Free Vascularized Medial Femoral Condyle Bone Graft for Scaphoid Nonunion with Poor Prognosis Factors
- Affiliations
-
- 1Department of Orthopedic Surgery, Yeungnam University Hospital, Yeungnam University College of Medicine, Daegu, Korea
- 2Department of Orthopedic Surgery, Seoul National University Bundang Hospital, Daegu, Korea
- KMID: 2516155
- DOI: http://doi.org/10.12790/ahm.20.0077
Abstract
- Purpose
Authors attempt to evaluate the clinical and radiographic results of the treatment of scaphoid nonunion with poor prognostic factors with the free vascularized medial femoral condyle bone graft.
Methods
We operated on eight patients with avascular necrosis or prolonged nonunion of the scaphoid between January 2016 and July 2019. Wrist motion in terms of flexion, extension, and ulnar and radial deviation, a visual analogue scale (VAS), the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire, the modified Mayo wrist score, scapholunate angle, and carpal height index were collected in the clinic setting preoperatively and at the latest follow-up in all patients
Results
Eight patients with union achieved correction and maintenance of both scapholunate angle and carpal height index. The VAS pain scores significantly improved from 5.1 preoperatively to 3.3 postoperatively. There was a statistically significant improvement in the average DASH score at the final follow-up. Scapholunate relationships in the reconstructed wrists remained almost unchanged, with average scapholunate angles of 49.7° before surgery and 47.0° at the latest postoperative follow-up. There was no statistical significance between the number of poor prognosis factors and the time to union, but there was a positive correlation.
Conclusion
It could help surgeons manage the scaphoid nonunion associated with poor prognostic factors such as avascular necrosis, carpal collapse (posttraumatic arthritis), prolonged nonunion, and failed prior scaphoid nonunion surgery.
Figure
-

Fig. 1. (A) Anterior (Russe) scaphoid exposure shows the nonunion site. When the nonunion site was exposed, an oval cortical window was made using a 3-mm diameter high-speed burr on the volar aspect of the proximal and distal pole of the scaphoid. (B) Intraoperative photos of debridement of the nonunion site at the scaphoid and preparation to accept the vascularized medial femoral condyle graft. (C) The graft was further shaped to fit the nonunion site. The periosteal surface attached to the pedicle should lie volar. (D) Vascular repairs were end-to-side to the radial artery and end-to-end to a vena comitans.
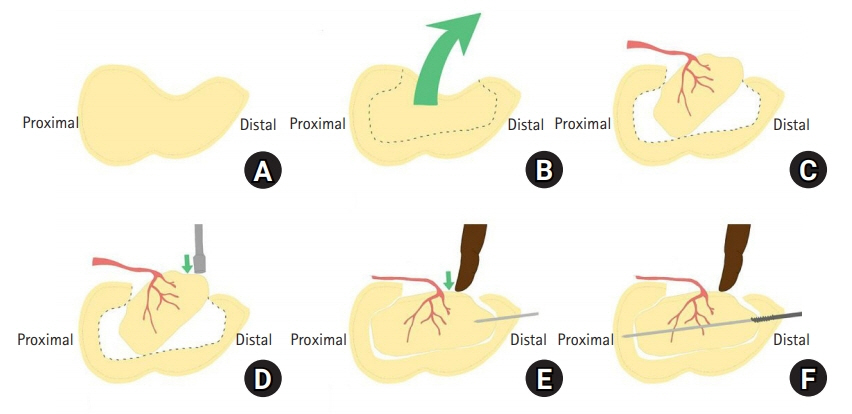
Fig. 2. (A) Lateral aspect of the scaphoid. (B) The surgeon excavated as much necrotic bone as possible if encountered while leaving the dorsal cortex intact. (C) The graft is inset obliquely into the scaphoid defect with the cortex facing palmarly. (D) Push the distal part of the graft with the impactor. (E) To fit graft properly without rotation or extrusion of graft and vessels, the surgeon holds the distal part of the graft with the index finger during temporary fixation with guide wire. (F) A 3.0-mm partially threaded headless compression screw was inserted along the guide wire and the guide wire was removed.

Fig. 3. (A) Preparation and harvesting of the medial femoral condyle graft. The vastus medialis fascia was incised sharply at its posterior aspect, and the muscle retracted properly exposing the medial genicular artery system. (B) A rectangular shape of sufficient size to fill the gap in the scaphoid is marked out, the periosteum sharply incised, and the bone cut with a micro sagittal saw and osteotomes. (C) The corticocancellous graft was harvested with its vascular pedicle.
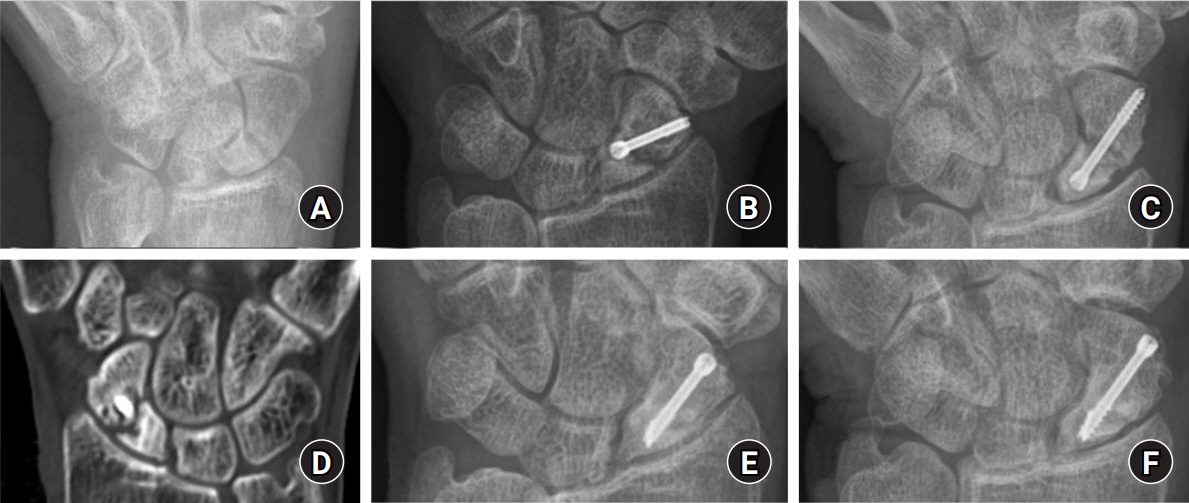
Fig. 4. (A) Scaphoid view of the wrist of a 51-year-old man, showing an scaphoid fracture. (B) Anteroposterior and (C) scaphoid view of wrist at 10 month after 1st operation in other hospital, showing an established scaphoid nonunion, sclerotic change around the fracture site. (D) Postoperative computed tomography at 10 month after 1st operation in other medical center, showing sclerotic change. (E) Anteroposterior and (F) scaphoid view of wrist 1-year after the last operation, showing achievement of union, correction, and maintenance of carpal height index.
Reference
-
1. Kakar S, Bishop AT, Shin AY. Role of vascularized bone grafts in the treatment of scaphoid nonunions associated with proximal pole avascular necrosis and carpal collapse. J Hand Surg Am. 2011; 36:722–5.
Article2. Guzzini M, Lanzetti RM, Proietti L, Lupariello D, Iorio R, Ferretti A. The role of vascularized flaps in the treatment of proximal pole avascular necrosis in scaphoid non-unions. Acta Biomed. 2019; 90(12-S):64–8.3. Gras M, Wahegaonkar AL, Mathoulin C. Treatment of avascular necrosis of the proximal pole of the scaphoid by arthroscopic resection and prosthetic semireplacement arthroplasty using the pyrocarbon Adaptive Proximal Scaphoid Implant (APSI): long-term functional outcomes. J Wrist Surg. 2012; 1:159–64.
Article4. Chaudhry T, Uppal L, Power D, Craigen M, Tan S. Scaphoid nonunion with poor prognostic factors: the role of the free medial femoral condyle vascularized bone graft. Hand (N Y). 2017; 12:135–9.5. Kim J, Park JW, Chung J, Jeong Bae K, Gong HS, Baek GH. Non-vascularized iliac bone grafting for scaphoid nonunion with avascular necrosis. J Hand Surg Eur Vol. 2018; 43:24–31.
Article6. Sgromolo NM, Rhee PC. The role of vascularized bone grafting in scaphoid nonunion. Hand Clin. 2019; 35:315–22.
Article7. Putnam JG, DiGiovanni RM, Mitchell SM, Castañeda P, Edwards SG. Plate fixation with cancellous graft for scaphoid nonunion with avascular necrosis. J Hand Surg Am. 2019; 44:339.
Article8. Merrell GA, Wolfe SW, Slade JF 3rd. Treatment of scaphoid nonunions: quantitative meta-analysis of the literature. J Hand Surg Am. 2002; 27:685–91.
Article9. Boyer MI. MFC bone graft for scaphoid nonunion, osteonecrosis, and failed prior surgery: three strikes but not necessarily out: commentary on an article by Nicholas Pulos, MD, et al.: “free vascularized medial femoral condyle bone graft after failed scaphoid nonunion surgery”. J Bone Joint Surg Am. 2018; 100:e111.10. Pulos N, Kollitz KM, Bishop AT, Shin AY. Free vascularized medial femoral condyle bone graft after failed scaphoid nonunion surgery. J Bone Joint Surg Am. 2018; 100:1379–86.
Article11. Dehghani M, Soltanmohamadi M, Tahririan MA, Moezi M, Daneshpajouhnejad P, Zarezadeh A. Management of scaphoid nonunion with avascular necrosis using 1,2 intercompartmental supraretinacular arterial bone graft. Adv Biomed Res. 2014; 3:185.
Article12. Bürger HK, Windhofer C, Gaggl AJ, Higgins JP. Vascularized medial femoral trochlea osteocartilaginous flap reconstruction of proximal pole scaphoid nonunions. J Hand Surg Am. 2013; 38:690–700.
Article13. Elgammal A, Lukas B. Vascularized medial femoral condyle graft for management of scaphoid non-union. J Hand Surg Eur Vol. 2015; 40:848–54.
Article14. Kazmers NH, Thibaudeau S, Levin LS. A scapholunate ligament-sparing technique utilizing the medial femoral condyle corticocancellous free flap to reconstruct scaphoid nonunions with proximal pole avascular necrosis. J Hand Surg Am. 2016; 41:e309–15.
Article15. Youm Y, McMurthy RY, Flatt AE, Gillespie TE. Kinematics of the wrist. I. An experimental study of radial-ulnar deviation and flexion-extension. J Bone Joint Surg Am. 1978; 60:423–31.
Article16. Jones DB Jr, Bürger H, Bishop AT, Shin AY. Treatment of scaphoid waist nonunions with an avascular proximal pole and carpal collapse: surgical technique. J Bone Joint Surg Am. 2009; 91 Suppl 2:169–83.17. Kollitz KM, Pulos N, Bishop AT, Shin AY. Primary medial femoral condyle vascularized bone graft for scaphoid nonunions with carpal collapse and proximal pole avascular necrosis. J Hand Surg Eur Vol. 2019; 44:600–6.
Article18. Doi K, Oda T, Soo-Heong T, Nanda V. Free vascularized bone graft for nonunion of the scaphoid. J Hand Surg Am. 2000; 25:507–19.
Article19. Aibinder WR, Wagner ER, Bishop AT, Shin AY. Bone grafting for scaphoid nonunions: is free vascularized bone grafting superior for scaphoid nonunion? Hand (N Y). 2019; 14:217–22.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Scaphoid Fractures and Nonunions
- The Effect of Smoking on the Outcomes of Vascularized Bone Graft Surgery in Scaphoid Nonunion through Meta-analysis
- Scaphoid Fractures and Nonunions: Recent Trends of Treatment
- Treatment of Scaphoid Nonunionusing a Pedicled Vascularized Bone Graft
- Treatment of Nonunion of Proximal Scaphoid Fractures Using Vascularized Bone Graft
