Long-Term Efficacy of Prophylactic Cavotricuspid Isthmus Ablation during Atrial Fibrillation Ablation in Patients Without Typical Atrial Flutter: a Prospective, Multicentre, Randomized Trial
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Division of Cardiology, Department of Internal Medicine, College of Medicine, St. Vincent's Hospital, The Catholic University of Korea, Seoul, Korea
- 3Department of Internal Medicine, Division of Cardiology, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 4Division of Cardiology, Department of Internal Medicine, College of Medicine, Daejeon St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea
- 5Division of Cardiology, Department of Internal Medicine, College of Medicine, Eunpyeong St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea
- 6Division of Cardiology, Department of Internal Medicine, College of Medicine, Yeouido St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea
- 7Division of Cardiology, Department of Internal Medicine, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea
- 8Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2509904
- DOI: http://doi.org/10.4070/kcj.2020.0174
Abstract
- Background and Objectives
Cavotricuspid isthmus (CTI) block is easily achieved, and prophylactic ablation can be performed during atrial fibrillation (AF) ablation. However, the previous study was too small and short-term to clarify the efficacy of this block.
Methods
Patients who underwent catheter ablation for paroxysmal AF were enrolled, and patients who had previous or induced atrial flutter (AFL) were excluded. We randomly assigned 366 patients to pulmonary vein isolation (PVI) only and prophylactic CTI ablation (PVI vs. PVI+CTI).
Results
There was no significant difference in procedure time between the two groups because most CTI blocks were performed during the waiting time after the PVI (176.8±72.6 minutes in PVI vs. 174.2±76.5 minutes in PVI+CTI, p=0.75). All patients were followed up for at least 18 months, and the median follow-up was 3.4 years. The recurrence rate of AF or AFL was not different in the 2 groups (25.7% in PVI vs. 25.7% in PVI+CTI, p=0.92). The recurrence rate of any AFL was not significantly different in the 2 groups (3.3% in PVI vs. 1.6% in PVI+CTI, p=0.31). The recurrence rate of typical AFL also was not different (0.5% in PVI vs. 0.5% in PVI+CTI, p=0.99).
Conclusions
In this large and long-term follow-up study, prophylactic CTI ablation had no benefit in patients with paroxysmal AF without typical AFL.
Figure
-
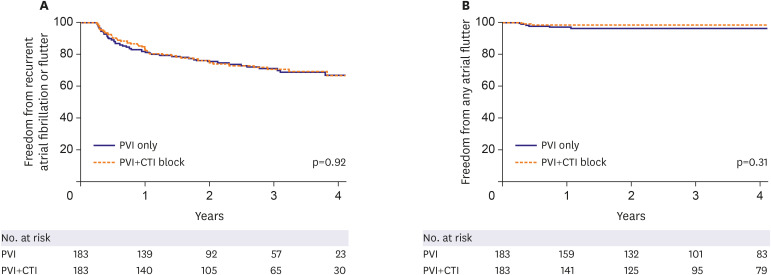
Figure 1 Kaplan-Meier curves for recurrence rates of atrial fibrillation or flutter (A) and any atrial flutter (B).CTI = cavotricuspid isthmus; PVI = pulmonary vein isolation.
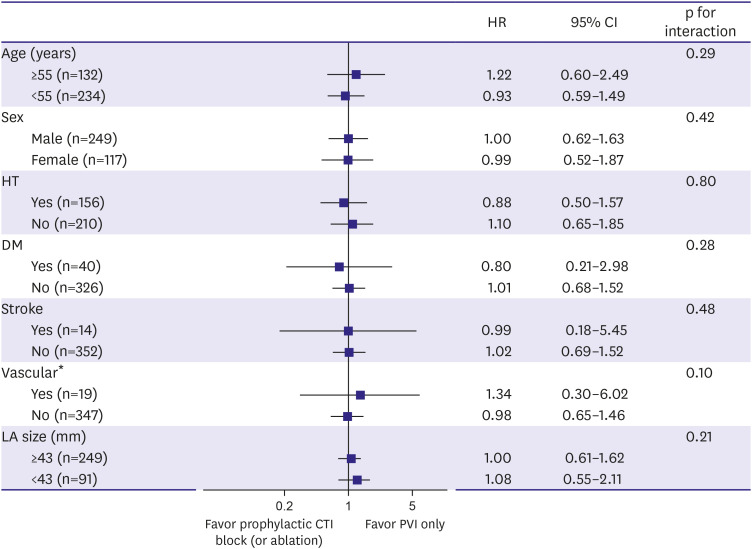
Figure 2 Interactions and hazard ratios for recurrence rates of atrial fibrillation or flutter.CI = confidence interval; CTI = cavotricuspid isthmus; DM = diabetes mellitus; HR = hazard ratio; HT = hypertension; LA = left atrial; PVI = pulmonary vein isolation.*Vascular disease included myocardial infarction, peripheral artery disease, and aortic plaque.
Cited by 2 articles
-
Prophylactic Cavotricuspid Isthmus Ablation in Patients without Typical Atrial Flutter: End of the Line
Eue-Keun Choi
Korean Circ J. 2020;51(1):65-67. doi: 10.4070/kcj.2020.0417.Rare and Elusive Arrhythmia: Atrial Tachycardia From Noncoronary Aortic Cusp During Catheter Ablation for Atrial Fibrillation
Jae-Sun Uhm
Korean Circ J. 2022;52(7):527-528. doi: 10.4070/kcj.2022.0137.
Reference
-
1. Feld G, Wharton M, Plumb V, et al. Radiofrequency catheter ablation of type 1 atrial flutter using large-tip 8- or 10-mm electrode catheters and a high-output radiofrequency energy generator: results of a multicenter safety and efficacy study. J Am Coll Cardiol. 2004; 43:1466–1472. PMID: 15093885.2. Calkins H, Canby R, Weiss R, et al. Results of catheter ablation of typical atrial flutter. Am J Cardiol. 2004; 94:437–442. PMID: 15325925.
Article3. Hsieh MH, Tai CT, Chiang CE, et al. Recurrent atrial flutter and atrial fibrillation after catheter ablation of the cavotricuspid isthmus: a very long-term follow-up of 333 patients. J Interv Card Electrophysiol. 2002; 7:225–231. PMID: 12510133.4. Scharf C, Veerareddy S, Ozaydin M, et al. Clinical significance of inducible atrial flutter during pulmonary vein isolation in patients with atrial fibrillation. J Am Coll Cardiol. 2004; 43:2057–2062. PMID: 15172412.
Article5. Roithinger FX, Karch MR, Steiner PR, SippensGroenewegen A, Lesh MD. Relationship between atrial fibrillation and typical atrial flutter in humans: activation sequence changes during spontaneous conversion. Circulation. 1997; 96:3484–3491. PMID: 9396445.6. Winter JB, Crijns HJ. Atrial flutter and atrial fibrillation: two sides of a coin or one coin? J Cardiovasc Electrophysiol. 2000; 11:859–860. PMID: 10969747.7. Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace. 2018; 20:e1–160.8. Kumagai K, Tojo H, Noguchi H, et al. Effects of cavotricuspid isthmus catheter ablation on paroxysmal atrial fibrillation. Jpn Heart J. 2001; 42:79–89. PMID: 11324809.
Article9. Pontoppidan J, Nielsen JC, Poulsen SH, et al. Prophylactic cavotricuspid isthmus block during atrial fibrillation ablation in patients without atrial flutter: a randomised controlled trial. Heart. 2009; 95:994–999. PMID: 19261602.
Article10. Chen J, de Chillou C, Basiouny T, et al. Cavotricuspid isthmus mapping to assess bidirectional block during common atrial flutter radiofrequency ablation. Circulation. 1999; 100:2507–2513. PMID: 10604888.
Article11. Calkins H, Kuck KH, Cappato R, et al. 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace. 2012; 14:528–606. PMID: 22389422.
Article12. Sawhney NS, Anousheh R, Chen WC, Feld GK. Diagnosis and management of typical atrial flutter. Cardiol Clin. 2009; 27:55–67. PMID: 19111764.
Article13. Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016; 37:2893–2962. PMID: 27567408.
Article14. Mesquita J, Ferreira AM, Cavaco D, et al. Impact of prophylactic cavotricuspid isthmus ablation in atrial fibrillation recurrence after a first pulmonary vein isolation procedure. Int J Cardiol. 2018; 259:82–87. PMID: 29579616.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of Atrial Flutter
- Prophylactic Cavotricuspid Isthmus Ablation in Patients without Typical Atrial Flutter: End of the Line
- The Difference of Left Atrial Volume Index: Can It Predict the Occurrence of Atrial Fibrillation after Radiofrequency Ablation of Atrial Flutter?
- Radiofreqeuncy Catheter Ablation for Tachyarrhythmia
- Initial Experience with Total Thoracoscopic Ablation
