Sodium/glucose Co-Transporter 2 Inhibitor, Empagliflozin, Alleviated Transient Expression of SGLT2 after Myocardial Infarction
- Lee SY
 1,2
1,2 - Lee TW3
- Park GT3
- Kim JH2,3
- Lee HC4
- Han JH4,6
- Yoon A4,6
- Yoon D5
- Kim S5
- Jung SM1
- Choi JH1
- Chon MK1
- Lee SH1
- Hwang KW1
- Kim J1
- Park YH1
- Kim JH1
- Chun KJ1
- Hur J4,6
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea
- 2Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea
- 3Department of Physiology, School of Medicine, Pusan National University, Yangsan, Korea
- 4Department of Convergence Medicine, Pusan National University School of Medicine, Yangsan, Korea
- 5Department of Chemistry, Center for Proteome Biophysics and Chemistry Institute for Functional Materials, Pusan National University, Busan, Korea
- 6PNU GRAND Convergence Medical Science Education Research Center, Pusan National University School of Medicine, Yangsan, Korea
- KMID: 2513523
- DOI: http://doi.org/10.4070/kcj.2020.0303
Abstract
- Background and Objectives
Large clinical studies of sodium/glucose cotransporter 2 (SGLT2) inhibitors have shown a significant beneficial effect on heart failure-associated hospitalization and cardiovascular events. As SGLT2 is known to be absent in heart cells, improved cardiovascular outcomes are thought to be accounted for by the indirect effects of the drug. We sought to confirm whether such benefits were mediated through SGLT2 expressed in the heart using myocardial infarction (MI) model.
Methods
Mice pre-treated with empagliflozin (EMPA), an SGLT2 inhibitor, showed a significantly reduced infarct size compared with the vehicle group three days post-MI. Interestingly, we confirmed SGLT2 localized in the infarct zone. The sequential changes of SGLT2 expression after MI were also evaluated.
Results
One day after MI, SGLT2 transiently appeared in the ischemic areas in the vehicle group and increased until 72 hours. The appearance of SGLT2 was delayed and less in amount compared with the vehicle group. Additionally, there was a significant difference in metabolites, including glucose and amino acids in the 1 H nuclear magnetic resonance analysis between groups.
Conclusions
Our work demonstrates that SGLT2 is transiently expressed in heart tissue early after MI and EMPA may directly operate on SGLT2 to facilitate metabolic substrates shifts.
Keyword
Figure
-
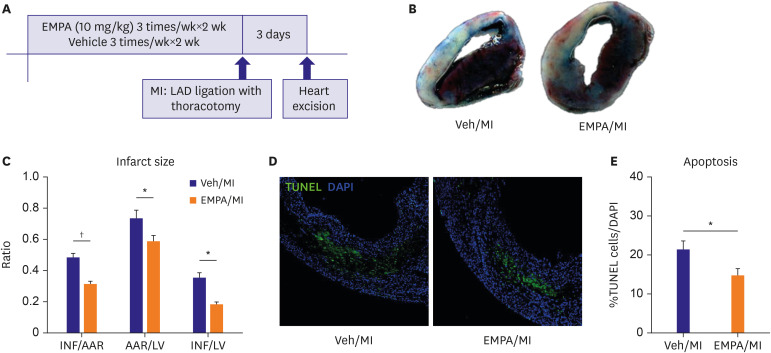
Figure 1 Pre-treatment of SGLT2i/EMPA reduced infarct size and apoptotic cells in non-diabetic MI model. (A) Experiment protocol. (B, C) Day 3 hearts were stained with 2,3,5-triphenyltetrazolium chloride for measurement of INF. Representative images and quantitative analysis of infarct size. (D, E) Apoptosis was evaluated by TUNEL staining (green) and DAPI staining (blue) with day 3 hearts. Representative images including infarct and infarct border zone and quantitative analysis of apoptotic cells (Scale bars: 50 μm).AAR = area at risk; DAPI = 4′,6-diamidino-2-phenylindole; EMPA = empagliflozin; INF = infarct area; LAD = left anterior descending; LV = left ventricular; MI = myocardial infarction; TUNEL = terminal deoxynucleotidyl transferase-mediated dUTP nick endlabeling; Veh = vehicle.*p<0.05, †p<0.001 between the 2 groups connected by line.
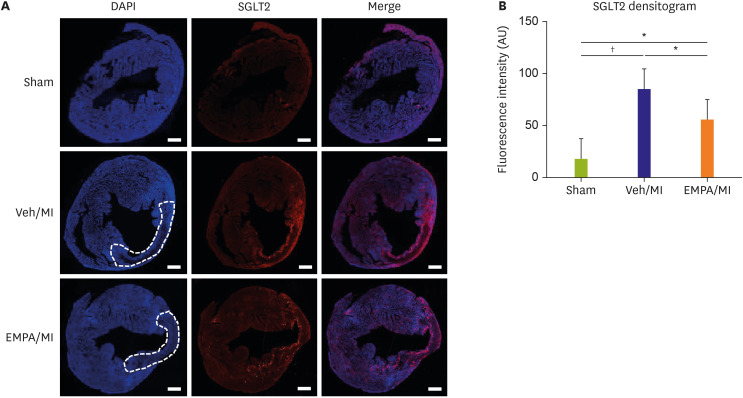
Figure 2 Expression of SGLT2 on mouse heart in infarcted area. (A) Representative images of immunofluorescence stain of SGLT2 on mouse heart 72 hours after MI. The infarcted zones are demarcated with dotted line. SGLT2 stained prominently on infarcted area regardless of EMPA treatment. (B) Quantitative analysis of SGLT2 fluorescence densitogram. Both vehicle and EMPA group showed significant increase in SGLT2 intensity. However, no difference between vehicle and EMPA group was noted (Scale bars: 500 μm).DAPI = 4′,6-diamidino-2-phenylindole; EMPA = empagliflozin; MI = myocardial infarction; SGLT2 = sodium/glucose cotransporter 2; Veh = vehicle.*p<0.05, †p<0.001 between the 2 groups connected by line.
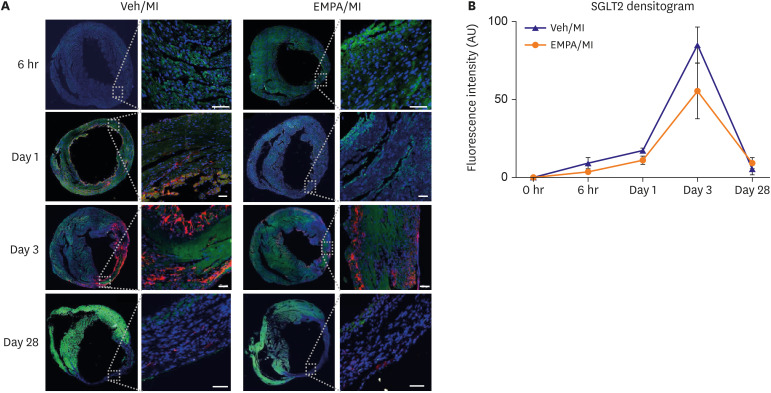
Figure 3 Transient expression of SGLT2 on ischemic mouse heart and suppressed SGLT2 expression on infarcted heart in EMPA treated group. (A) Representative images of time sequence after myocardial infarction. DAPI stains in blue, troponin T stains in green, SGLT2 stains in red. At 6 hours after MI, both group showed no SGLT2 stain. On day 1, in vehicle group, SGLT2 stain in infarcted area was noted, but not in EMPA group. On day 3, both group showed SGLT2 stain mainly on endo- and epicardial area of infarct zone. On day 28, both group showed little SGLT2 stain in infarct zone. (B) SGLT2 densitogram during time sequence showing inter-group difference of fluorescence intensity. EMPA group showing slower rate of increase of SGLT2 intensity and lower peak value than vehicle group (Scale bars: 50 μm).DAPI = 4′,6-diamidino-2-phenylindole; EMPA = empagliflozin; MI = myocardial infarction; SGLT2 = sodium/glucose cotransporter 2; Veh = vehicle.
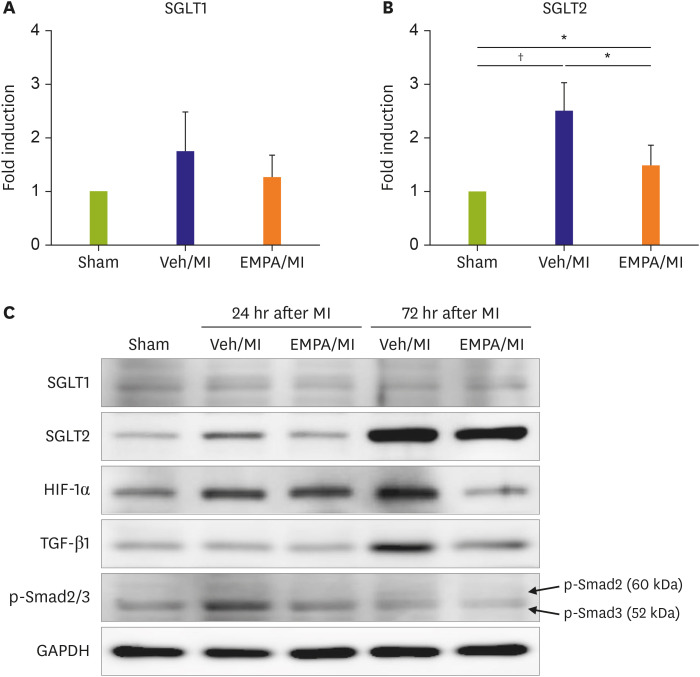
Figure 4 Post-MI 24 and 72 hours western blot showing the existence of SGLT2 on ischemic mice hearts and the effects of EMPA pre-treatment. Fold induction of SGLT1 (A) and SGLT2 (B) of each group from western blot analysis. SGLT1 showed no significant difference between all three groups. However SGLT2 was significantly elevated in the vehicle group compared with sham group (p=0.001). However when EMPA was pre-treated, SGLT2 protein level significantly decreased (p=0.037) in the ischemia condition, although the level is still higher than the sham group (p=0.048). (C) Additional western blot analysis of HIF-1α, TGF-β1 and phosphorylated SMAD2/3 at 24 hours and 72 hours after MI are also shown. The samples from different time sequence loaded in the same gel.EMPA = empagliflozin; GAPDH = glyceraldehyde 3-phosphate dehydrogenase; HIF-1α = Hypoxia-inducible Factor-1α; MI = myocardial infarction; p-SMAD = phosphorylated SMAD; SGLT1 = sodium/glucose cotransporter 1; SGLT2 = sodium/glucose cotransporter 2; TGF-β1 = transforming growth factor-β1; Veh = vehicle.*p<0.05, †p<0.01 between the 2 groups connected by line.
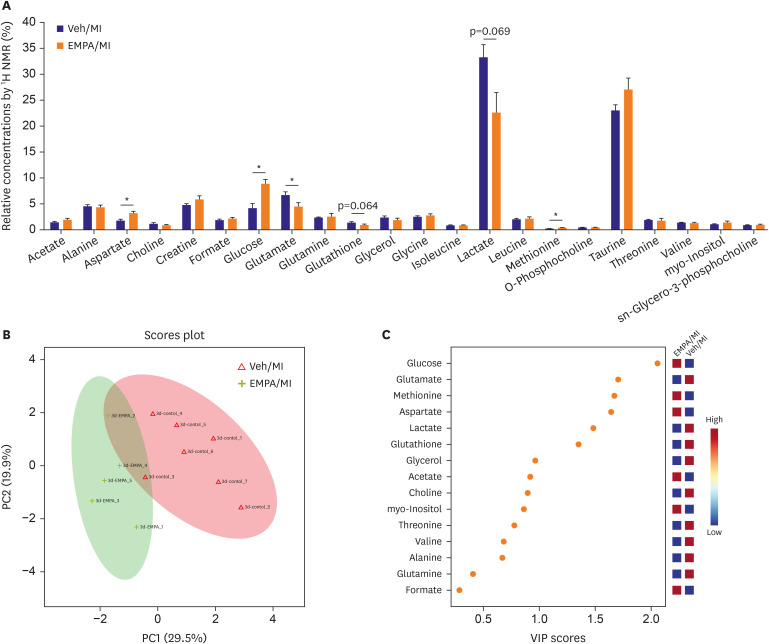
Figure 5 Metabolite analysis with 1H NMR. (A) The result of metabolite analysis by 1H NMR. (B) PCA score plot well differentiating metabolic profiles between EMPA and vehicle groups. Green for EMPA group and red for Vehicle group. (C) VIP score analysis.EMPA = empagliflozin; MI = myocardial infarction; NMR = nuclear magnetic resonance; PCA = principal components analysis; Veh = vehicle; VIP = variable importance in projection.*p<0.05.
Reference
-
1. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019; 380:347–357. PMID: 30415602.
Article2. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015; 373:2117–2128. PMID: 26378978.
Article3. Arnott C, Li Q, Kang A, et al. Sodium-glucose cotransporter 2 inhibition for the prevention of cardiovascular events in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. J Am Heart Assoc. 2020; 9:e014908. PMID: 31992158.
Article4. McMurray JJ, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019; 381:1995–2008. PMID: 31535829.5. Damman K, Beusekamp JC, Boorsma EM, et al. Randomized, double-blind, placebo-controlled, multicentre pilot study on the effects of empagliflozin on clinical outcomes in patients with acute decompensated heart failure (EMPA-RESPONSE-AHF). Eur J Heart Fail. 2020; 22:713–722. PMID: 31912605.
Article6. Vallon V. The mechanisms and therapeutic potential of SGLT2 inhibitors in diabetes mellitus. Annu Rev Med. 2015; 66:255–270. PMID: 25341005.
Article7. Chen J, Williams S, Ho S, et al. Quantitative PCR tissue expression profiling of the human SGLT2 gene and related family members. Diabetes Ther. 2010; 1:57–92. PMID: 22127746.
Article8. Ferrannini G, Hach T, Crowe S, Sanghvi A, Hall KD, Ferrannini E. Energy balance after sodium-glucose cotransporter 2 inhibition. Diabetes Care. 2015; 38:1730–1735. PMID: 26180105.
Article9. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017; 377:644–657. PMID: 28605608.
Article10. Uthman L, Baartscheer A, Schumacher CA, et al. Direct cardiac actions of sodium glucose cotransporter 2 inhibitors target pathogenic mechanisms underlying heart failure in diabetic patients. Front Physiol. 2018; 9:1575. PMID: 30519189.
Article11. Ndibalema AR, Kabuye D, Wen S, Li L, Li X, Fan Q. Empagliflozin protects against proximal renal tubular cell injury induced by high glucose via regulation of hypoxia-inducible factor 1-alpha. Diabetes Metab Syndr Obes. 2020; 13:1953–1967. PMID: 32606855.12. Zapata-Morales JR, Galicia-Cruz OG, Franco M, Martinez Y Morales F. Hypoxia-inducible factor-1α (HIF-1α) protein diminishes sodium glucose transport 1 (SGLT1) and SGLT2 protein expression in renal epithelial tubular cells (LLC-PK1) under hypoxia. J Biol Chem. 2014; 289:346–357. PMID: 24196951.
Article13. Panchapakesan U, Pegg K, Gross S, et al. Effects of SGLT2 inhibition in human kidney proximal tubular cells--renoprotection in diabetic nephropathy? PLoS One. 2013; 8:e54442. PMID: 23390498.
Article14. Yurista SR, Silljé HH, Oberdorf-Maass SU, et al. Sodium-glucose co-transporter 2 inhibition with empagliflozin improves cardiac function in non-diabetic rats with left ventricular dysfunction after myocardial infarction. Eur J Heart Fail. 2019; 21:862–873. PMID: 31033127.
Article15. Wright EM, Hirayama BA, Loo DF. Active sugar transport in health and disease. J Intern Med. 2007; 261:32–43. PMID: 17222166.
Article16. Zhou L, Cryan EV, D'Andrea MR, Belkowski S, Conway BR, Demarest KT. Human cardiomyocytes express high level of Na+/glucose cotransporter 1 (SGLT1). J Cell Biochem. 2003; 90:339–346. PMID: 14505350.
Article17. Tazawa S, Yamato T, Fujikura H, et al. SLC5A9/SGLT4, a new Na+-dependent glucose transporter, is an essential transporter for mannose, 1,5-anhydro-D-glucitol, and fructose. Life Sci. 2005; 76:1039–1050. PMID: 15607332.
Article18. Banerjee SK, McGaffin KR, Pastor-Soler NM, Ahmad F. SGLT1 is a novel cardiac glucose transporter that is perturbed in disease states. Cardiovasc Res. 2009; 84:111–118. PMID: 19509029.
Article19. Di Franco A, Cantini G, Tani A, et al. Sodium-dependent glucose transporters (SGLT) in human ischemic heart: a new potential pharmacological target. Int J Cardiol. 2017; 243:86–90. PMID: 28526540.
Article20. Lambert R, Srodulski S, Peng X, Margulies KB, Despa F, Despa S. Intracellular Na+ concentration ([Na+]i) is elevated in diabetic hearts due to enhanced Na+-glucose cotransport. J Am Heart Assoc. 2015; 4:e002183. PMID: 26316524.
Article21. Van Steenbergen A, Balteau M, Ginion A, et al. Sodium-myoinositol cotransporter-1, SMIT1, mediates the production of reactive oxygen species induced by hyperglycemia in the heart. Sci Rep. 2017; 7:41166. PMID: 28128227.
Article22. Vrhovac I, Balen Eror D, Klessen D, et al. Localizations of Na(+)-D-glucose cotransporters SGLT1 and SGLT2 in human kidney and of SGLT1 in human small intestine, liver, lung, and heart. Pflugers Arch. 2015; 467:1881–1898. PMID: 25304002.
Article23. Kashiwagi Y, Nagoshi T, Yoshino T, et al. Expression of SGLT1 in human hearts and impairment of cardiac glucose uptake by phlorizin during ischemia-reperfusion injury in mice. PLoS One. 2015; 10:e0130605. PMID: 26121582.
Article24. Ferrannini E, Mark M, Mayoux E. CV protection in the EMPA-REG OUTCOME trial: a “thrifty substrate” hypothesis. Diabetes Care. 2016; 39:1108–1114. PMID: 27289126.
Article25. Stanley WC, Recchia FA, Lopaschuk GD. Myocardial substrate metabolism in the normal and failing heart. Physiol Rev. 2005; 85:1093–1129. PMID: 15987803.
Article26. Taegtmeyer H, Goodwin GW, Doenst T, Frazier OH. Substrate metabolism as a determinant for postischemic functional recovery of the heart. Am J Cardiol. 1997; 80:3A–10A.
Article27. Taegtmeyer H. Energy metabolism of the heart: from basic concepts to clinical applications. Curr Probl Cardiol. 1994; 19:59–113. PMID: 8174388.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sodium Glucose Co-Transporter 2 (SGLT2) Inhibitor
- Sodium-Glucose Cotransporter 2 Inhibitors: Mechanisms of Action and Various Effects
- Glucose Lowering Effect of SGLT2 Inhibitors: A Review of Clinical Studies
- Effect of Empagliflozin, a Selective Sodium-Glucose Cotransporter 2 Inhibitor, on Kidney and Peripheral Nerves in Streptozotocin-Induced Diabetic Rats
- Inhibition of Sodium-Glucose Cotransporter-2 during Serum Deprivation Increases Hepatic Gluconeogenesis via the AMPK/AKT/FOXO Signaling Pathway
