Unusual Pharyngo-Esophageal Dysphagia Caused by a High-Riding Right Brachiocephalic Artery
- Affiliations
-
- 1Department of Rehabilitation Medicine, Kangwon National University Hospital, Chuncheon, Korea
- 2Department of Rehabilitation Medicine, Kangwon National University School of Medicine, Chuncheon, Korea
- KMID: 2513233
- DOI: http://doi.org/10.5535/arm.20057
Abstract
- High-riding right brachiocephalic and subclavian arteries are often asymptomatic and rare vascular variations. We present a patient with high-riding right brachiocephalic and subclavian arteries that caused compressive pharyngeal and cervical esophageal dysphagia. An 82-year-old woman presented to our hospital with dysphagia that worsened with solid food. A pulsatile lump was observed on the right neck side. A videofluoroscopic swallowing study showed a deviated food bolus movement anterolaterally from the normal vertical pharyngoesophageal transition, with a filling defect in the lower pharynx through the upper esophagus. Neck computed tomography (CT) showed high-riding right brachiocephalic and subclavian arteries and a tortuous right common carotid artery located adjacent to the trachea in the cervical area. The cervical midline structures were deviated to the left neck side. A neck mass with vascular variation should be considered as a cause of dysphagia that worsens with solid food; CT should be considered to determine its cause.
Figure
-

Fig. 1. The esophageal phase of thin fluid swallowing during the videofluoroscopic swallowing study. Both the lateral projection (A) and anterior-posterior views (B) showed a filling defect (white arrow) in the lower pharynx through the upper esophagus at the C4-7 vertebral level. The black dotted line delineates the thin fluid bolus.

Fig. 2. Enhanced neck computed tomography shows high-riding right brachiocephalic artery (RBA) and right subclavian artery (RSA): (A) sagittal 2D view, (B) coronal 2D view, (C) axial 2D view, (D, E) 3D reconstruction image. (A, D) The RSA branched out from the RBA at the C5 vertebral level and coursed downward posteriorly to the RBA. (B, E) The RSA occupied the right neck area laterally to the trachea. (C) The RSA compressed the midline neck structures, and a left tracheal deviation was observed at the C5 vertebral level. RCA, right common carotid artery; RJV, right jugular vein; LCA, left common carotid artery; LJV, left jugular vein.
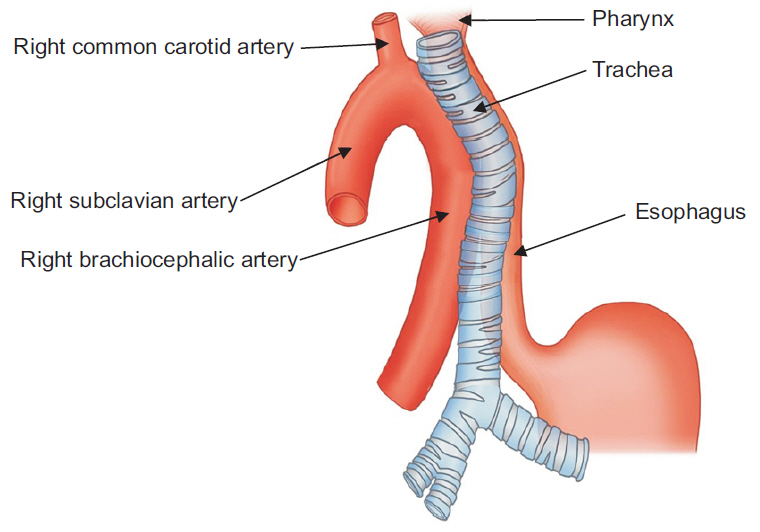
Fig. 3. Tracheal, pharyngeal, and esophageal compression by high-riding right brachiocephalic and subclavian arteries.
Reference
-
1. Groher ME, Bukatman R. The prevalence of swallowing disorders in two teaching hospitals. Dysphagia. 1986; 1:3–6.
Article2. Gupta V, Niranjan K, Rawat L, Gupta AK. Stent-graft repair of a large cervical internal carotid artery pseudoaneurysm causing dysphagia. Cardiovasc Intervent Radiol. 2009; 32:558–62.
Article3. Gupta A, Winslet MC. Tortuous common carotid artery as a cause of dysphagia. J R Soc Med. 2005; 98:275–6.
Article4. Gamache FW Jr, Voorhies RM. Hypertrophic cervical osteophytes causing dysphagia: a review. J Neurosurg. 1980; 53:338–44.5. Bakheit AM. Management of neurogenic dysphagia. Postgrad Med J. 2001; 77:694–9.
Article6. Carucci LR, Turner MA. Dysphagia revisited: common and unusual causes. Radiographics. 2015; 35:105–22.
Article7. Upadhyaya PK, Bertellotti R, Laeeq A, Sugimoto J. Beware of the aberrant innominate artery. Ann Thorac Surg. 2008; 85:653–4.
Article8. Dua SG, Purandare NC, Pramesh CS. Incidental detection of high-riding innominate artery and bilateral retropharyngeal carotid arteries: radiological findings and clinical relevance. Clin Radiol. 2011; 66:685–7.
Article9. Chegar BE, Emko P. Bilateral vocal cord paralysis secondary to esophageal compression. Am J Otolaryngol. 2004; 25:361–3.
Article
