Delayed cranial nerve palsy after successful coil embolization in cavernous sinus lesion
- Affiliations
-
- 1Department of Neurosurgery, Yeungnam University Medical Center and College of Medicine, Daegu, Korea
- KMID: 2514336
- DOI: http://doi.org/10.7461/jcen.2021.E2020.06.002
Abstract
- Cavernous sinus (CS) lesion is hard to access by surgical approach. With the development of endovascular technique, neurointerventional therapy is an alternative modality for CS lesions. This endovascular technique has been widely used for the past decade, avoiding the risks associated with surgical treatment. However, complications can still arise from coil embolization. Although immediate complication associate with embolic event or mass effect has been well described, but delayed (>1 year from treatment) nerve palsy after coil embolization is rare. We report two cases of delayed cranial nerve palsy after successful endovascular coil embolization in CS lesion.
Figure
-

Fig. 1. Case 1, A 61-year-old woman with delayed incomplete Horner’s syndrome beginning 19 months following coiling of a left ICA aneurysm. (A, B) Preoperative angiography demonstrated the incidental unruptured aneurysm of the left cavernous ICA. (C, D) In postoperative angiography, complete coiling was checked. (E, F) After 19 months, follow-up angiography was done and there was no interval change on coiling site. ICA, internal carotid artery.
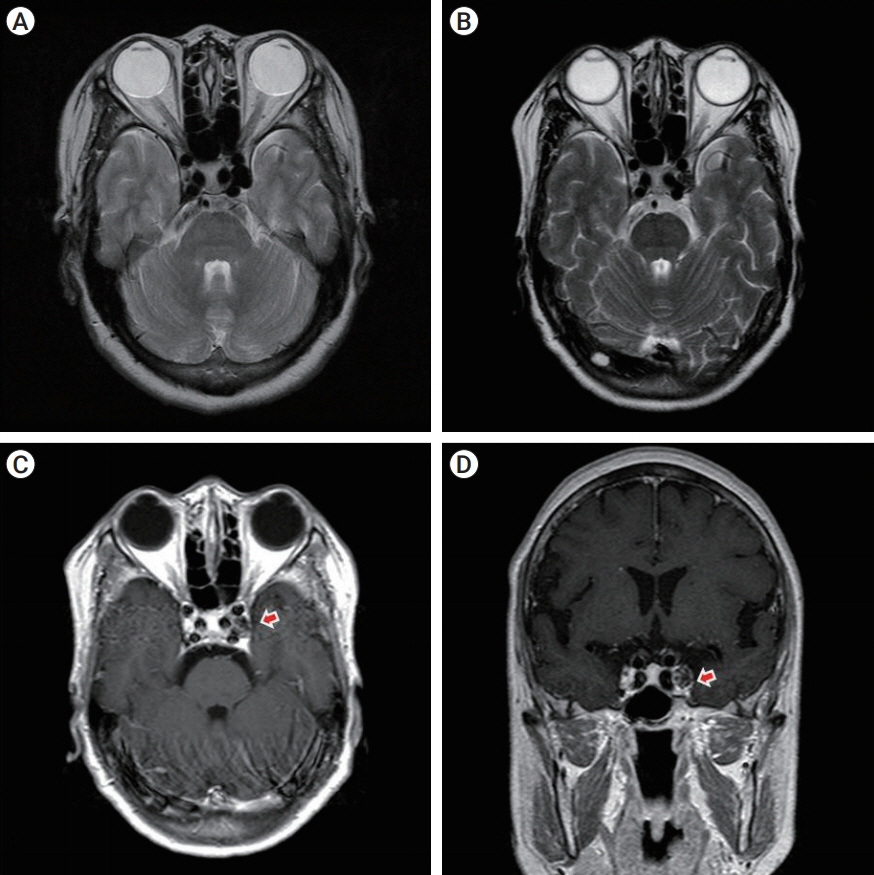
Fig. 2. Case 1, (A) Preoperative T2-weighted axial MRI reveals an aneurysm arising from the cavernous portion of the left ICA. (B) 19 months later, postoperative T2-weighted axial MRI shows heterogeneous signal intensity from within the aneurysm, consistent with coil packing. (C, D) Postoperative T1-weighted axial MRI shows discontinuity of left CS outer wall (arrow). MRI, magnetic resonance imaging; ICA, internal carotid artery; CS, cavernous sinus.
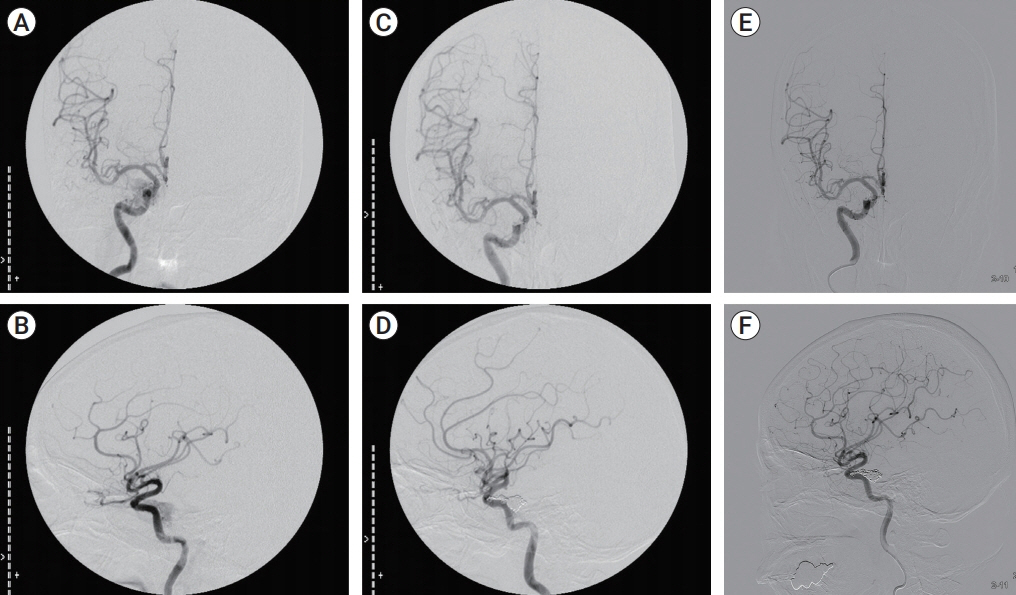
Fig. 3. Case 2, A 50-year-old woman with delayed right 6th nerve palsy beginning 38 months after coil embolization of CCF. (A, B) Preoperative angiography was done and dural type CCF. (C, D) In postoperative angiography, CCF and shunting flow was not checked. (E, F) After 38 months, follow-up angiography was done and there was no interval change on coiling site. CCF, carotid cavernous fistula.
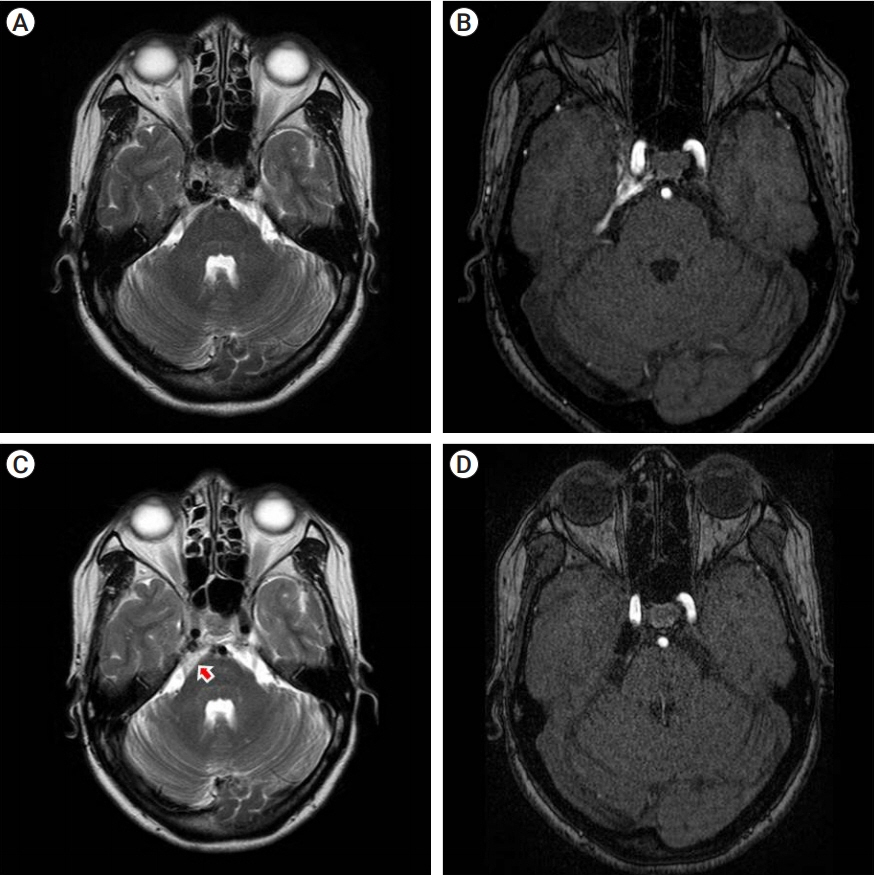
Fig. 4. (A) Preoperative T2-weighted axial MRI shows the signal voiding on right CS. (B) preoperative MR source image shows abnormal signal flow on the right CS. (C) 38 months later, postoperative T2-weighted axial MRI shows some mixed signal intensity lesion suggesting inflammatory reaction or thrombosis (arrow) around CS and prepontine/superior cerebellopontine cistern. (D) Postoperative MR source image reveals complete obliteration of CCF. MRI, magnetic resonance imaging; CS, cavernous sinus; CCF, carotid cavernous fistula.
Reference
-
1. Bocher-Schwarz HG, Ringel K, Bohl J, Filippi R, Kempski O, Perneczky A. Histological findings in coil-packed experimental aneurysms 3 months after embolization. Neurosurgery. 2002; Feb. 50(2):379–84. discussion 384-5.
Article2. Bou Ghannam A, Subramanian PS. Delayed onset cranial nerve palsies after endovascular coil embolization of direct carotid-cavernous fistulas. J Neuroophthalmol. 2018; Jun. 38(2):156–9.
Article3. Brilstra EH, Rinkel GJ, van der Graaf Y, van Rooij WJ, Algra A. Treatment of intracranial aneurysms by embolization with coils: a systematic review. Stroke. 1999; Feb. 30(2):470–6.4. Derdeyn CP, Cross DT 3rd, Moran CJ, Brown GW, Pilgram TK, Diringer MN, et al. Postprocedure ischemic events after treatment of intracranial aneurysms with Guglielmi detachable coils. J Neurosurg. 2002; May. 96(5):837–43.
Article5. Kashiwazaki D, Kuwayama N, Akioka N, Kuroda S. Delayed abducens nerve palsy after transvenous coil embolization for cavernous sinus dural arteriovenous fistulae. Acta Neurochir (Wien). 2014; Jan. 156(1):97–101.
Article6. Kim DJ, Kim DI, Suh SH, Kim J, Lee SK, Kim EY, et al. Results of transvenous embolization of cavernous dural arteriovenous fistula: a single-center experience with emphasis on complications and management. AJNR Am J Neuroradiol. 2006; Nov-Dec. 27(10):2078–82.7. Klisch J, Huppertz HJ, Spetzger U, Hetzel A, Seeger W, Schumacher M. Transvenous treatment of carotid cavernous and dural arteriovenous fistulae: results for 31 patients and review of the literature. Neurosurgery. 2003; Oct. 53(4):836–56. discussion 856-7.
Article8. Nishino K, Ito Y, Hasegawa H, Kikuchi B, Shimbo J, Kitazawa K, et al. Cranial nerve palsy following transvenous embolization for a cavernous sinus dural arteriovenous fistula: association with the volume and location of detachable coils. J Neurosurg. 2008; Aug. 109(2):208–14.
Article9. Schmidt GW, Oster SF, Golnik KC, Tumialan LM, Biousse V, Turbin R, et al. Isolated progressive visual loss after coiling of paraclinoid aneurysms. AJNR Am J Neuroradiol. 2007; NovDec. 28(10):1882–9.
Article10. Turner RD, Byrne JV, Kelly ME, Mitsos AP, Gonugunta V, Lalloo S, et al. Delayed visual deficits and monocular blindness after endovascular treatment of large and giant paraophthalmic aneurysms. Neurosurgery. 2008; Sep. 63(3):469–74. discussion 474-5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reversible Abducens Nerve Palsy Following Transvenous Embolization of Cavernous Sinus Dural Arteriovenous Fistula
- Coil Embolization Via a Superior Ophthalmic Vein Approach of Carotid Cavernous Sinus Fistula
- Isolated Sphenoid Sinus Mucocele Presenting as Third Nerve Palsy
- Isolated Oculomotor Nerve Palsy Caused by Cavernous Sinus Dural Arteriovenous Fistula: Case Report
- Arachnoid Cyst in Cavernous Sinus: Case Report
