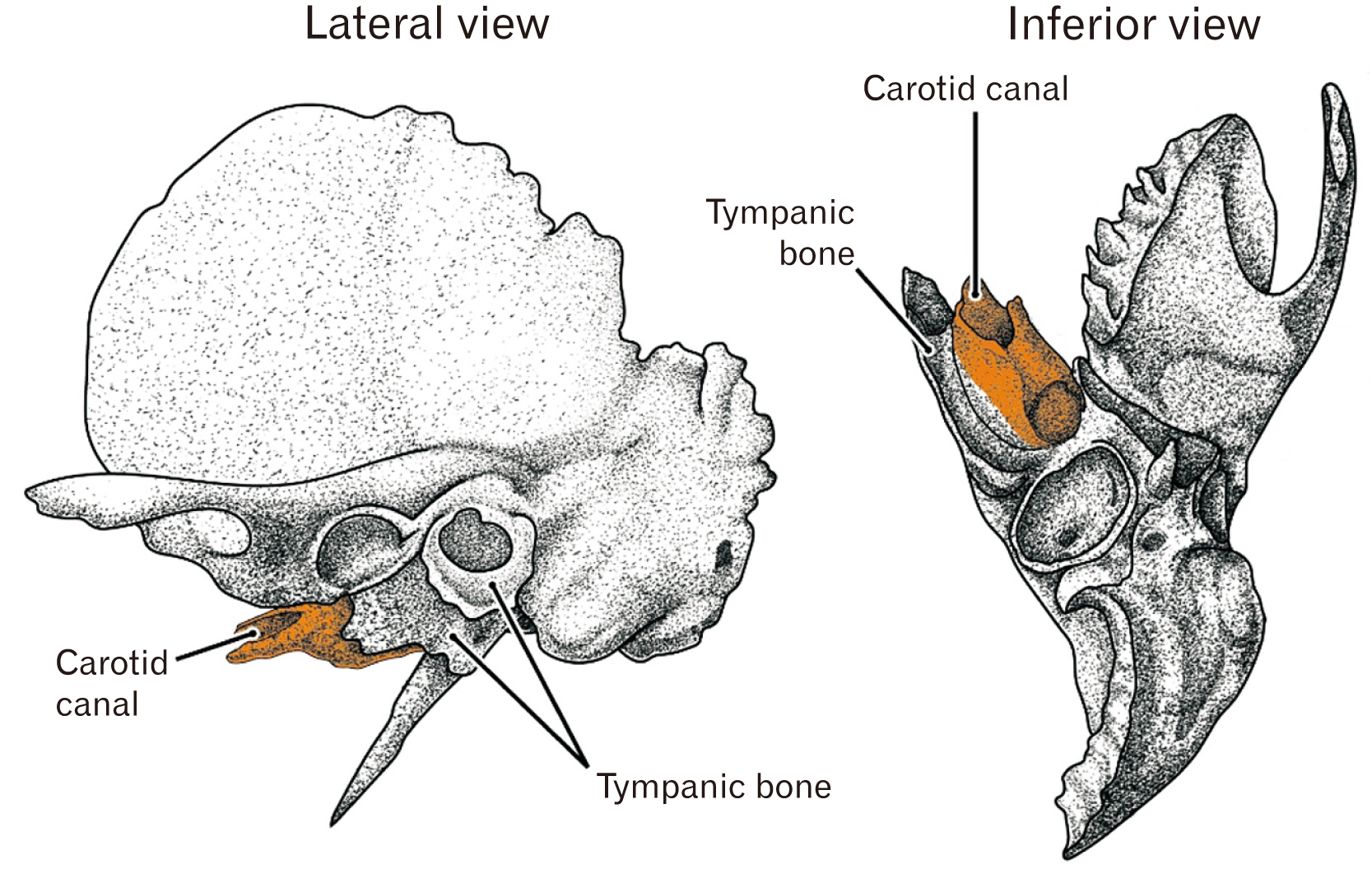
Fig. 1 Temporal bone in adults: the lateral and inferior views. The carotid canal (colored orange) as well as the tympanic bone has rough external surfaces and they appear to additionally attach to the inferolateral aspect of the temporal bone.

Fig. 2 Initial carotid canal in sagittal sections: a wide gap or loose space between the cochlear wall and the sphenoid. Azan staining (A–D) or H&E staining (E, F). (A, B) A fetus of crown-rump length (CRL) 97 mm (approximately 13 weeks); (C, D) CRL 100 mm (13 weeks); (E, F) CRL 105 mm (14 weeks). (B) and (D) are higher magnification view of the center of (A) and (C), respectively. (F) is a higher magnification view of a square in (E). The left-hand side of each panel corresponds to the anterior side of the head. The ala temporalis of the sphenoid (ala) is ossified in (B) and (D), while it is cartilaginous in (E). In (D), an inferior part of the ala (ala with asterisk) looks like a pterygoid. In contrast, most parts of the pterygoid of the sphenoid is bony (B, E). (F) Shows the pterygoid containing two modes of the ossification. (B, D, E) Stars indicate a linear mesenchymal condensation corresponding to the future antero-inferior margin of the petrosal part of the temporal bone. Scale bars: (A, C) 5 mm; (B, D, E) 1 mm; (F) 0.1 mm. ABD, abducant nerve; AP, alar process; DPN, deep petrosal nerve; ICA, internal carotid artery; IR, inferior rectus of the eye; PPG, pterygopalatine ganglion; PTT, pharyngotympanic tube; tent, tentorium cerebelli; TG, trigeminal ganglion.

Fig. 3 Initial carotid canal in horizontal sections: a slit surrounded by the cochlear wall, alar process (AP) and basisphenoid. Azan staining. (A–C) A fetus of crown-rump length (CRL) 49 mm (approximately 10 weeks); (D) CRL 52 mm (10 weeks); (E) CRL 95 mm (13 weeks); (F) CRL 100 mm (14 weeks). The upper side of each panel corresponds to the anterior side of the head. The basisphenoid, a large cartilage mass, contains both the notochord (NC) and hypophysial fossa (fossa). The internal carotid artery is surrounded by the petrosa or cochlear wall posteriorly, the AP anteriorly and the basisphenoid medially. A slit between the petrosa and sphenoid appears to be narrower in larger specimens. All scale bars: 1 mm. chiasma, optic chiasma; HP, hypophysis; ICA, internal carotid artery; ON, optic nerve; SPS, superior petrosal sinus; TG, trigeminal ganglion.

Fig. 4 Wide and dense mesenchymal tissue containing the internal carotid artery and extending between the cochlear wall and sphenoid. Horizontal sections. A fetus of crown-rump length (CRL) 228 mm (approximately 28 weeks). H&E staining. (A) or (D) displays the most superior (or inferior) site in the figure. (E–G) are higher magnification views of squares in (A), (B), and (D), respectively. The left-hand side of each panel corresponds to the anterior side of the head. In these superior sections, no structure delineates the future carotid canal except for the bony alar process (AP) of the sphenoid. Instead, a dense mesenchymal tissue extends between the cochlear wall and sphenoid and it contains abundant veins. (A–D) or (E–G) were prepared at the same magnification; (A, E) Scale bar: 1 mm. ala, ala temporalis of the sphenoid; GPN, greater petrosal nerve; ICA, internal carotid artery; ICN, internal carotid nerve; MXN, maxillary nerve (intracranial course); TG, trigeminal ganglion.

Fig. 5 Initial ossification of the carotid canal starts in the dense mesenchymal tissue connecting to the anterosuperior end of the cochlear wall. Sagittal sections. A fetus of crown-rump length (CRL) 276 mm (approximately 32 weeks). H&E staining. Panel (A) containing the future cavernous sinus, displays the most medial site in the figure. (C) and (E) are higher magnification views of squares in (B) and (D), respectively. Panel (F) corresponding to a square in (E), exhibits the membranous ossification starts in the in the dense mesenchymal tissue connecting to the anterior end of the cochlear wall. The left-hand side of each panel corresponds to the anterior side of the head. Note an inferior margin (stars in A–E) of the dense mesenchymal tissue extends between the cochlear wall and the sphenoid (the alar process [AP], ala temporalis [ala] and pterygoid): it connects with the pharyngotympanic tube cartilage in (B) and (D). The palatine bone (PB) looks like a part of the pterygoid (A). Scale bars: (A–E) 1 mm; (F) 0.1 mm. ala, ala temporalis of the sphenoid; ABN, abducant nerve; ICA, internal carotid artery; IR, inferior rectus of the eye; MXN, maxillary nerve in the round foramen; OCN, oculomotor nerve; PPG, pterygopalatine ganglion; PTT, pharyngotympanic tube; SPS, superior petrosal sinus; TG, trigeminal ganglion.

Fig. 6 Carotid canal is involved into the bony cochlear wall. Sagittal sections. A fetus of crown-rump length (CRL) 274 mm (approximately 31 weeks). H&E staining. The left-hand side of each panel corresponds to the superior side of the head. Panel (A) containing the future cavernous sinus, displays the most medial site in the figure. (B) or (C) is a higher magnification view of a square in (A) or (B). The inferior side of each panel corresponds to the anterior side of the head (long arrow in A). In the medial part of the carotid canal (A–C), a membranous ossification is on-going. In contrast, in the lateral part, a bony process of the cochlear wall (arrow in D, E) appears to surround the carotid canal from the inferior side rather than from the superior side (Fig. 3D). Stars in (D) indicate an inferior margin of the dense mesenchymal tissue (corresponding to that in Fig. 3A, B) extends between the cochlear wall and sphenoid (ala temporalis or ala). Asterisk in (F) indicates the medial end of the growing tympanic cavity. Scale bars: (A, B, D–F) 1 mm; (C) 0.1 mm. AP, alar process of the sphenoid; ICA, internal carotid artery; ICN, internal carotid nerve; MHT, meningohypophysial trunk of the internal carotid artery; OPN, ophthalmic nerve; PTT, pharyngotympanic tube; SPS, superior petrosal sinus; TG, trigeminal ganglion.

Fig. 7 Carotid and facial nerve canals adjacent to the tympanic cavity: membranous ossification in these septa. Sagittal sections. A fetus of crown-rump length (CRL) 272 mm (approximately 31 weeks). H&E staining. The left-hand side of each panel corresponds to the posterior side of the head. Panel (A) displays a plane 1.2 mm medial to (B). (A, B) Contain the carotid and facial nerve canals: the septum is developing for the internal carotid artery (ICA), while the latter canal still opens widely to the tympanic cavity (arrows in B). (C) or (E) is a higher magnification view of a square in panel (A) or (D). The left-hand side of each panel corresponds to the anterior side of the head. Near the facial nerve, membranous ossification (upper insert of C) coexist endochondral ossification indicated by a tidemark (arrowheads; lower insert). (D) A section near (B), exhibits a site corresponding to a square in (B). (E) A higher magnification view of a square in (D), shows membranous ossification in a septum between the carotid canal and tympanic cavity. Scale bars: (A–D) 1 mm; (E) 0.1 mm. Magnification of inserts, same as (E). ant, anterior; infe, inferior; ICN, internal carotid nerve; LSC, lateral semicircular canal.
Reference
-
References
1. Katori Y, Rodríguez-Vázquez JF, Verdugo-López S, Murakami G, Kawase T, Kobayashi T. 2012; Initial stage of fetal development of the pharyngotympanic tube cartilage with special reference to muscle attachments to the tube. Anat Cell Biol. 45:185–92. DOI: 10.5115/acb.2012.45.3.185. PMID: 23094207. PMCID: PMC3472145.
Article2. Jin ZW, Cho KH, Abe H, Katori Y, Murakami G, Rodríguez-Vázquez JF. 2017; Fetal facial nerve course in the ear region revisited. Surg Radiol Anat. 39:885–95. DOI: 10.1007/s00276-017-1818-y. PMID: 28194509.
Article3. Zhang Q, Wang H, Udagawa J, Otani H. 2011; Morphological and morphometric study on sphenoid and basioccipital ossification in normal human fetuses. Congenit Anom (Kyoto). 51:138–48. DOI: 10.1111/j.1741-4520.2011.00322.x. PMID: 21848997.
Article4. Santaolalla-Montoya F, Martinez-Ibargüen A, Sánchez-Fernández JM, Sánchez-del-Rey A. 2012; Principles of cranial base ossification in humans and rats. Acta Otolaryngol. 132:349–54. DOI: 10.3109/00016489.2011.642814. PMID: 22201370.
Article5. Hayashi S, Kim JH, Hwang SE, Shibata S, Fujimiya M, Murakami G, Cho BH. 2014; Interface between intramembranous and endochondral ossification in human foetuses. Folia Morphol (Warsz). 73:199–205. DOI: 10.5603/FM.2014.0029. PMID: 24902099.
Article6. Michaels L, Soucek S, Linthicum F. 2010; The intravestibular source of the vestibular aqueduct. II: its structure and function clarified by a developmental study of the intra-skeletal channels of the otic capsule. Acta Otolaryngol. 130:420–8. DOI: 10.3109/00016480903253561. PMID: 19895329. PMCID: PMC2865695.
Article7. Bast TH, Anson BJ. 1949. The temporal bone and the ear. Thomas;Springfield:8. Anson BJ, Donaldson JA. 1973. Surgical anatomy of the temporal bone and ear. 2nd ed. WB Saunders;Philadelphia:9. Nemzek WR, Brodie HA, Chong BW, Babcook CJ, Hecht ST, Salamat S, Ellis WG, Seibert JA. 1996; Imaging findings of the developing temporal bone in fetal specimens. AJNR Am J Neuroradiol. 17:1467–77. PMID: 8883642.10. Richard C, Courbon G, Laroche N, Prades JM, Vico L, Malaval L. 2017; Inner ear ossification and mineralization kinetics in human embryonic development- microtomographic and histomorphological study. Sci Rep. 7:4825. DOI: 10.1038/s41598-017-05151-0. PMID: 28684743. PMCID: PMC5500530.
Article11. Abing W, Rauchfuss A. 1987; Fetal development of the tympanic part of the facial canal. Arch Otorhinolaryngol. 243:374–7. DOI: 10.1007/BF00464645. PMID: 3566620.
Article12. Spector JG, Ge X. 1993; Ossification patterns of the tympanic facial canal in the human fetus and neonate. Laryngoscope. 103:1052–65. DOI: 10.1288/00005537-199309000-00018. PMID: 8361310.
Article13. Yamamoto M, Kitamura K, Kasahara M, Serikawa M, Katumura S, Yoshimoto T, Matubayashi T, Odaka K, Matsunaga S, Abe S. 2017; Histological study of the developing pterygoid process of the fetal mouse sphenoid. Anat Sci Int. 92:364–72. DOI: 10.1007/s12565-016-0340-3. PMID: 27015685.
Article14. Yamamoto M, Takada H, Ishizuka S, Kitamura K, Jeong J, Sato M, Hinata N, Abe S. 2020; Morphological association between the muscles and bones in the craniofacial region. PLoS One. 15:e0227301. DOI: 10.1371/journal.pone.0227301. PMID: 31923241. PMCID: PMC6953862.
Article15. Katori Y, Kawamoto A, Cho KH, Ishii K, Abe H, Abe S, Rodríguez-Vázquez JF, Murakami G, Kawase T. 2013; Transsphenoidal meningocele: an anatomical study using human fetuses including report of a case. Eur Arch Otorhinolaryngol. 270:2729–36. DOI: 10.1007/s00405-013-2392-5. PMID: 23408024.
Article16. Cho KH, Chang H, Yamamoto M, Abe H, Rodríguez-Vázquez JF, Murakami G, Katori Y. 2013; Rathke's pouch remnant and its regression process in the prenatal period. Childs Nerv Syst. 29:761–9. DOI: 10.1007/s00381-012-2015-2. PMID: 23314691.
Article17. Katori Y, Kawase T, Cho KH, Abe H, Rodríguez-Vázquez JF, Murakami G, Abe S. 2012; Prestyloid compartment of the parapharyngeal space: a histological study using late-stage human fetuses. Surg Radiol Anat. 34:909–20. DOI: 10.1007/s00276-012-0975-2. PMID: 22576264.
Article18. Katori Y, Kawase T, Ho Cho K, Abe H, Rodríguez-Vázquez JF, Murakami G, Fujimiya M. 2013; Suprahyoid neck fascial configuration, especially in the posterior compartment of the parapharyngeal space: a histological study using late-stage human fetuses. Clin Anat. 26:204–12. DOI: 10.1002/ca.22088. PMID: 22576755.
Article19. Sánchez-Fernández JM, Saint-Gerons S, Sánchez del Rey A. 1992; A microanalytical study on human auditory ossicles in normal and pathological conditions. Acta Otolaryngol. 112:317–21. DOI: 10.1080/00016489.1992.11665425. PMID: 1604999.20. Ohtsuki S, Ishikawa A, Yamada S, Imai H, Matsuda T, Takakuwa T. 2018; Morphogenesis of the middle ear during fetal development as observed via magnetic resonance imaging. Anat Rec (Hoboken). 301:757–64. DOI: 10.1002/ar.23760. PMID: 29266805.
Article21. Nemzek WR, Brodie HA, Hecht ST, Chong BW, Babcook CJ, Seibert JA. 2000; MR, CT, and plain film imaging of the developing skull base in fetal specimens. AJNR Am J Neuroradiol. 21:1699–706. PMID: 11039353. PMCID: PMC8174876.22. Jeffery N, Spoor F. 2004; Ossification and midline shape changes of the human fetal cranial base. Am J Phys Anthropol. 123:78–90. DOI: 10.1002/ajpa.10292. PMID: 14669239.
Article23. Weninger WJ, Müller GB. 1997; The sympathetic nerves of the parasellar region: pathways to the orbit and the brain. Acta Anat (Basel). 160:254–60. DOI: 10.1159/000148019. PMID: 9732126.
Article24. Weninger WJ, Müller GB. 1999; The parasellar region of human infants: cavernous sinus topography and surgical approaches. J Neurosurg. 90:484–90. DOI: 10.3171/jns.1999.90.3.0484. PMID: 10067917.
Article25. Sato M, Cho KH, Yamamoto M, Hirouchi H, Murakami G, Abe H, Abe S. 2020; Cavernous sinus and abducens nerve in human fetuses near term. Surg Radiol Anat. 42:761–70. DOI: 10.1007/s00276-020-02443-5. PMID: 32112281.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Initial stage of fetal development of the pharyngotympanic tube cartilage with special reference to muscle attachments to the tube
- Feasibility and Safety of Superolateral Sphenoidotomy: Radiologic Study by Analyzing Multiplanar Reconstructive CT Scans
- Pneumatization of the sphenoid sinus and its surrounding neurovascular structures
- Tuberculoma Masquerading as a Meningioma: Case Report
- Ruptured Infectious Internal Carotid Artery Aneurysm Presenting with Epistaxis: A Case Report
