Revised Korean Antiviral Guideline Reduces the Hepatitis B-related Hepatocellular Carcinoma Risk in Cirrhotic Patients
- Kim DS
 1
1 - Park SY2
- Kim BK1,3
- Park JY1,3
- Kim DY1,3
- Han KH1,3
- Lee YR2
- Tak WY2
- Kweon YO2
- Jung I4
- Han M5
- Kim EH5
- Ahn SH1,3
- Kim SU1,3
- Affiliations
-
- 1Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea
- 2Department of Internal Medicine, Kyungpook National University Hospital, Daegu, Korea
- 3Yonsei Liver Center, Severance Hospital, Seoul, Korea
- 4Division of Biostatistics, Department of Biomedical Systems Informatics, Yonsei University College of Medicine, Seoul, Korea
- 5Biostatistics Collaboration Unit, Department of Biomedical Systems Informatics, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2515086
- DOI: http://doi.org/10.3346/jkms.2021.36.e105
Abstract
- Background
Since September 2015, the initiation of antiviral therapy (AVT) for patients with chronic hepatitis B (CHB)-related cirrhosis has been reimbursed according to the revised Korean Association for the Study of Liver (KASL) guideline, if the patient had hepatitis B virus DNA level ≥ 2,000 IU/L, regardless of aminotransferase or alanine aminotransferase levels. This study investigated whether the KASL guideline implementation reduced the risk of CHB-related hepatocellular carcinoma (HCC) in patients with cirrhosis in South Korea.
Methods
A total of 429 patients with CHB-related cirrhosis who initiated AVT between 2014 and 2016 were recruited. The risk of HCC development was compared between patients who initiated AVT before and after September 2015 (pre-guideline [n = 196, 45.7%] vs. postguideline implementation [n = 233, 54.3%]).
Results
Univariate analysis showed that AVT initiation before guideline implementation, older age, male gender, and diabetes significantly predicted increased risk of HCC development (all P < 0.05). Subsequent multivariate analysis showed that AVT initiation before guideline implementation (HR = 1.941), older age (HR = 5.762), male gender (HR = 2.555), and diabetes (HR = 1.568) independently predicted increased risk of HCC development (all P < 0.05). Additionally, multivariate analysis showed that AVT initiation before guideline implementation (HR = 2.309), male gender (HR = 3.058), and lower platelet count (HR = 0.989) independently predicted mortality (P < 0.05). The cumulative incidences of HCC and mortality were significantly higher in patients who initiated AVT before guideline implementation than in those who initiated AVT after guideline implementation (all P < 0.05, log-rank test).
Conclusion
The prognosis of patients with CHB-related cirrhosis who initiated AVT improved after guideline implementation according to the revised KASL guideline.
Figure
-
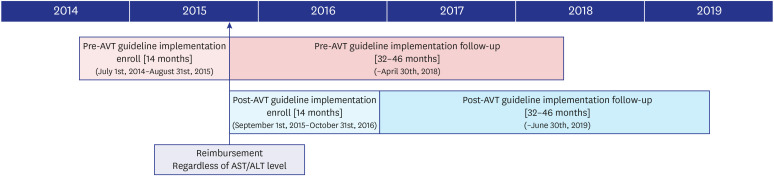
Fig. 1 Diagram of cohort enrollment and follow-up period. Patients were enrolled based on AVT start date. The pre- and post-guideline implementation cohort was separated in September 1st, 2015, which is the start date for National Health Insurance Service medical insurance reimbursement for cirrhotic chronic hepatitis B patients with HBV DNA > 2,000 IU/mL, regardless of AST/ALT levels. The enrollment period for the pre-guideline implementation cohort was from July 1st, 2014 to August 31st, 2015 and the post guideline implementation cohort was from September 1st, 2015 to October 31st, 2016 (both 14 months). Follow up periods were matched for both cohorts to a maximum of 45 months, until April 30th, 2018 and June 30th, 2019 for the previous and current AVT guideline cohort, respectively.AVT = antiviral therapy, AST = aspartate aminotransferase, ALT = alanine aminotransferase, HBV = Hepatitis B virus.
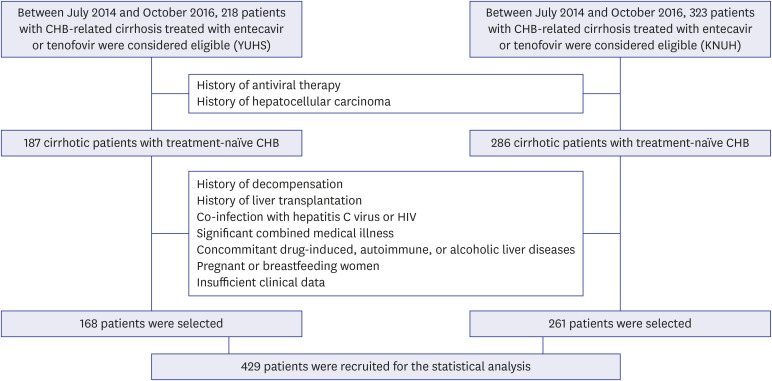
Fig. 2 Flow of study population selection process. A total of 218 patients from YUHS and 323 patients from KNUH with CHB treated with entecavir or tenofovir between July 2014 and October 2016 were considered eligible for participation. After exclusion of 50 and 37 patients from YUHS and KNUH, respectively, according to our exclusion criteria, 168 patients from YUHS and 261 patients from KNUH were ultimately included for statistical analysis.YUHS = Yonsei University Health System, KNUH = Kyungpook National University Hospital, CHB = chronic hepatitis B, HIV = human immunodeficiency virus.
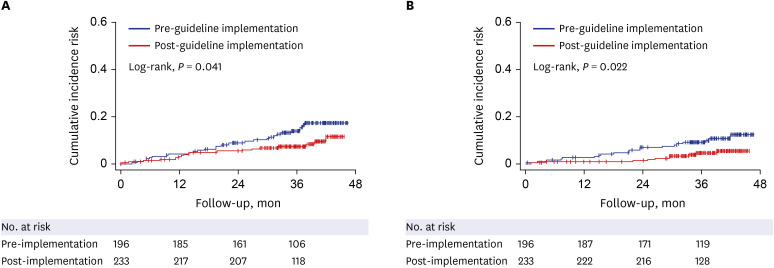
Fig. 3 The cumulative incidence rates of HCC (A) and mortality or transplantation (B) according to antiviral therapy guideline implementation. The cumulative incidence risk of HCC and mortality or transplantation of patients in the pre-guideline implementation cohort was significantly higher than that of patients in the post-guideline implementation cohort (P = 0.041 and P = 0.022 respectively, log-rank test).HCC = hepatocellular carcinoma.
Reference
-
1. World Health Organization. Hepatitis B vaccines: WHO position paper, July 2017 - recommendations. Vaccine. 2019; 37(2):223–225. PMID: 28743487.2. Kim DS, Lim TS, Jeon MY, Kim BK, Park JY, Kim DY, et al. Transarterial chemoembolization in treatment-naïve and recurrent hepatocellular carcinoma: a propensity-matched outcome analysis. Dig Dis Sci. 2019; 64(12):3660–3668. PMID: 31187326.
Article3. Ikeda K, Saitoh S, Suzuki Y, Kobayashi M, Tsubota A, Koida I, et al. Disease progression and hepatocellular carcinogenesis in patients with chronic viral hepatitis: a prospective observation of 2215 patients. J Hepatol. 1998; 28(6):930–938. PMID: 9672166.
Article4. Sookoian S, Pirola CJ. Genetic predisposition in nonalcoholic fatty liver disease. Clin Mol Hepatol. 2017; 23(1):1–12. PMID: 28268262.
Article5. Lai CL, Gane E, Liaw YF, Hsu CW, Thongsawat S, Wang Y, Globe Study Group, et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med. 2007; 357(25):2576–2588. PMID: 18094378.
Article6. Park MS, Kim BK, Kim KS, Kim JK, Kim SU, Park JY, et al. Antiviral efficacies of currently available rescue therapies for multidrug-resistant chronic hepatitis B. Clin Mol Hepatol. 2013; 19(1):29–35. PMID: 23593607.
Article7. Kim DS, Jeon MY, Lee HW, Kim BK, Park JY, Kim DY, et al. Influence of hepatic steatosis on the outcomes of patients with chronic hepatitis B treated with entecavir and tenofovir. Clin Mol Hepatol. 2019; 25(3):283–293. PMID: 30419649.
Article8. Kim SU, Seo YS, Lee HA, Kim MN, Lee YR, Lee HW, et al. A multicenter study of entecavir vs. tenofovir on prognosis of treatment-naïve chronic hepatitis B in South Korea. J Hepatol. 2019; 71(3):456–464. PMID: 30959156.
Article9. Liang LY, Wong GL. Unmet need in chronic hepatitis B management. Clin Mol Hepatol. 2019; 25(2):172–180. PMID: 30754963.
Article10. Yim HJ, Kim JH, Park JY, Yoon EL, Park H, Kwon JH, et al. Comparison of clinical practice guidelines for the management of chronic hepatitis B: when to start, when to change, and when to stop. Clin Mol Hepatol. 2020; 26(4):411–429. PMID: 32854458.
Article11. McMahon BJ, Bulkow L, Simons B, Zhang Y, Negus S, Homan C, et al. Relationship between level of hepatitis B virus DNA and liver disease: a population-based study of hepatitis B e antigen-negative persons with hepatitis B. Clin Gastroenterol Hepatol. 2014; 12(4):701–706.e1-3. PMID: 24035774.
Article12. Korean Association for the Study of the Liver. Management of chronic hepatitis B. Clin Mol Hepatol. 2012; 18(2):109–162. PMID: 22893865.13. Cristina SJ, Marta CM, Mercedes GS, Almudena PM, Álvaro HM, Luis VS, et al. Characterization and evaluation of liver fibrosis grade in patients with chronic hepatitis B virus infection and normal transaminases. Clin Mol Hepatol. 2018; 24(4):384–391. PMID: 29969885.
Article14. Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology. 2007; 45(2):507–539. PMID: 17256718.
Article15. Liaw YF, Leung N, Kao JH, Piratvisuth T, Gane E, Han KH, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int. 2008; 2(3):263–283. PMID: 19669255.
Article16. Wong GL. Management of chronic hepatitis B patients in immunetolerant phase: what latest guidelines recommend. Clin Mol Hepatol. 2018; 24(2):108–113. PMID: 29353469.
Article17. Lee S, Kim BK, Kim SU, Park SY, Kim JK, Lee HW, et al. Clinical outcomes and prognostic factors of patients with advanced hepatocellular carcinoma treated with sorafenib as first-line therapy: a Korean multicenter study. J Gastroenterol Hepatol. 2014; 29(7):1463–1469. PMID: 25273508.
Article18. Betensky RA. Measures of follow-up in time-to-event studies: why provide them and what should they be? Clin Trials. 2015; 12(4):403–408. PMID: 26025565.
Article19. Lai M, Hyatt BJ, Nasser I, Curry M, Afdhal NH. The clinical significance of persistently normal ALT in chronic hepatitis B infection. J Hepatol. 2007; 47(6):760–767. PMID: 17928090.
Article20. Kumar M, Sarin SK, Hissar S, Pande C, Sakhuja P, Sharma BC, et al. Virologic and histologic features of chronic hepatitis B virus-infected asymptomatic patients with persistently normal ALT. Gastroenterology. 2008; 134(5):1376–1384. PMID: 18471514.
Article21. Casado JL. Renal and bone toxicity with the use of tenofovir: understanding at the end. AIDS Rev. 2016; 18(2):59–68. PMID: 27230467.22. Cho H, Cho Y, Cho EJ, Lee JH, Yu SJ, Oh KH, et al. Tenofovir-associated nephrotoxicity in patients with chronic hepatitis B: two cases. Clin Mol Hepatol. 2016; 22(2):286–291. PMID: 27377911.
Article23. Lee SW, Kwon JH, Lee HL, Yoo SH, Nam HC, Sung PS, et al. Comparison of tenofovir and entecavir on the risk of hepatocellular carcinoma and mortality in treatment-naïve patients with chronic hepatitis B in Korea: a large-scale, propensity score analysis. Gut. 2020; 69(7):1301–1308. PMID: 31672838.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Antiviral therapy in chronic hepatitis B: Revised national medical insurance imbursement policy
- Development and surveillance of hepatocellular carcinoma in patients with sustained virologic response after antiviral therapy for chronic hepatitis C
- Who Needs Screening for the Early Detection of Hepatocellular Carcinoma ?
- Long Term Efficacy of Antiviral Therapy: Mortality and Incidence of Hepatocellular Carcinoma
- Treatment of Hepatitis C in Special Conditions: Liver Cirrhosis
