Cannulation of the Portal Vein during Endoscopic Retrograde Cholangiopancreatography in a Patient with Choledocholithiasis
- Affiliations
-
- 1Department of Internal Medicine, Presbyterian Medical Center, Jeonju, Korea
- KMID: 2516043
- DOI: http://doi.org/10.4166/kjg.2021.030
Abstract
- Cannulation of the portal vein is a rare complication of ERCP. This paper reports a case of portal vein catheterization during ERCP in a patient with choledocholithiasis. A 62-year-old man was admitted to the Presbyterian Medical Center with right upper quadrant pain and jaundice. ERCP was performed under the suspicion of obstructive jaundice caused by a radiolucent stone. Bile duct cannulation using a pull-type papillotome was attempted, but it failed. After needle-knife fistulotomy, wire-guided cannulation was performed successfully, and 10 mL contrast was injected. On the other hand, the fluoroscopy image showed that the contrast medium disappeared very quickly. Pure blood was collected when the catheter was aspirated to identify the bile reflux, indicating possible cannulation of the portal vein. The procedure was terminated immediately and abdominal computed tomography showed air in the portal vein. One day after, a follow-up CT scan showed no air in the portal vein. The patient underwent repeated ERCP, and the common bile duct was cannulated. In most cases, isolated portal vein cannulation does not result in severe morbidity. However, it is important to aware of this rare complication so that no further invasive procedure is performed on the patient.
Keyword
Figure
-

Fig. 1 (A) Endoscopic image showing papillary orifice covered by hooding fold. (B) Endoscopic image of major papilla before needle-knife fistulotomy. There was no damage or deformation of the papilla while trying to cannulate the bile duct. (C) Endoscopic image of major papilla after needle-knife fistulotomy. Using a needle-knife, an incision was started at the most protruding part of the infundibulum, and an incision was made about 3mm in the direction of the papillary orifice.

Fig. 2 After wire-guided cannulation, we injected 10 mL contrast through the papillotome but the fluoroscopy image showed that the contrast medium disappeared very quickly.

Fig. 3 Aspiration was performed in order to identify the bile reflux, but pure blood was collected indicating possible cannulation of the portal vein.
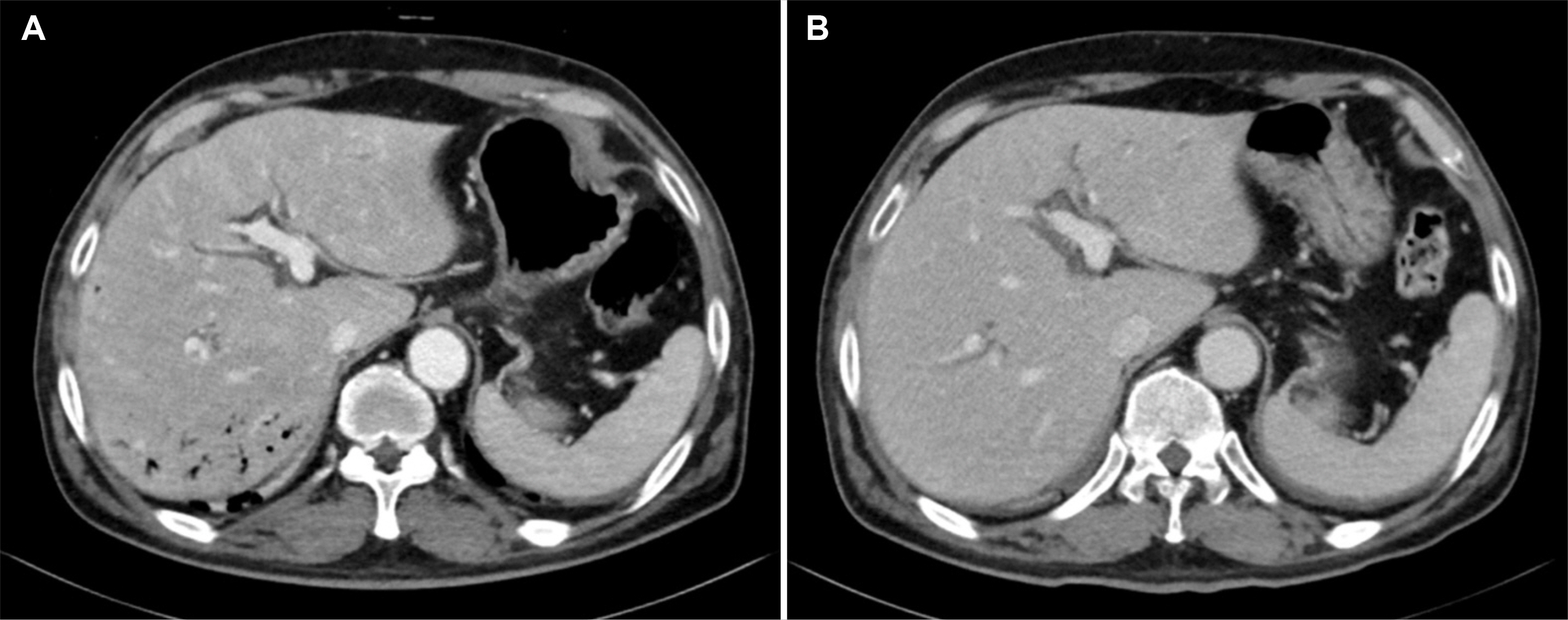
Fig. 4 (A) Abdominal computed tomography (CT) scan obtained immediately after endoscopic retrograde cholangiopancreatography showed air in the portal vein. (B) One day after, follow up CT scan presented no air in the portal vein.
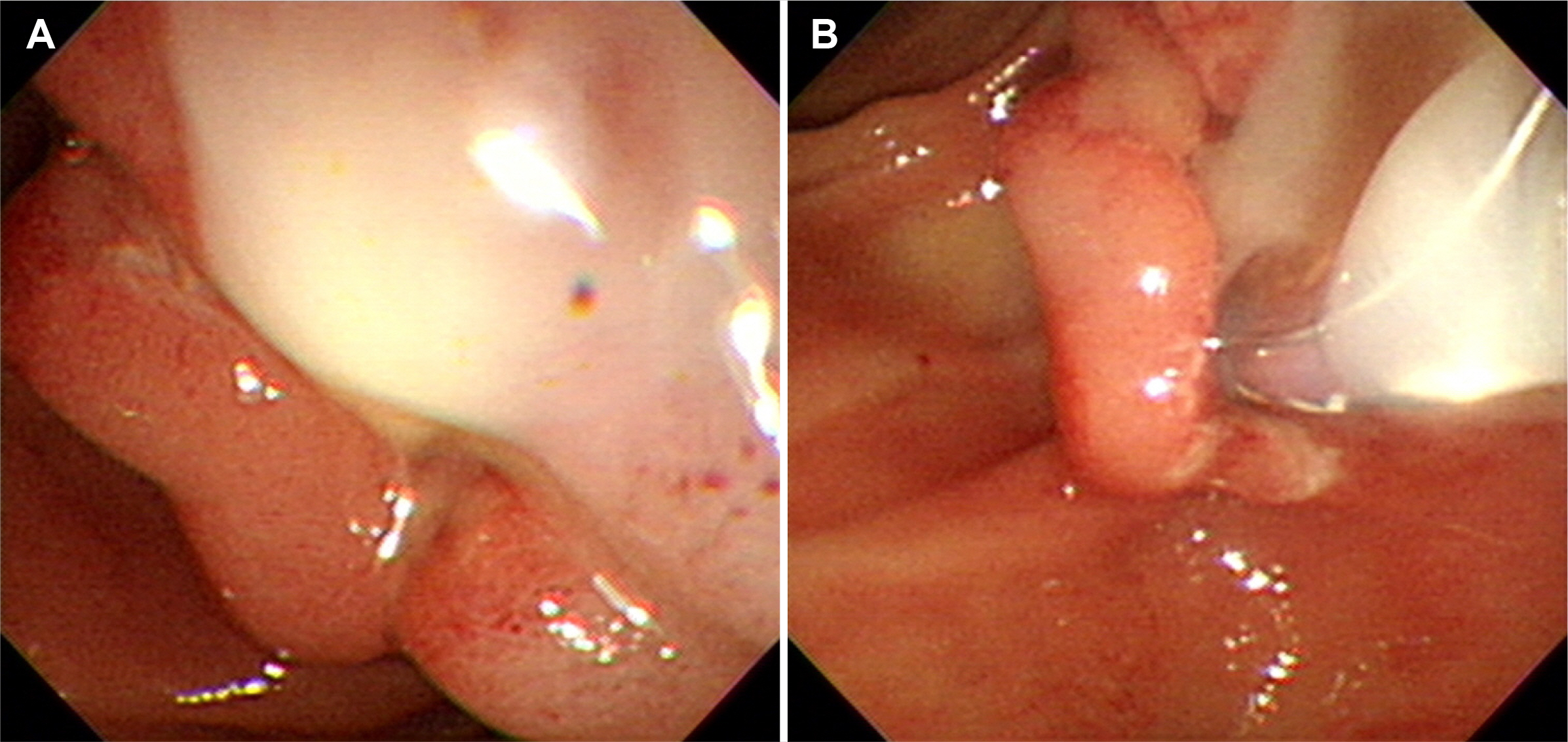
Fig. 5 (A) Endoscopic image showing the pus was oozing from the site where the fistulotomy was performed. (B) Guide wire was inserted into the opening where the pus was drained, and then a papillotome was advanced over the guide wire.
Reference
-
1. Espinel J, Pinedo ME, Calleja JL. 2007; Portal vein filling: an unusual complication of needle-knife sphincterotomy. Endoscopy. 39 Suppl 1:E245. DOI: 10.1055/s-2007-966156. PMID: 17957642.
Article2. Furuzono M, Hirata N, Saitou J, Nakaji S. 2009; A rare complication during ERCP and sphincterotomy: placement of an endoscopic nasobiliary drainage tube in the portal vein. Gastrointest Endosc. 70:588–590. DOI: 10.1016/j.gie.2008.12.255. PMID: 19555937.
Article3. Huibregtse K, Gish R, Tytgat GN. 1988; A frightening event during endoscopic papillotomy. Gastrointest Endosc. 34:67–68. DOI: 10.1016/S0016-5107(88)71239-0.
Article4. Ricci E, Mortilla MG, Conigliaro R, Bertoni G, Bedogni G, Chilovi F. 1992; Portal vein filling: a rare complication associated with ERCP for endoscopic biliary stent placement. Gastrointest Endosc. 38:524–525. DOI: 10.1016/S0016-5107(92)70503-3.
Article5. Kim CL, Ha Y, Om SY, et al. 2014; Portal vein cannulation during endoscopic retrograde cholangiopancreatography. Korean J Med. 86:462–465. DOI: 10.3904/kjm.2014.86.4.462.
Article6. Kalaitzakis E, Stern N, Sturgess R. 2011; Portal vein cannulation: an uncommon complication of endoscopic retrograde cholangiopancreatography. World J Gastroenterol. 17:5131–5132. DOI: 10.3748/wjg.v17.i46.5131. PMID: 22171149. PMCID: PMC3235598.
Article7. Kawakami H, Kuwatani M, Kudo T, Ehira N, Yamato H, Asaka M. 2011; Portobiliary fistula: unusual complication of wire-guided cannulation during endoscopic retrograde cholangiopancreatography. Endoscopy. 43 Suppl 2 UCTN:E98–E99. DOI: 10.1055/s-0030-1256150. PMID: 21425030.
Article8. Lum C, Cho KC, Scholl DG, Sundaram NK. 1998; Portal vein opacification during ERCP in patients with pancreatitis. Abdom Imaging. 23:81–83. DOI: 10.1007/s002619900290. PMID: 9437069.
Article9. Kennedy C, Larvin M, Linsell J. 1997; Fatal hepatic air embolism following ERCP. Gastrointest Endosc. 45:187–188. DOI: 10.1016/S0016-5107(97)70246-3.
Article10. Barbeiro S, Atalaia-Martins C, Gon?alves C, Cotrim I. 2017; Portal air embolism after endoscopic retrograde cholangiopancreatography. Rev Esp Enferm Dig. 109:452–453. DOI: 10.17235/reed.2017.4771/2016.11. Finsterer J, Stöllberger C, Bastovansky A. 2010; Cardiac and cerebral air embolism from endoscopic retrograde cholangio-pancreatography. Eur J Gastroenterol Hepatol. 22:1157–1162. DOI: 10.1097/MEG.0b013e32833c5459. PMID: 20555267.
Article12. So H, Song TJ, Lee D, et al. 2015; Endoscopic treatment of recurrent bleeding from a portobiliary fistula with a fully covered self-expandable metal stent. Endoscopy. 47 Suppl 1:E616–E617. DOI: 10.1055/s-0035-1569656. PMID: 26714149.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Portal Vein Cannulation During Endoscopic Retrograde Cholangiopancreatography
- Can Endoscopic Ultrasonography Prevent Unnecessary Endoscopic Retrograde Cholangiopancreatography in Patients with High and Intermediate Likelihood of Choledocholithiasis?
- The Usefulness of Cap-assisted Endoscopic Retrograde Cholangiopancreatography for Cannulation Complicated by a Periampullary Diverticulum
- Cholelithiasis Fortunately Removed by Endoscopic Retrograde Cholangiopancreatography
- Prevention of Post-endoscopic Retrograde Cholangiopancreatography Pancreatitis: An Endoscopic Perspective
