Neonatal Med.
2020 Nov;27(4):197-201. 10.5385/nm.2020.27.4.197.
Campomelic Dysplasia with Sex Reversal Harboring a Novel Frameshift Mutation
- Affiliations
-
- 1Department of Pediatrics, Asan Medical Center Children’s Hospital, Seoul, Korea
- 2Department of Pediatrics, Kyung Hee University Hospital at Gangdong, Seoul, Korea
- 3Medical Genetics Center, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2510826
- DOI: http://doi.org/10.5385/nm.2020.27.4.197
Abstract
- Campomelic dysplasia (CD) is a rare genetic disease characterized by skeletal dysplasia that also affects several other organ systems. CD is caused by a SOX9 mutation. We here report a case of CD with a 46, XY karyotype and female external genitalia. This child was born with a weight of 3.12 kg after 37 weeks of gestation. She exhibited a number of characteristic features including a small thoracic cage, bowing of both femurs, clubbed feet, hypoplastic scapula, 11 pairs of ribs, a bell-shaped narrow thorax, micrognathia, macroglossia, a cleft palate, a flattened nasal bridge, and low set ears. She experienced additional distress because of the presence of a tracheal ring and because she had tracheomalacia. CD was diagnosed through nucleotide sequence analysis. A frameshift mutation, c.235delC (p.Gln79Argfs*31), was identified in the SOX9 gene that has not previously been reported.
Keyword
Figure
-
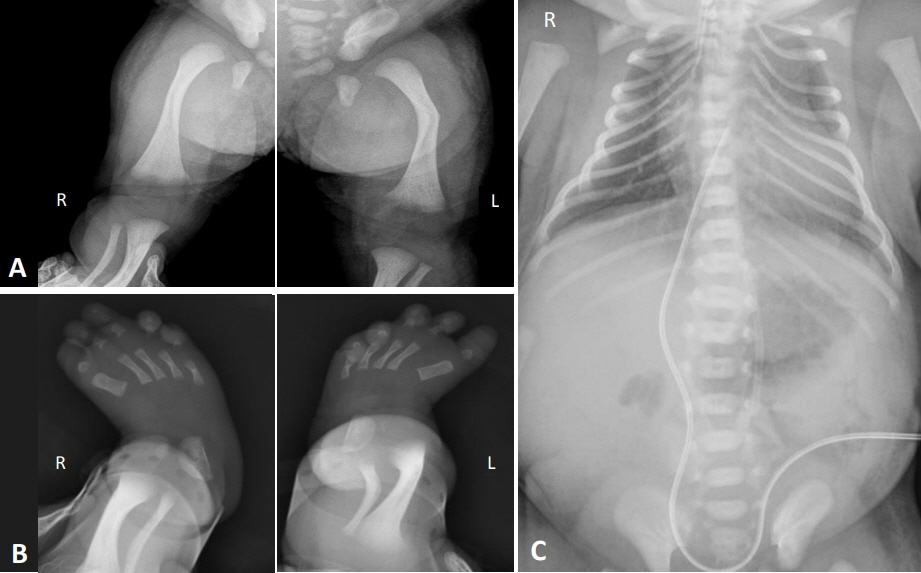
Figure 1. Radiographic examinations of the study patient showing (A) bowing of both femurs, (B) metatarsus adductus in both feet, and (C) 11 pairs of ribs and a bell-shaped thoracic cage.

Figure 2. Sequencing analysis of the SOX9 gene in the study patient identified a c.235del(C) heterozygous deletion mutation in exon 1, leading to a premature termination at codon 235.
Reference
-
1. Unger S, Scherer G, Superti-Furga A. Campomelic dysplasia. In : Adam AP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K, editors. GeneReviews. Seattle;University of Washington: 1993. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1760/.2. Mansour S, Hall CM, Pembrey ME, Young ID. A clinical and genetic study of campomelic dysplasia. J Med Genet. 1995; 32:415–20.3. Symon A, Harley V. SOX9: a genomic view of tissue specific expression and action. Int J Biochem Cell Biol. 2017; 87:18–22.4. Foster JW, Dominguez-Steglich MA, Guioli S, Kwok C, Weller PA, Stevanovic M, et al. Campomelic dysplasia and autosomal sex reversal caused by mutations in an SRY-related gene. Nature. 1994; 372:525–30.5. Kwok C, Weller PA, Guioli S, Foster JW, Mansour S, Zuffardi O, et al. Mutations in SOX9, the gene responsible for Campomelic dysplasia and autosomal sex reversal. Am J Hum Genet. 1995; 57:1028–36.6. Hattori T, Muller C, Gebhard S, Bauer E, Pausch F, Schlund B, et al. SOX9 is a major negative regulator of cartilage vascularization, bone marrow formation and endochondral ossification. Development. 2010; 137:901–11.7. Lefebvre V, Huang W, Harley VR, Goodfellow PN, de Crombrugghe B. SOX9 is a potent activator of the chondrocytespecific enhancer of the pro alpha1(II) collagen gene. Mol Cell Biol. 1997; 17:2336–46.8. Bell DM, Leung KK, Wheatley SC, Ng LJ, Zhou S, Ling KW, et al. SOX9 directly regulates the type-II collagen gene. Nat Genet. 1997; 16:174–8.9. Kent J, Wheatley SC, Andrews JE, Sinclair AH, Koopman P. A male-specific role for SOX9 in vertebrate sex determination. Development. 1996; 122:2813–22.10. Bernard P, Tang P, Liu S, Dewing P, Harley VR, Vilain E. Dimerization of SOX9 is required for chondrogenesis, but not for sex determination. Hum Mol Genet. 2003; 12:1755–65.11. Kim HY, Yoon CH, Kim GH, Yoo HW, Lee BS, Kim KS, et al. A case of campomelic dysplasia without sex reversal. J Korean Med Sci. 2011; 26:143–5.12. Ko JM, Hah JH, Kim SW, Cho TJ, Kim GH, Yoo HW. A Korean girl with campomelic dysplasia caused by a novel nonsense mutation within the SOX9 gene. J Genet Med. 2012; 9:89–92.13. Meyer J, Sudbeck P, Held M, Wagner T, Schmitz ML, Bricarelli FD, et al. Mutational analysis of the SOX9 gene in campomelic dysplasia and autosomal sex reversal: lack of genotype/phenotype correlations. Hum Mol Genet. 1997; 6:91–8.14. Mansour S, Offiah AC, McDowall S, Sim P, Tolmie J, Hall C. The phenotype of survivors of campomelic dysplasia. J Med Genet. 2002; 39:597–602.15. Pfeifer D, Kist R, Dewar K, Devon K, Lander ES, Birren B, et al. Campomelic dysplasia translocation breakpoints are scattered over 1 Mb proximal to SOX9: evidence for an extended control region. Am J Hum Genet. 1999; 65:111–24.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Campomelic Dysplasia without Sex Reversal
- A case of fetal skelectal anomaly of Campomelic syndrome
- A Korean Girl with Campomelic Dysplasia caused by a Novel Nonsense Mutation within the SOX9 Gene
- A Case with Spondyloepiphyseal Dysplasia Tarda with TRAPPC2 Mutation
- A Frameshift Mutation of the Pro-Apoptotic VDAC1 Gene in Cancers with Microsatellite Instability
