Characterization of dental phenotypes and treatment modalities in Korean patients with Parry–Romberg syndrome
- Affiliations
-
- 1Department of Orthodontics, School of Dentistry, Seoul National University, Seoul, Korea
- 2Department of Orthodontics, Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea
- KMID: 2508449
- DOI: http://doi.org/10.4041/kjod.2020.50.6.407
Abstract
Objective
To investigate the dental phenotypes and treatment modalities (TxMod) in Korean patients with Parry–Romberg syndrome (PRS) using longitudinal data.
Methods
The samples consisted of 10 PRS patients, who were treated and/or followed-up at Seoul National University Dental Hospital between 1998 and 2019. Using a novel PRS severity index based on the numbers of the atrophy-involved area and asymmetry-involved item, we classified them into mild (n = 3), moderate (n = 2), and severe (n = 5). Dental phenotypes, including congenitally missing tooth (Con-Missing-Tooth), microdontia, tooth with short root (Short-Root), tooth with dilacerated root, and delayed eruption/impacted tooth, were investigated along with Tx-Mod.
Results
The side of occurrence of all dental phenotypes showed 100% concordance with the side of PRS involvement. The most two common dental phenotypes were Con-MissingTooth and Short-Root (n = 29 and n = 17 in six patients). The sums of the average number of Con-Missing-Tooth and Short-Root increased from mild PRS to moderate PRS and severe PRS cases (1.0, 6.0, and 6.2). In terms of TxMod, growth observation due to mild atrophy, fixed orthodontic treatment, and grafting were used for mild PRS cases. Tx-Mod for moderate PRS cases involved growth observation for surgery due to an early age at the initial visit. For severe PRS cases, diverse Tx-Mod combinations including unilateral functional appliance, fixed orthodontic treatment, growth observation, grafting, and orthognathic surgery were used.
Conclusions
The novel PRS severity index may be useful to provide primary data for individualized diagnosis and treatment planning for PRS patients.
Keyword
Figure
-

Figure 1 Cephalometric and panoramic radiographs acquired from patients with Parry–Romberg syndrome (PRS) stratified by the PRS severity index. A, A patient with mild PRS (patient #8, left side involvement). B, A patient with moderate PRS (patient #5, right side involvement). C, A patient with severe PRS (patient #9, left side involvement).
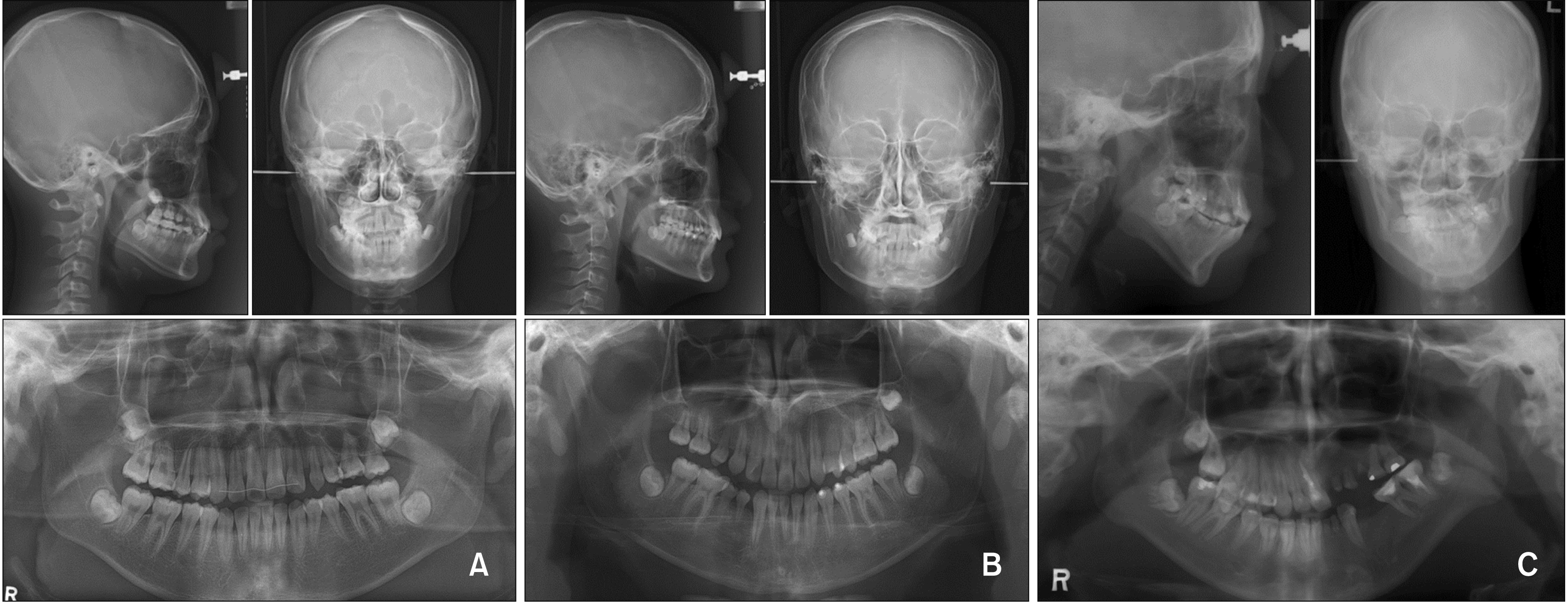
Figure 2 Facial photographs showing soft tissue atrophy and facial asymmetry in patients with Parry–Romberg syndrome. A, Soft tissue atrophy in the forehead (patient #7, left side involvement). B, Soft tissue atrophy in the peri-orbital tissue (patient #6, right side involvement). C, Soft tissue atrophy in the middle and lower thirds of the face, with a difference in the facial soft tissue volume between the affected and unaffected sides, deviation of the oral commissure, and chin point deviation (patient #2, right side involvement).
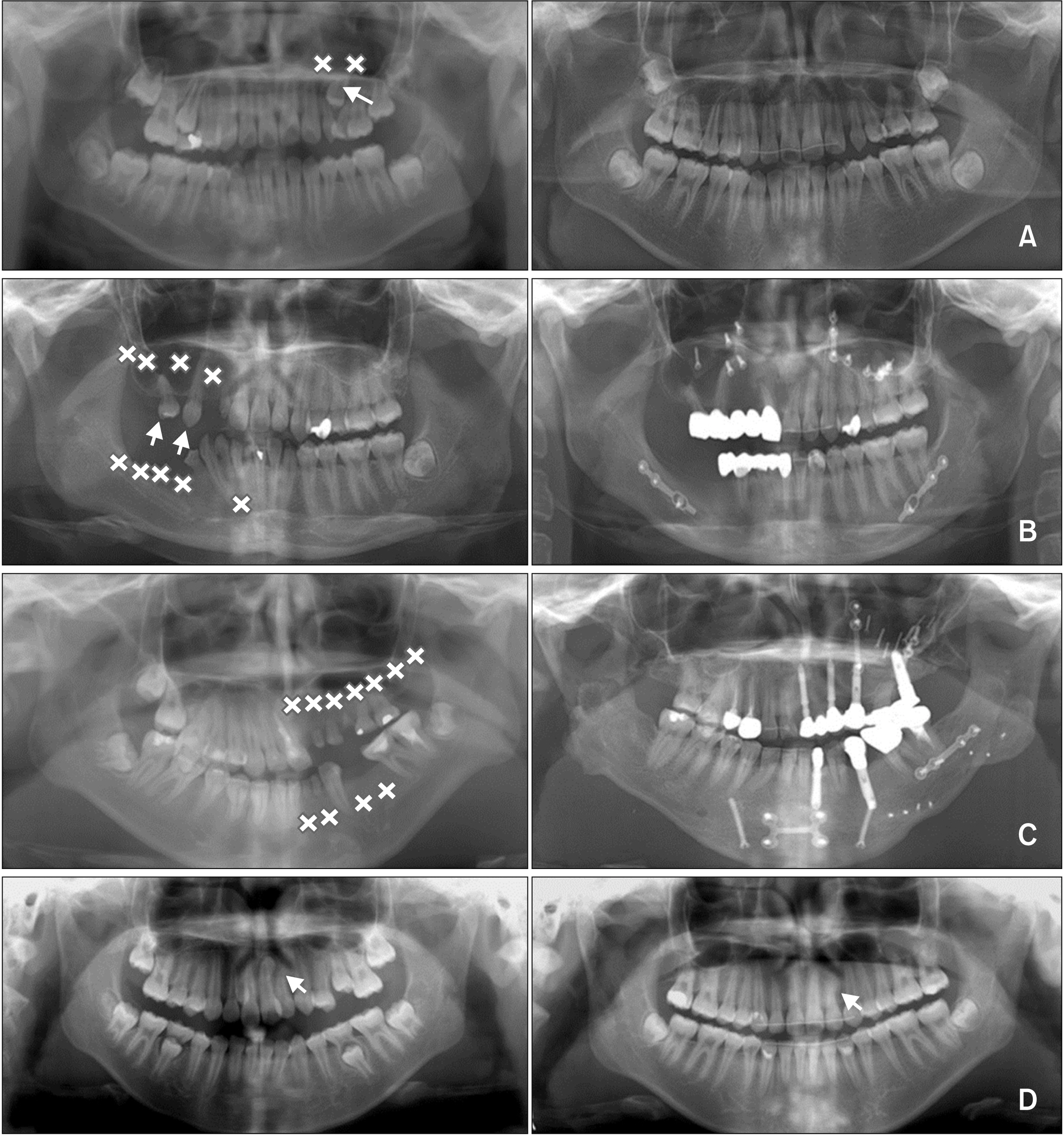
Figure 3 Treatment outcome of Parry–Romberg syndrome (PRS) patients according to the dental phenotype. A, Patient #8 (left side involvement) had congenital missing of #23 and #25 (x-mark), impaction and short root of #24 (arrow), and prolonged retention of #63 and #65. After extraction of #65, #24 was aligned using forced eruption with fixed orthodontic treatment. #63 was maintained for substitution of #23 and spaces were created on the mesial and distal sides of #63 to compensate for the absence of #25. B, Patient #6 (right side involvement) had multiple congenital missing of #12, #14, #16, #17, #41, #44–#47 (x-mark) and microdontia with short root of #13 and #15 (arrow). She was treated with orthognathic surgery with fixed orthodontic treatment. Then, multiple-unit bridges (#11-X-X-13-15 and #31-X-42-43-X) were fabricated; dental implants could not be placed because of severe atrophy of the alveolar bone. C, Patient #9 (left side involvement) had multiple congenital missing of #21–#27, #31, #32, #34, and #35 (x-mark). She was treated with orthognathic surgery with fixed orthodontic treatment. Then, congenitally missing teeth were replaced by retained deciduous teeth and dental implant prosthesis. D, Patient #7 (left side involvement) had dilacerated root of #22 (arrow). It was aligned at an appropriate location without side effect such as root resorption.
Reference
-
1. Stone J. 2003; Parry-Romberg syndrome: a global survey of 205 patients using the internet. Neurology. 61:674–6. DOI: 10.1212/WNL.61.5.674. PMID: 12963760.
Article2. Pinheiro TP, Silva CC, Silveira CS, Botelho PC, Pinheiro Md, Pinheiro Jde J. 2006; Progressive hemifacial atrophy--case report. Med Oral Patol Oral Cir Bucal. 11:E112–4. PMID: 16505785.3. Patel H, Thakkar C, Patel K. 2010; Parry-Romberg syndrome: a rare entity. J Maxillofac Oral Surg. 9:247–50. DOI: 10.1007/s12663-010-0103-y. PMID: 22190798. PMCID: PMC3177453.
Article4. El-Kehdy J, Abbas O, Rubeiz N. 2012; A review of Parry-Romberg syndrome. J Am Acad Dermatol. 67:769–84. DOI: 10.1016/j.jaad.2012.01.019. PMID: 22405645.
Article5. Stone J, Hunt D, Fernandes P. 2020. Parry Romberg syndrome [Internet]. National Organization for Rare Disorders;Danbury, CT: Available from: https://rarediseases.org/rare-diseases/parry-romberg-syndrome/. updated 2020; cited 2020 May 19.6. Blaszczyk M, Królicki L, Krasu M, Glinska O, Jablonska S. 2003; Progressive facial hemiatrophy: central nervous system involvement and relationship with scleroderma en coup de sabre. J Rheumatol. 30:1997–2004. PMID: 12966605.7. Gonul M, Dogan B, Izci Y, Varol G. 2005; Parry-Romberg syndrome in association with anti-dsDNA antibodies: a case report. J Eur Acad Dermatol Venereol. 19:740–2. DOI: 10.1111/j.1468-3083.2005.01290.x. PMID: 16268883.
Article8. O'Flynn S, Kinirons M. 2006; Parry-Romberg syndrome: a report of the dental findings in a child followed up for 9 years. Int J Paediatr Dent. 16:297–301. DOI: 10.1111/j.1365-263X.2006.00730.x. PMID: 16759329.9. Tollefson MM, Witman PM. 2007; En coup de sabre morphea and Parry-Romberg syndrome: a retrospective review of 54 patients. J Am Acad Dermatol. 56:257–63. DOI: 10.1016/j.jaad.2006.10.959. PMID: 17147965.
Article10. Al-Aizari NA, Azzeghaiby SN, Al-Shamiri HM, Darwish S, Tarakji B. 2015; Oral manifestations of Parry-Romberg syndrome: a review of literature. Avicenna J Med. 5:25–8. DOI: 10.4103/2231-0770.154193. PMID: 25878963. PMCID: PMC4394568.
Article11. de Vasconcelos Carvalho M, do Nascimento GJ, Andrade E, Andrade M, Sobral AP. 2010; Association of aesthetic and orthodontic treatment in Parry-Romberg syndrome. J Craniofac Surg. 21:436–9. DOI: 10.1097/SCS.0b013e3181cfe917. PMID: 20216455.12. Hu J, Yin L, Tang X, Gui L, Zhang Z. 2011; Combined skeletal and soft tissue reconstruction for severe Parry-Romberg syndrome. J Craniofac Surg. 22:937–41. DOI: 10.1097/SCS.0b013e31820fe27d. PMID: 21558914.
Article13. Foster TD. 1979; The effects of hemifacial atrophy on dental growth. Br Dent J. 146:148–50. DOI: 10.1038/sj.bdj.4804213. PMID: 283809.
Article14. Fayad S, Steffensen B. 1994; Root resorptions in a patient with hemifacial atrophy. J Endod. 20:299–303. DOI: 10.1016/S0099-2399(06)80821-6. PMID: 7931029.
Article15. Mazzeo N, Fisher JG, Mayer MH, Mathieu GP. 1995; Progressive hemifacial atrophy (Parry-Romberg syndrome). Case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 79:30–5. DOI: 10.1016/S1079-2104(05)80069-1. PMID: 7614157.
Article16. Urban J, Toruniowa B, Chibowska M. 1996; Progressive hemifacial atrophy: ten-year observation of a case. Cutis. 58:165–8. PMID: 8864604.17. Kurian K, Shanmugam S, Mathew B, Elongavan . 2003; Facial hemiatrophy--a report of 5 cases. Indian J Dent Res. 14:238–45. PMID: 15328992.18. Colquhoun AN, Ferguson MM, Doyle TC. 2000; Hemifacial atrophy with bilateral short roots. Br J Oral Maxillofac Surg. 38:533–6. DOI: 10.1054/bjom.2000.0461. PMID: 11010789.
Article19. Dixit S, Kalkur C, Sattur AP, Bornstein MM, Melton F. 2016; Scleroderma and dentistry: two case reports. J Med Case Rep. 10:297. DOI: 10.1186/s13256-016-1086-1. PMID: 27776552. PMCID: PMC5078903.
Article20. Grippaudo C, Deli R, Grippaudo FR, Di Cuia T, Paradisi M. 2004; Management of craniofacial development in the Parry-Romberg syndrome: report of two patients. Cleft Palate Craniofac J. 41:95–104. DOI: 10.1597/02-066. PMID: 14697063.
Article21. You KH, Baik HS. 2011; Orthopedic and orthodontic treatment of Parry-Romberg syndrome. J Craniofac Surg. 22:970–3. DOI: 10.1097/SCS.0b013e31820fe339. PMID: 21558909.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Eyelid Myokymia as the Presenting Feature of Parry-Romberg Syndrome
- Three-dimensional imaging of progressive facial hemiatrophy (Parry-Romberg syndrome) with unusual conjunctival findings
- Parry-Romberg Syndrome with Intermittent Exotropia
- Parry-Romberg Syndrome with Intracranial Vascular Dysplasia: A case report
- A Case of Parry-Romberg Syndrome in Neonate
