Malignant rhabdoid tumor of the kidney in an adult with loss of INI1 expression and mutation in the SMARCB1 gene
- Affiliations
-
- 1Departments of Pathology, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea
- 2Departments of Urology, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea
- KMID: 2513901
- DOI: http://doi.org/10.4132/jptm.2021.01.26
Abstract
- A 57-year-old man with left flank pain was referred to our institute. Computed tomography scans revealed two enhancing masses in the left kidney. The clinical diagnosis was renal cell carcinoma (RCC). He underwent a radical nephrectomy with an adrenalectomy. Two well-circumscribed solid masses in the hilum and the lower pole (4.5 × 3.5 cm and 7.0 × 4.1 cm) were present. Poorly cohesive uniform round to polygonal epithelioid cells making solid sheets accounted for most of the tumor area. The initial diagnosis was RCC, undifferentiated with rhabdoid features. As the tumor showed loss of INI1 expression and a mutation in the SMARCB1 gene on chromosome 22, the revised diagnosis was a malignant rhabdoid tumor (MRT) of the kidney. To date, only a few cases of renal MRT in adults have been reported. To the best of our knowledge, this is the first report of MRT in the native kidney of an adult demonstrating a SMARCB1 gene mutation, a hallmark of MRT.
Keyword
Figure
-
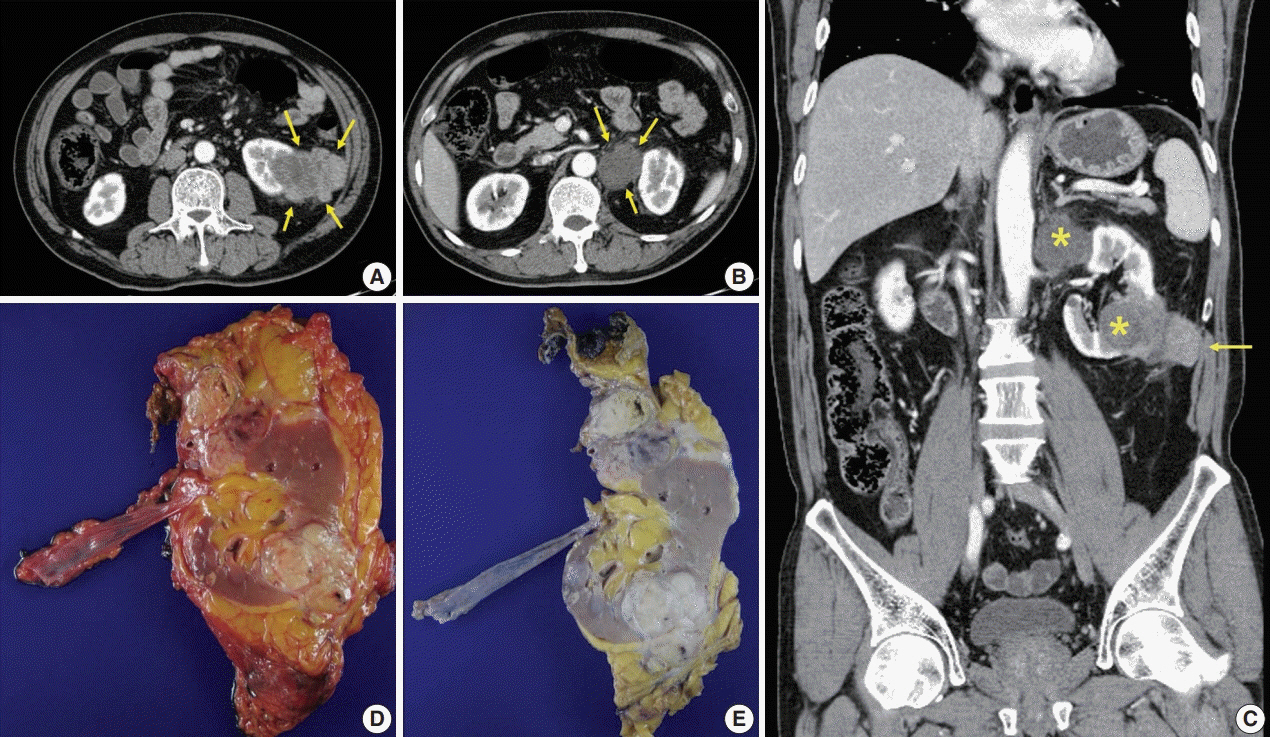
Fig. 1. Radiologic and gross features of the tumor. (A) Axial abdominopelvic computed tomography (CT) scan showing a 6.5-cm-sized heterogeneously enhancing exophytic and lobulated mass (arrows) in the lower pole of the left kidney. Mild fat infiltration is seen around the mass, and invasion of the Gerota’s fascia is present. (B) Axial CT scan showing a 3.5-cm-sized mass (arrows) with homogeneously low density in the superior aspect of the left renal hilum. As the tumor compressed the kidney from the exterior, it was interpreted as a necrotic lymph node. (C) Coronally reformatted images of CT showing both masses (asterisks). The lower pole mass invaded the abdominal wall (arrow). (D, E) Surgical specimen before (D) and after (E) fixation. The kidney bore two well-circumscribed solid masses in the hilum near the upper pole and in the lower pole, measuring 4.5×3.5 cm and 7.0×4.1 cm, respectively. They were homogeneously yellowish-gray in color and firm with focal areas of hemorrhage and necrosis.
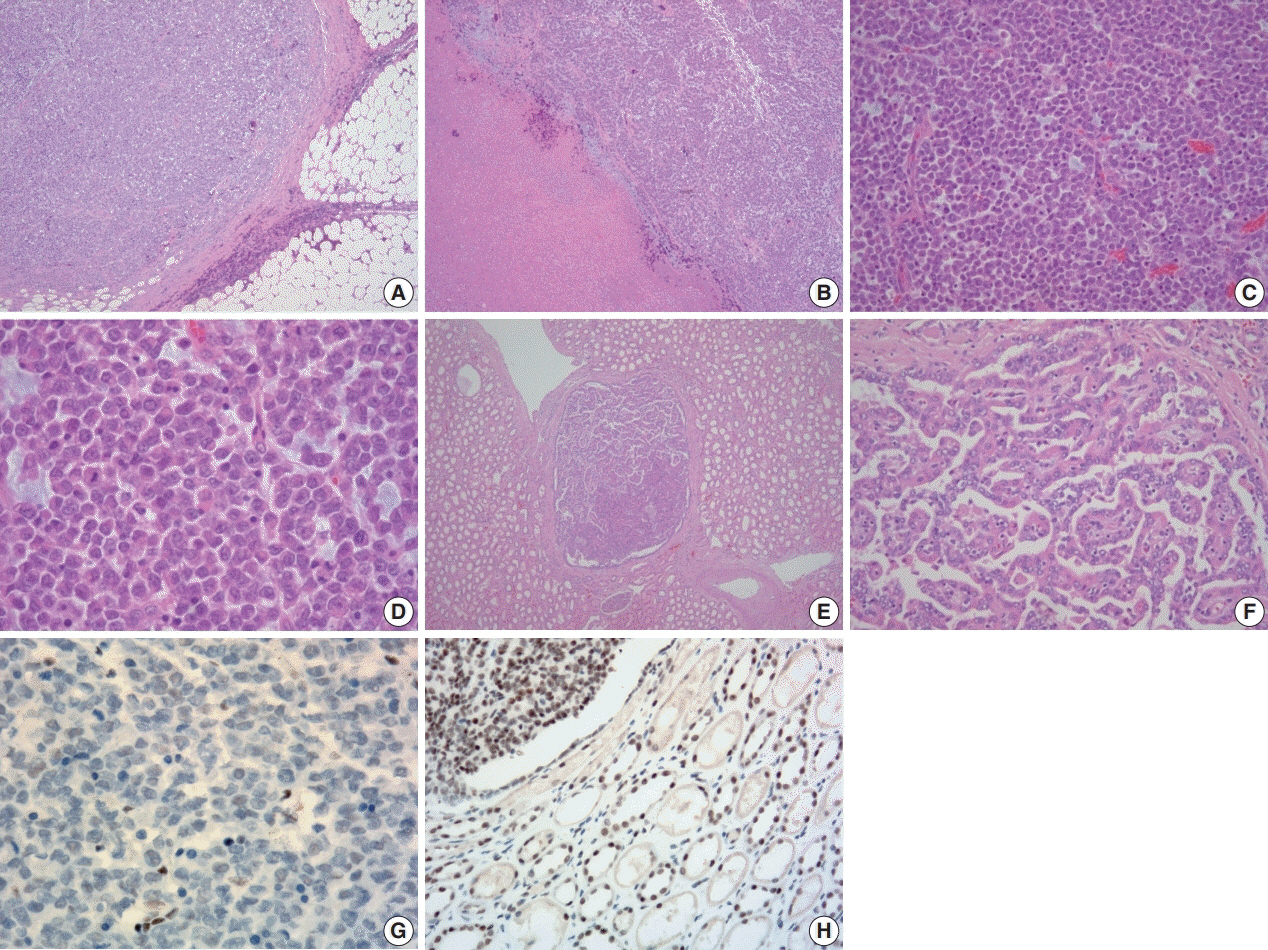
Fig. 2. Histologic and immunohistochemical features of the tumor. (A) Microscopically, the tumor was relatively well-defined and separated by dense fibrous tissue at most interfaces. (B) Areas of necrosis were present. (C) The tumor was composed almost entirely of solid sheets of tumor cells. (D) High power view revealing poorly cohesive uniform round to polygonal epithelioid cells. They had abundant densely eosinophilic cytoplasm with occasional round eosinophilic inclusion and large eccentric nuclei with irregular borders. Nucleoli were prominent. (E, F) Multiple small round nodules with papillary architecture were observed irrespective of the main mass. They were positive for cytokeratin 7 (not shown) and interpreted as papillary adenoma. (G) Tumor cells showing loss of immunoreactivity for integrase interactor 1 (INI-1; 1:100 dilution). (H) Retained immunoreactivity for INI-1 is shown in the normal renal tubular epithelium and papillary area (upper left) (1:100 dilution).
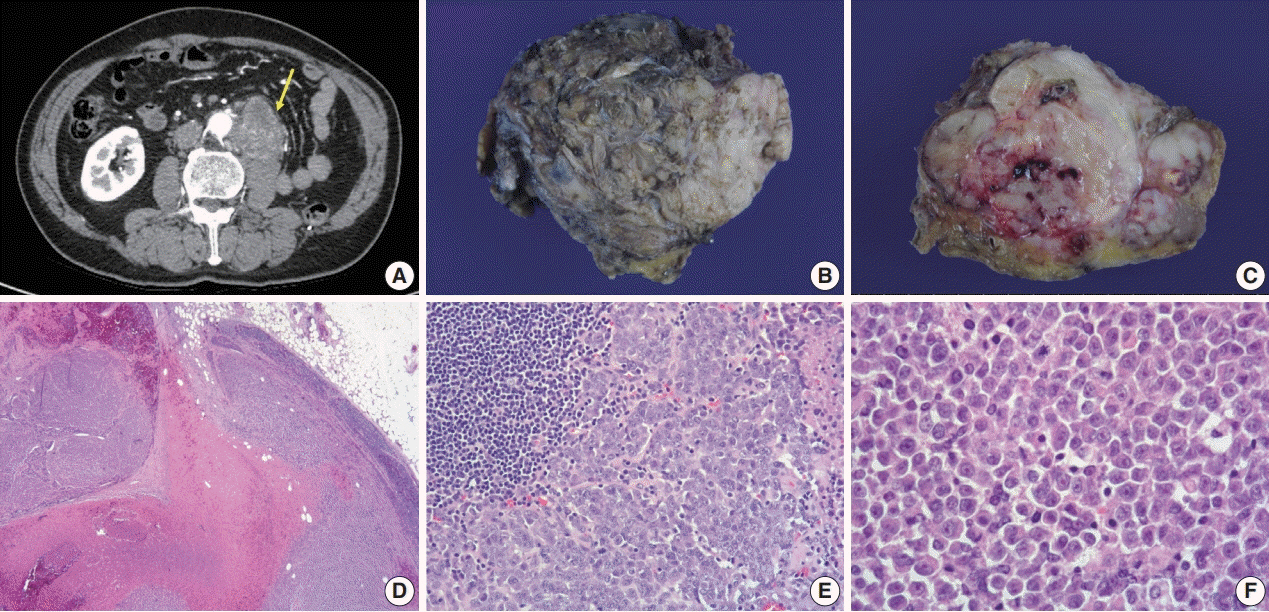
Fig. 3. Radiologic, gross, and histologic features of the newly-developed mass. (A) Follow-up axial abdominopelvic computed tomography scan a year after the surgery, revealing a newly visible 6.5-cm-sized heterogeneous enhancing lobulated mass (arrow) in the anterior aspect of the left psoas muscle underlying the left nephrectomy site, extending to the posterior aspect of the infrarenal abdominal aorta. Thus, aortic invasion was suspected. It was considered a recurrent tumor in the lymph nodes. (B) The specimen sent for examination was a conglomeration of lymph nodes (7.5×6×3.5 cm). (C) Whitish-tan solid and firm cut surfaces with areas of focal necrosis and hemorrhage were seen. (D) Solid sheets of tumor cells diffusely effacing lymph nodes and area of necrosis were seen. (E) Lymphoid tissue (upper left) and poorly cohesive round to polygonal tumor cells are shown. (F) Tumor cells had eosinophilic cytoplasm with occasional round eosinophilic inclusion and large eccentric nuclei with prominent nucleoli, resembling the former tumor from the kidney.
Reference
-
References
1. Schmidt D, Harms D, Zieger G. Malignant rhabdoid tumor of the kidney. Histopathology, ultrastructure and comments on differential diagnosis. Virchows Arch A Pathol Anat Histopathol. 1982; 398:101–8.
Article2. Lowe W, Weiss RM, Todd MB, True LD. Malignant rhabdoid tumor of the kidney in an adult. J Urol. 1990; 143:110–1.
Article3. Clausen HV, Horn T, Anagnostaki L, Larsen S. Malignant rhabdoid tumour of the kidney in an adult: a case report with immunohistochemical and ultrastructural investigation. Scand J Urol Nephrol Suppl. 1994; 157:123–8.4. Ebbinghaus SW, Herrera G, Marshall ME. Rhabdoid tumor of the kidney in an adult: review of the literature and report of a case responding to interleukin-2. Cancer Biother. 1995; 10:237–41.
Article5. Peng HQ, Stanek AE, Teichberg S, Shepard B, Kahn E. Malignant rhabdoid tumor of the kidney in an adult: a case report and review of the literature. Arch Pathol Lab Med. 2003; 127:e371–3.
Article6. Zhao G, Na R, Yang Y, Han R. Pure malignant rhabdoid tumor of the left kidney in an adult: a case report and review of the literature. Oncol Lett. 2013; 5:1481–4.
Article7. Podduturi V, Campa-Thompson MM, Zhou XJ, Guileyardo JM. Malignant rhabdoid tumor of the kidney arising in an adult patient. Proc (Bayl Univ Med Cent). 2014; 27:239–41.
Article8. Okumura Y, Adachi Y, Shirahase T, et al. Malignant rhabdoid tumour in an adult kidney: a case report. Mol Clin Oncol. 2019; 11:55–8.
Article9. Ayari Y, Ben Rhouma S, Boussaffa H, et al. Malignant rhabdoid tumor in a solitary kidney arising in an adult patient with chronic obstructive renal calculi. Int J Surg Case Rep. 2019; 58:85–7.
Article10. Sultan I, Qaddoumi I, Rodriguez-Galindo C, Nassan AA, Ghandour K, Al-Hussaini M. Age, stage, and radiotherapy, but not primary tumor site, affects the outcome of patients with malignant rhabdoid tumors. Pediatr Blood Cancer. 2010; 54:35–40.
Article11. Cheng JX, Tretiakova M, Gong C, Mandal S, Krausz T, Taxy JB. Renal medullary carcinoma: rhabdoid features and the absence of INI1 expression as markers of aggressive behavior. Mod Pathol. 2008; 21:647–52.
Article12. Gokden N, Nappi O, Swanson PE, et al. Renal cell carcinoma with rhabdoid features. Am J Surg Pathol. 2000; 24:1329–38.13. Beckwith JB, Palmer NF. Histopathology and prognosis of Wilms tumors: results from the First National Wilms’ Tumor Study. Cancer. 1978; 41:1937–48.14. Versteege I, Sevenet N, Lange J, et al. Truncating mutations of hSNF5/INI1 in aggressive paediatric cancer. Nature. 1998; 394:203–6.
Article15. Roberts CW, Galusha SA, McMenamin ME, Fletcher CD, Orkin SH. Haploinsufficiency of Snf5 (integrase interactor 1) predisposes to malignant rhabdoid tumors in mice. Proc Natl Acad Sci U S A. 2000; 97:13796–800.
Article16. Shannon B, Stan Wisniewski Z, Bentel J, Cohen RJ. Adult rhabdoid renal cell carcinoma. Arch Pathol Lab Med. 2002; 126:1506–10.
Article17. Wick MR, Ritter JH, Dehner LP. Malignant rhabdoid tumors: a clinicopathologic review and conceptual discussion. Semin Diagn Pathol. 1995; 12:233–48.18. Perry A, Fuller CE, Judkins AR, Dehner LP, Biegel JA. INI1 expression is retained in composite rhabdoid tumors, including rhabdoid meningiomas. Mod Pathol. 2005; 18:951–8.
Article19. Przybycin CG, McKenney JK, Reynolds JP, et al. Rhabdoid differentiation is associated with aggressive behavior in renal cell carcinoma: a clinicopathologic analysis of 76 cases with clinical follow-up. Am J Surg Pathol. 2014; 38:1260–5.20. Weeks DA, Beckwith JB, Mierau GW. Rhabdoid tumor: an entity or a phenotype? Arch Pathol Lab Med. 1989; 113:113–4.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rhabdoid Carcinoma of the Rectum
- Imaging Findings of a Malignant Rhabdoid Tumor in the Stomach: A Case Report
- A Case of Malignant Rhabdoid Tumor in the Anterior Mediastinum
- Epithelioid Malignant Intracerebral Nerve Sheath Tumor: A Case Report and a Comparison with Conventional Type
- Adult-Onset Sellar and Suprasellar Atypical Teratoid Rhabdoid Tumor Treated with a Multimodal Approach: A Case Report
