J Korean Med Sci.
2020 Dec;35(48):e430. 10.3346/jkms.2020.35.e430.
Risk Factors for Intraprocedural Rerupture during Embolization of Ruptured Intracranial Aneurysms
- Affiliations
-
- 1Department of Neurosurgery, Renmin Hospital of Wuhan University, Wuhan, China
- KMID: 2509532
- DOI: http://doi.org/10.3346/jkms.2020.35.e430
Abstract
- Background
Intraprocedural rupture (IPR) is a devastating complication in endovascular treatment of ruptured intracranial aneurysms, but its risk factors have not been fully assessed. This study was performed to explore the risk factors for IPR during embolization of ruptured cerebral aneurysms.
Methods
A total of 1,494 patients with ruptured intracranial aneurysms who underwent endovascular interventional embolization were enrolled. Clinical characteristics were collected for each patient. Univariate and multivariate logistic regression analysis was employed to identify the factors independently associated with IPR. A receiver operating characteristic (ROC) curve analysis was performed to determine the cutoff values of continuous variables predicting IPR.
Results
Forty-one patients suffered from IPR (2.7%). Multivariate logistic regression analysis indicated that aneurysm size (odds ratio [OR], 0.819; 95% confidence interval [CI], 0.732–0.916), aneurysms with irregular morphology (OR, 2.162; 95% CI, 1.143–4.091), time from symptom onset to intervention (OR, 1.615; 95% CI, 1.207–2.161), and vasospasm during embolization (OR, 2.021; 95% CI, 1.038–3.934) were the independent risk factors of IPR. ROC curve analysis showed that the area under the curve for aneurysm size and time from onset to intervention were 0.697 (cutoff value, 3.4 mm; sensitivity, 78.8%; and specificity, 53.7%) and 0.659 (cutoff value, 2 days; sensitivity, 78.0%; and specificity, 45.2%), respectively.
Conclusion
Aneurysms with irregular morphology, aneurysms ≤ 3.4 mm in diameter, time from onset to intervention > 2 days and cerebral vasospasm during embolization are independent risk factors for IPR during coil embolization of ruptured aneurysms. More attention should be paid to the factors increasing the risk of IPR in patients with ruptured aneurysms so as to minimize this complication.
Figure
-
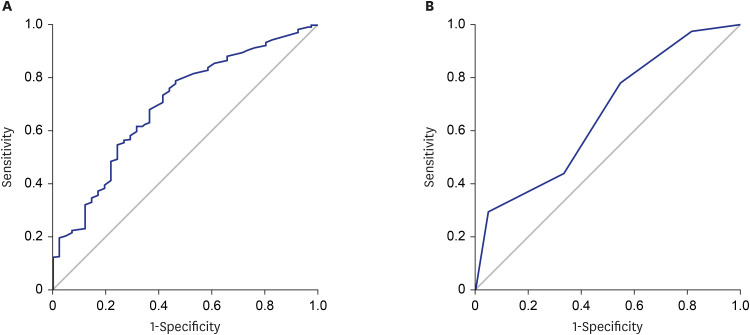
Fig. 1 The ROC curves for aneurysm size and time from onset to intervention. (A) The cutoff level of the aneurysm size for IPR. The cutoff level of 3.4 mm shows a sensitivity of 78.8% and a specificity of 53.7%. The AUC is 0.697. (B) The cutoff value of the time from onset to intervention for IPR. The cutoff level of 2 days shows a sensitivity of 78.0% and a specificity of 45.2%. The AUC is 0.659.ROC = receiver operating characteristic, IPR = intraprocedural rerupture, AUC = area under the curve.
Reference
-
1. Kang SD. Ruptured anterior communicating artery aneurysm causing bilateral oculomotor nerve palsy: a case report. J Korean Med Sci. 2007; 22(1):173–176. PMID: 17297277.2. Jeon BC, Chen SY, Zheng YR, Cho YW, Kwon KY. Superior orbital rim approach for anterior communicating artery aneurysms: a surgical series of 27 patients. J Korean Med Sci. 2003; 18(4):566–572. PMID: 12923335.
Article3. Stapleton CJ, Walcott BP, Butler WE, Ogilvy CS. Neurological outcomes following intraprocedural rerupture during coil embolization of ruptured intracranial aneurysms. J Neurosurg. 2015; 122(1):128–135. PMID: 25361491.
Article4. Zhang X, Long XA, Luo B, Karuna T, Duan CZ. Factors responsible for poor outcome after intraprocedural rerupture of ruptured intracranial aneurysms: identification of risk factors, prevention and management on 18 cases. Eur J Radiol. 2012; 81(1):e77–85. PMID: 21353424.
Article5. Elijovich L, Higashida RT, Lawton MT, Duckwiler G, Giannotta S, Johnston SC, et al. Predictors and outcomes of intraprocedural rupture in patients treated for ruptured intracranial aneurysms: the CARAT study. Stroke. 2008; 39(5):1501–1506. PMID: 18323484.6. Li L, Zhang X, Feng Z, Zhao R, Hong B, Xu Y, et al. Risk factors for intraprocedural rupture in the endovascular treatment of unruptured intracranial aneurysms: a single-center experience with 1232 procedures. World Neurosurg. 2019; 123:e9–14. PMID: 30278291.
Article7. Kawabata S, Imamura H, Adachi H, Tani S, Tokunaga S, Funatsu T, et al. Risk factors for and outcomes of intraprocedural rupture during endovascular treatment of unruptured intracranial aneurysms. J Neurointerv Surg. 2018; 10(4):362–366. PMID: 28710085.
Article8. Kocur D, Przybyłko N, Bażowski P, Baron J. Rupture during coiling of intracranial aneurysms: predictors and clinical outcome. Clin Neurol Neurosurg. 2018; 165:81–87. PMID: 29331871.
Article9. Choi W, Kwon SC, Lee WJ, Weon YC, Choi B, Lee H, et al. Feasibility and safety of mild therapeutic hypothermia in poor-grade subarachnoid hemorrhage: prospective pilot study. J Korean Med Sci. 2017; 32(8):1337–1344. PMID: 28665071.
Article10. Lindgren AE, Koivisto T, Björkman J, von Und Zu Fraunberg M, Helin K, Jääskeläinen JE, et al. Irregular shape of intracranial aneurysm indicates rupture risk irrespective of size in a population-based cohort. Stroke. 2016; 47(5):1219–1226. PMID: 27073241.
Article11. Zaidat OO, Ionita CC, Hussain SI, Alexander MJ, Friedman AH, Graffagnino C. Impact of ruptured cerebral aneurysm coiling and clipping on the incidence of cerebral vasospasm and clinical outcome. J Neuroimaging. 2009; 19(2):144–149. PMID: 18681928.
Article12. Arenillas JF, Candell-Riera J, Romero-Farina G, Molina CA, Chacón P, Aguadé-Bruix S, et al. Silent myocardial ischemia in patients with symptomatic intracranial atherosclerosis: associated factors. Stroke. 2005; 36(6):1201–1206. PMID: 15879333.13. Hokari M, Isobe M, Imai T, Chiba Y, Iwamoto N, Isu T. The impact of atherosclerotic factors on cerebral aneurysm is location dependent: aneurysms in stroke patients and healthy controls. J Stroke Cerebrovasc Dis. 2014; 23(9):2301–2307. PMID: 25156785.
Article14. Starke RM, Chalouhi N, Ding D, Raper DM, Mckisic MS, Owens GK, et al. Vascular smooth muscle cells in cerebral aneurysm pathogenesis. Transl Stroke Res. 2014; 5(3):338–346. PMID: 24323713.
Article15. Wang GX, Yu JY, Wen L, Zhang L, Mou KJ, Zhang D. Risk factors for the rupture of middle cerebral artery bifurcation aneurysms using CT angiography. PLoS One. 2016; 11(12):e0166654. PMID: 27977691.
Article16. Mitchell PJ, Muthusamy S, Dowling R, Yan B. Does small aneurysm size predict intraoperative rupture during coiling in ruptured and unruptured aneurysms? J Stroke Cerebrovasc Dis. 2013; 22(8):1298–1303. PMID: 23265780.
Article17. Nguyen TN, Raymond J, Guilbert F, Roy D, Bérubé MD, Mahmoud M, et al. Association of endovascular therapy of very small ruptured aneurysms with higher rates of procedure-related rupture. J Neurosurg. 2008; 108(6):1088–1092. PMID: 18518708.
Article18. van Rooij WJ, Keeren GJ, Peluso JP, Sluzewski M. Clinical and angiographic results of coiling of 196 very small (< or = 3 mm) intracranial aneurysms. AJNR Am J Neuroradiol. 2009; 30(4):835–839. PMID: 19131407.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combined Endovascular and Microsurgical Procedures as Complementary Approaches in the Treatment of a Single Intracranial Aneurysm
- Rebleeding of Ruptured Intracranial Aneurysms in the Immediate Postoperative Period after Coil Embolization
- Rerupture of Cerebral Aneurysms during Angiography: Report of 3 Cases
- Clinical Experience of Thromboembolic Complications of Coil Embolization for Intracranial Aneurysms with Literature Review
- Single-session Coil Embolization of Multiple Intracranial Aneurysms
