Artificial Intelligence in Lower Gastrointestinal Endoscopy: The Current Status and Future Perspective
- Affiliations
-
- 1Digestive Endoscopy Unit and Gastroenterology, Fondazione Poliambulanza, Brescia, Italy
- 2Department of Gastroenterology, Fondazione Policlinico Universitario A. Gemelli IRCCS -Università Cattolica del Sacro Cuore, Roma, Italy
- KMID: 2516312
- DOI: http://doi.org/10.5946/ce.2020.082
Abstract
- The present manuscript aims to review the history, recent advances, evidence, and challenges of artificial intelligence (AI) in colonoscopy. Although it is mainly focused on polyp detection and characterization, it also considers other potential applications (i.e., inflammatory bowel disease) and future perspectives. Some of the most recent algorithms show promising results that are similar to human expert performance. The integration of AI in routine clinical practice will be challenging, with significant issues to overcome (i.e., regulatory, reimbursement). Medico-legal issues will also need to be addressed. With the exception of an AI system that is already available in selected countries (GI Genius; Medtronic, Minneapolis, MN, USA), the majority of the technology is still in its infancy and has not yet been proven to reach a sufficient diagnostic performance to be adopted in the clinical practice. However, larger players will enter the arena of AI in the next few months.
Figure
-
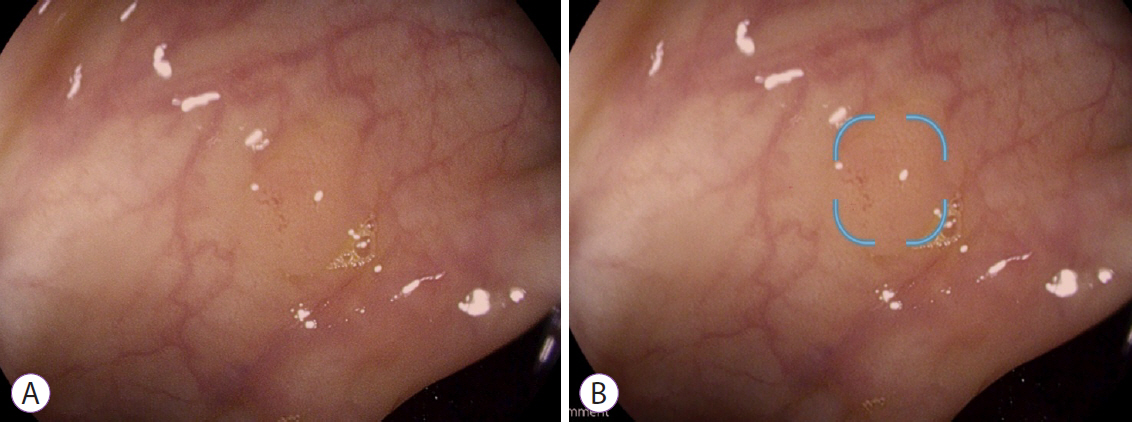
Fig. 1. A 5-mm polyp is visualized during colonoscopy (A) and with the support of DISCOVERY (PENTAX Medical, Tokyo, Japan) artificial intelligence system (B) which generates a small box on each frame where a polyp is detected.

Fig. 2. A 3-mm polyp is visualized during colonoscopy (A) and with the support of DISCOVERY (PENTAX Medical, Tokyo, Japan) artificial intelligence system (B) which generates a small box on each frame where a polyp is detected.
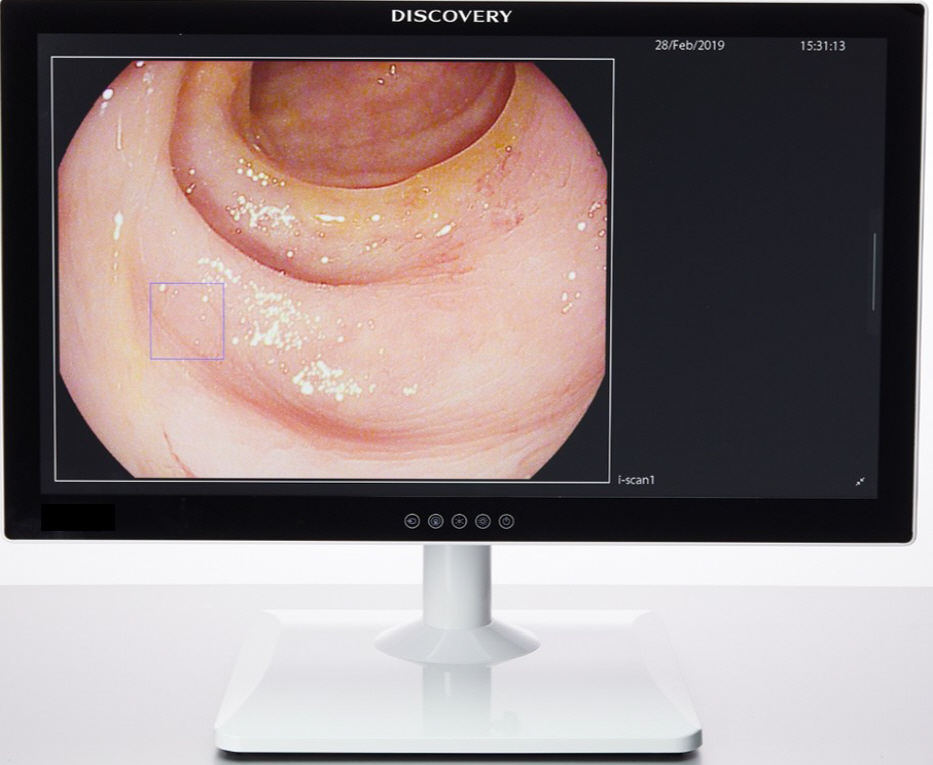
Fig. 3. DISCOVERY (PENTAX Medical, Tokyo, Japan) incorporates the artificial intelligence based on a deep neural network in a panel PC with a 32 inch LCD display. This panel PC can be connected with a signal cable (DVI/HD-SDI) to each PENTAX HD+ video processor for integration and is intended to be used as a secondary monitor.
Reference
-
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424.
Article2. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993; 329:1977–1981.3. Brenner H, Chang-Claude J, Jansen L, Knebel P, Stock C, Hoffmeister M. Reduced risk of colorectal cancer up to 10 years after screening, surveillance, or diagnostic colonoscopy. Gastroenterology. 2014; 146:709–717.
Article4. Zhao S, Wang S, Pan P, et al. Magnitude, risk factors, and factors associated with adenoma miss rate of tandem colonoscopy: a systematic review and meta-analysis. Gastroenterology. 2019; 156:1661–1674.e11.
Article5. Burt RW, Cannon JA, David DS, et al. Colorectal cancer screening. J Natl Compr Canc Netw. 2013; 11:1538–1575.6. Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators for colonoscopy and the risk of interval cancer. N Engl J Med. 2010; 362:1795–1803.
Article7. Corley DA, Jensen CD, Marks AR, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014; 370:1298–1306.
Article8. Marcondes FO, Gourevitch RA, Schoen RE, Crockett SD, Morris M, Mehrotra A. Adenoma detection rate falls at the end of the day in a large multi-site sample. Dig Dis Sci. 2018; 63:856–859.
Article9. Gkolfakis P, Tziatzios G, Facciorusso A, Muscatiello N, Triantafyllou K. Meta-analysis indicates that add-on devices and new endoscopes reduce colonoscopy adenoma miss rate. Eur J Gastroenterol Hepatol. 2018; 30:1482–1490.
Article10. Morris EJ, Rutter MD, Finan PJ, Thomas JD, Valori R. Post-colonoscopy colorectal cancer (PCCRC) rates vary considerably depending on the method used to calculate them: a retrospective observational population-based study of PCCRC in the English National Health Service. Gut. 2015; 64:1248–1256.
Article11. Wang Y, Tavanapong W, Wong J, Oh JH, de Groen PC. Polyp-Alert: near real-time feedback during colonoscopy. Comput Methods Programs Biomed. 2015; 120:164–179.
Article12. Fernández-Esparrach G, Bernal J, López-Cerón M, et al. Exploring the clinical potential of an automatic colonic polyp detection method based on the creation of energy maps. Endoscopy. 2016; 48:837–842.
Article13. Misawa M, Kudo SE, Mori Y, et al. Artificial intelligence-assisted polyp detection for colonoscopy: initial experience. Gastroenterology. 2018; 154:2027–2029.e3.
Article14. Urban G, Tripathi P, Alkayali T, et al. Deep learning localizes and identifies polyps in real time with 96% accuracy in screening colonoscopy. Gastroenterology. 2018; 155:1069–1078.e8.
Article15. Wang P, Berzin TM, Glissen Brown JR, et al. Real-time automatic detection system increases colonoscopic polyp and adenoma detection rates: a prospective randomised controlled study. Gut. 2019; 68:1813–1819.
Article16. Wang P, Liu X, Berzin TM, et al. Effect of a deep-learning computer-aided detection system on adenoma detection during colonoscopy (CADeDB trial): a double-blind randomised study. Lancet Gastroenterol Hepatol. 2020; 5:343–351.
Article17. Liu WN, Zhang YY, Bian XQ, et al. Study on detection rate of polyps and adenomas in artificial-intelligence-aided colonoscopy. Saudi J Gastroenterol. 2020; 26:13–19.
Article18. Gong D, Wu L, Zhang J, et al. Detection of colorectal adenomas with a real-time computer-aided system (ENDOANGEL): a randomised controlled study. Lancet Gastroenterol Hepatol. 2020; 5:352–361.
Article19. Hassan C, Wallace MB, Sharma P, et al. New artificial intelligence system: first validation study versus experienced endoscopists for colorectal polyp detection. Gut. 2020; 69:799–800.
Article20. Seibt H, Beyer A, Häfner M, Eggert C, Huber H, Rath T. Evaluation of a real-time artificial intelligence system using a deep neural network for polyp detection and localization in the lower gastrointestinal tract. Gastrointest Endosc. 2020; 91(6 Suppl):AB249.
Article21. Lui TKL, Guo CG, Leung WK. Accuracy of artificial intelligence on histology prediction and detection of colorectal polyps: a systematic review and meta-analysis. Gastrointest Endosc. 2020; 92:11–22.e6.22. Tischendorf JJ, Gross S, Winograd R, et al. Computer-aided classification of colorectal polyps based on vascular patterns: a pilot study. Endoscopy. 2010; 42:203–207.
Article23. Ahmad OF, Soares AS, Mazomenos E, et al. Artificial intelligence and computer-aided diagnosis in colonoscopy: current evidence and future directions. Lancet Gastroenterol Hepatol. 2019; 4:71–80.
Article24. Mori Y, Kudo SE, Misawa M, Mori K. Simultaneous detection and characterization of diminutive polyps with the use of artificial intelligence during colonoscopy. VideoGIE. 2019; 4:7–10.25. Kudo SE, Misawa M, Mori Y, et al. Artificial intelligence-assisted system improves endoscopic identification of colorectal neoplasms. Clin Gastroenterol Hepatol. 2020; 18:1874–1881.e2.
Article26. Chen PJ, Lin MC, Lai MJ, Lin JC, Lu HH, Tseng VS. Accurate classification of diminutive colorectal polyps using computer-aided analysis. Gastroenterology. 2018; 154:568–575.
Article27. Byrne MF, Chapados N, Soudan F, et al. Real-time differentiation of adenomatous and hyperplastic diminutive colorectal polyps during analysis of unaltered videos of standard colonoscopy using a deep learning model. Gut. 2019; 68:94–100.
Article28. Shahidi N, Rex DK, Kaltenbach T, Rastogi A, Ghalehjegh SH, Byrne MF. Use of endoscopic impression, artificial intelligence, and pathologist interpretation to resolve discrepancies between endoscopy and pathology analyses of diminutive colorectal polyps. Gastroenterology. 2020; 158:783–785.e1.
Article29. Zachariah R, Samarasena J, Luba D, et al. Prediction of polyp pathology using convolutional neural networks achieves “resect and discard” thresholds. Am J Gastroenterol. 2020; 115:138–144.
Article30. Maeda Y, Kudo SE, Mori Y, et al. Fully automated diagnostic system with artificial intelligence using endocytoscopy to identify the presence of histologic inflammation associated with ulcerative colitis (with video). Gastrointest Endosc. 2019; 89:408–415.
Article31. Ozawa T, Ishihara S, Fujishiro M, et al. Novel computer-assisted diagnosis system for endoscopic disease activity in patients with ulcerative colitis. Gastrointest Endosc. 2019; 89:416–421.e1.
Article32. Stidham RW, Liu W, Bishu S, et al. Performance of a deep learning model vs human reviewers in grading endoscopic disease severity of patients with ulcerative colitis. JAMA Netw Open. 2019; 2:e193963.
Article33. Takenaka K, Ohtsuka K, Fujii T, et al. Development and validation of a deep neural network for accurate evaluation of endoscopic images from patients with ulcerative colitis. Gastroenterology. 2020; 158:2150–2157.
Article34. Krishnan SM, Tan CS, Chan KL. Closed-boundary extraction of large intestinal lumen. In : . 1994. Nov. 3-6. Baltimore (MD), USA. Piscataway (NJ): IEEE;1994. p. 610–611.35. LeCun Y, Bengio Y, Hinton G. Deep learning. Nature. 2015; 521:436–444.
Article36. Krizhevsky A, Sutskever I, Hinton GE. ImageNet classification with deep convolutional neural networks. Commun ACM. 2017; 60:84–90.
Article37. Tziatzios G, Gkolfakis P, Triantafyllou K. Effect of fellow involvement on colonoscopy outcomes: a systematic review and meta-analysis. Dig Liver Dis. 2019; 51:1079–1085.
Article38. Rex DK, Kahi C, O’Brien M, et al. The american society for gastrointestinal endoscopy PIVI (preservation and incorporation of valuable endoscopic innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc. 2011; 73:419–422.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of artificial intelligence in diagnosing Barrett’s esophagus-related neoplasia
- Deep Learning in Upper Gastrointestinal Disorders: Status and Future Perspectives
- Application of artificial intelligence for diagnosis of early gastric cancer based on magnifying endoscopy with narrow-band imaging
- Application of Artificial Intelligence in Capsule Endoscopy: Where Are We Now?
- The Future of Capsule Endoscopy: The Role of Artificial Intelligence and Other Technical Advancements
