Ann Pediatr Endocrinol Metab.
2020 Dec;25(4):277-281. 10.6065/apem.2040026.013.
Cushing syndrome with acute kidney injury due to ureteral stones in a 6-year-old boy
- Affiliations
-
- 1Department of Pediatrics, Severance Children's Hospital, Endocrine Research Institute, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2510900
- DOI: http://doi.org/10.6065/apem.2040026.013
Abstract
- Cushing syndrome (CS) is rare in children. The clinical presentation of CS varies according to extent and duration of glucocorticoid excess, and urolithiasis is a common complication. We report the first case of a patient with CS associated with acute kidney injury (AKI) due to urolithiasis. A 6-year-old boy presented to the Emergency Department with seizure. On physical examination, he had clinical features of CS and high blood pressure. Brain computed tomography (CT) suggested posterior reversible encephalopathy syndrome due to hypertension. On evaluation of hypertension, laboratory tests suggested adrenocortical tumor, but abdominal CT suggested pheochromocytoma. During further evaluation, his condition deteriorated with AKI due to bilateral ureteral stones, for which the patient underwent continuous renal replacement therapy in the intensive care unit. After controlling hypercortisolism with etomidate and performing ureteral stent indwelling, an adrenal mass was resected and histologically confirmed as an adrenocortical adenoma. We review the clinical manifestations, diagnosis, and management of CS associated with urolithiasis and AKI. Early recognition and careful monitoring of urolithiasis in CS patients are important to avoid severe complications of urolithiasis.
Figure
-

Fig. 1. (A) General appearance of the patient 10 months before admission. (B) General appearance of the patient with moon face, obesity, and hirsutism at admission.
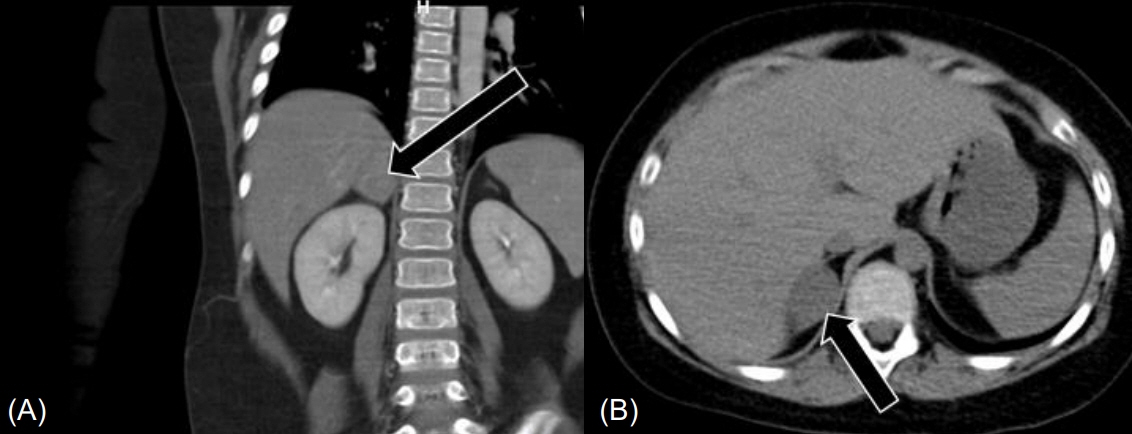
Fig. 2. Abdominal computed tomography revealed a 2.7-cm-sized mass in the right adrenal gland (black arrows) in coronal (A) and transverse images (B).
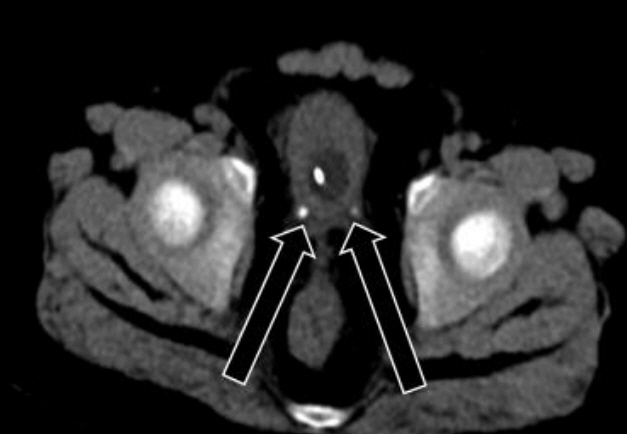
Fig. 3. Abdominal computed tomography revealed bilateral distal ureter stones (black arrows).
Reference
-
References
1. Nieman LK, Biller BM, Findling JW, Newell-Price J, Savage MO, Stewart PM, et al. The diagnosis of Cushing's syndrome: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2008; 93:1526–40.
Article2. Sharma ST, Nieman LK, Feelders RA. Cushing's syndrome: epidemiology and developments in disease management. Clin Epidemiol. 2015; 7:281–93.3. Lodish MB, Keil MF, Stratakis CA. Cushing's syndrome in pediatrics: an update. Endocrinol Metab Clin North Am. 2018; 47:451–62.4. Stratakis CA. An update on Cushing syndrome in pediatrics. Ann Endocrinol (Paris). 2018; 79:125–31.
Article5. Melo-Leite AF, Elias PC, Teixeira SR, Tucci S, Barros GE, Antonini SR, et al. Adrenocortical neoplasms in adulthood and childhood: distinct presentation. Review of the clinical, pathological and imaging characteristics. J Pediatr Endocrinol Metab. 2017; 30:253–76.
Article6. Farooqi S, Sarangarajan S, Shulman DI. Poor head growth as a presenting sign of a cortisol-secreting adrenal adenoma in a 2-year-old boy. J Pediatr. 2015; 166:764–6.
Article7. Bianchi D, Vespasiani G, Bove P. Acute kidney injury due to bilateral ureteral obstruction in children. World J Nephrol. 2014; 3:182–92.
Article8. Rahman SH, Papadakis GZ, Keil MF, Faucz FR, Lodish MB, Stratakis CA. Kidney stones as an underrecognized clinical sign in pediatric Cushing disease. J Pediatr. 2016; 170:273–7. e1.9. Miah T, Kamat D. Pediatric nephrolithiasis: a review. Pediatr Ann. 2017; 46:e242–4.
Article10. Aggarwal R, Srivastava A, Jain SK, Sud R, Singh R. Renal stones: a clinical review. EMJ Urol. 2017; 5:98–103.
Article11. Lodish M, Patronas NJ, Stratakis CA. Reversible posterior encephalopathy syndrome associated with micronodular adrenocortical disease and Cushing syndrome. Eur J Pediatr. 2010; 169:125–6.
Article12. Klein LA, Koyle M, Berg S. The emergency management of patients with ureteral calculi and fever. J Urol. 1983; 129:938–40.
Article13. Marien T, Miller NL. Treatment of the infected stone. Urol Clin North Am. 2015; 42:459–72.
Article14. Tresa V, Yaseen A, Lanewala AA, Hashmi S, Khatri S, Ali I, et al. Etiology, clinical profile and short-term outcome of acute kidney injury in children at a tertiary care pediatric nephrology center in Pakistan. Ren Fail. 2017; 39:26–31.
Article15. Sutherland SM, Kwiatkowski DM. Acute kidney injury in children. Adv Chronic Kidney Dis. 2017; 24:380–7.
Article16. Smets P, Meyer E, Maddens B, Daminet S. Cushing's syndrome, glucocorticoids and the kidney. Gen Comp Endocrinol. 2010; 169:1–10.
Article17. Schieda N, Siegelman ES. Update on CT and MRI of adrenal nodules. AJR Am J Roentgenol. 2017; 208:1206–17.
Article18. Lenders JW, Duh QY, Eisenhofer G, Gimenez-Roqueplo AP, Grebe SK, Murad MH, et al. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014; 99:1915–42.
Article19. Preda VA, Sen J, Karavitaki N, Grossman AB. Etomidate in the management of hypercortisolaemia in Cushing's syndrome: a review. Eur J Endocrinol. 2012; 167:137–43.20. Greening JE, Brain CE, Perry LA, Mushtaq I, Sales Marques J, Grossman AB, et al. Efficient short-term control of hypercortisolaemia by low-dose etomidate in severe paediatric Cushing's disease. Horm Res. 2005; 64:140–3.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Management of Ureteral Calculi with the Ureteroscopy: Failure Cases and Complications
- A Case of Cushing's Syndrome caused by Adrenocortical Carcinoma
- A Case of Cushing's Syndrome
- A Case Report of Acute Kidney Injury after Extracorporeal Shockwave Lithotripsy
- A Clinical Observation on Complete Anuria of Postrenal Type
