Korean J Gastroenterol.
2020 Oct;76(4):199-205. 10.4166/kjg.2020.76.4.199.
Clinical Impact of Common Bile Duct Angulation on the Recurrence of Common Bile Duct Stone: A Meta-analysis and Review
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea
- KMID: 2507767
- DOI: http://doi.org/10.4166/kjg.2020.76.4.199
Abstract
- Background/Aims
Local and systemic factors, such as diabetes, obesity, and hyperlipidemia, are considered risk factors for the recurrence of choledocholithiasis after successful endoscopic clearance. Local factors include the presence of bile sludge, common bile duct (CBD) diameter, and CBD angulation. Among them, it is unclear if acute CBD angulation is preferable to the recurrence of a CBD stone.
Methods
PubMed, EMBASE, CINAHL, the Cochrane Library databases, and google website were searched for randomized controlled trials reported in English and undertaken until August 2019. Meta‐analysis was performed on all randomized controlled trials for the recurrence of CBD stones between the patients with acute CBD angulation.
Results
Eight randomized trials (1,776 patients) were identified, and the total recurrent rate of CBD stones was 18.8% (334/1,776). A CBD angle ≤145° was significantly associated with an increased risk of recurrent CBD stone (OR=2.65, p<0.01). In two prospective studies, acute CBD angulation was not proven to be associated with a recurrence (p=0.39).
Conclusions
Approximately 20% of patients with a CBD stone showed recurrence after the complete clearance of the CBD stone, and a CBD angle ≤145° could increase the risk of recurrence. Overall, a large-scale prospective study should be necessary.
Keyword
Figure
-
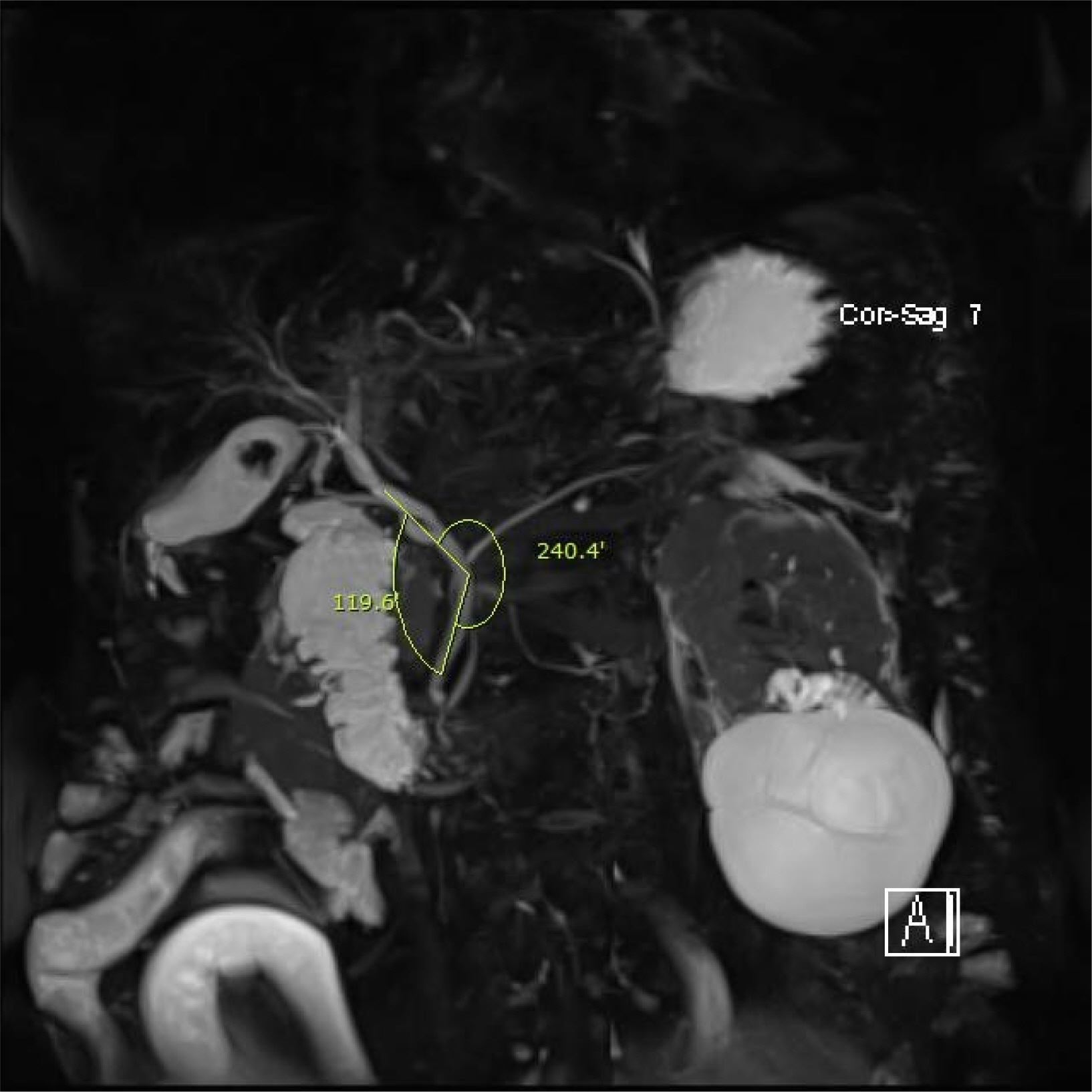
Fig. 1 Images of a patient diagnosed with acute cholangitis and common bile duct (CBD) stones show sharp CBD angulation (119.6°, from magnetic resonance cholangiopancreatography).
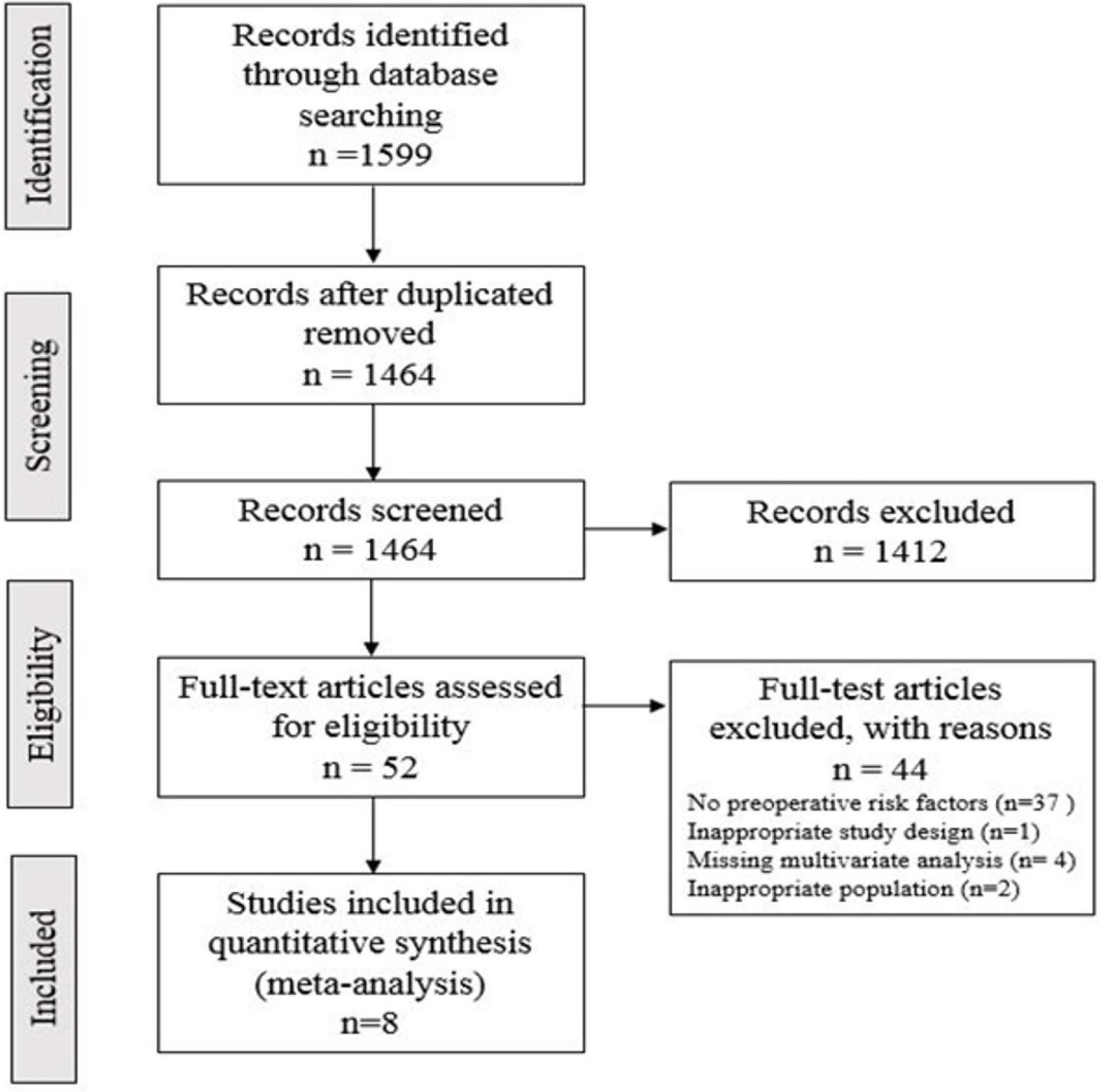
Fig. 2 Flow-chart of study selection.
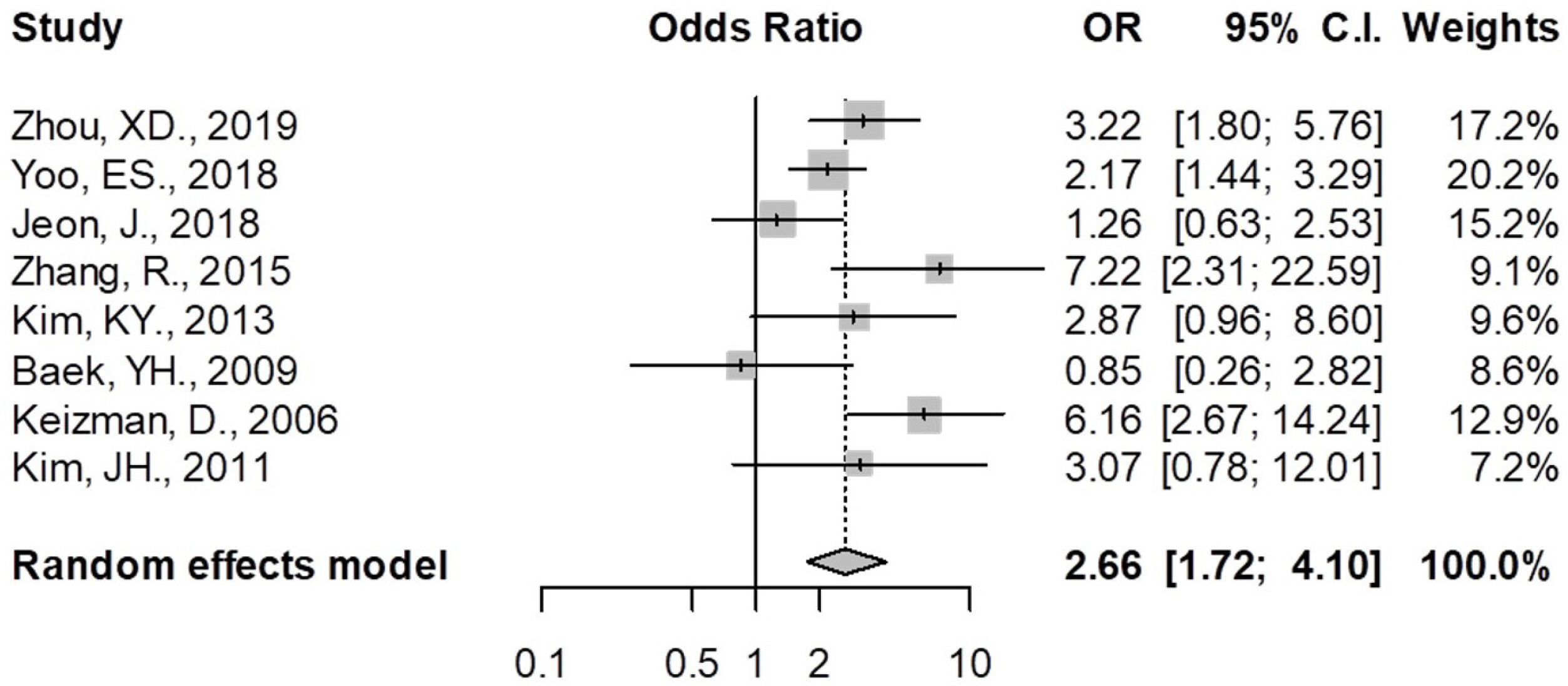
Fig. 3 Meta-analysis: odds ratios of common bile duct (CBD) angulation for CBD stone recurrence.

Fig. 4 Funnel plot of the study did not show publication bias.
Reference
-
1. Boerma D, Rauws EA, Keulemans YC, et al. 2002; Wait-and-see policy or laparoscopic cholecystectomy after endoscopic sphincterotomy for bile-duct stones: a randomised trial. Lancet. 360:761–765. DOI: 10.1016/S0140-6736(02)09896-3. PMID: 12241833.
Article2. Song ME, Chung MJ, Lee DJ, et al. 2016; Cholecystectomy for prevention of recurrence after endoscopic clearance of bile duct stones in Korea. Yonsei Med J. 57:132–137. DOI: 10.3349/ymj.2016.57.1.132. PMID: 26632393. PMCID: PMC4696944.
Article3. Prat F, Malak NA, Pelletier G, et al. 1996; Biliary symptoms and complications more than 8 years after endoscopic sphincterotomy for choledocholithiasis. Gastroenterology. 110:894–899. DOI: 10.1053/gast.1996.v110.pm8608900. PMID: 8608900.
Article4. Oak JH, Paik CN, Chung WC, Lee KM, Yang JM. 2012; Risk factors for recurrence of symptomatic common bile duct stones after cholecystectomy. Gastroenterol Res Pract. 2012:417821. DOI: 10.1155/2012/417821. PMID: 22991508. PMCID: PMC3443611.
Article5. Zhou XD, Chen QF, Zhang YY, et al. 2019; Outcomes of endoscopic sphincterotomy vs open choledochotomy for common bile duct stones. World J Gastroenterol. 25:485–497. DOI: 10.3748/wjg.v25.i4.485. PMID: 30700944. PMCID: PMC6350168.
Article6. Kim KY, Han J, Kim HG, et al. 2013; Late complications and stone recurrence rates after bile duct stone removal by endoscopic sphincterotomy and large balloon dilation are similar to those after endoscopic sphincterotomy alone. Clin Endosc. 46:637–642. DOI: 10.5946/ce.2013.46.6.637. PMID: 24340257. PMCID: PMC3856265.
Article7. Keizman D, Shalom MI, Konikoff FM. 2006; An angulated common bile duct predisposes to recurrent symptomatic bile duct stones after endoscopic stone extraction. Surg Endosc. 20:1594–1599. DOI: 10.1007/s00464-005-0656-x. PMID: 16858527.
Article8. Keizman D, Ish Shalom M, Konikoff FM. 2006; Recurrent symptomatic common bile duct stones after endoscopic stone extraction in elderly patients. Gastrointest Endosc. 64:60–65. DOI: 10.1016/j.gie.2006.01.022. PMID: 16813804.
Article9. Zhang R, Luo H, Pan Y, et al. 2015; Rate of duodenal-biliary reflux increases in patients with recurrent common bile duct stones: evidence from barium meal examination. Gastrointest Endosc. 82:660–665. DOI: 10.1016/j.gie.2015.03.1908. PMID: 25952091.
Article10. Yoo ES, Yoo BM, Kim JH, et al. 2018; Evaluation of risk factors for recurrent primary common bile duct stone in patients with cholecystectomy. Scand J Gastroenterol. 53:466–470. DOI: 10.1080/00365521.2018.1438507. PMID: 29457922.
Article11. Kim JH, Kim YS, Kim DK, et al. 2011; Short-term clinical outcomes based on risk factors of recurrence after removing common bile duct stones with endoscopic papillary large balloon dilatation. Clin Endosc. 44:123–128. DOI: 10.5946/ce.2011.44.2.123. PMID: 22741123. PMCID: PMC3363062.
Article12. Jeon J, Lim SU, Park CH, Jun CH, Park SY, Rew JS. 2018; Restoration of common bile duct diameter within 2 weeks after endoscopic stone retraction is a preventive factor for stone recurrence. Hepatobiliary Pancreat Dis Int. 17:251–256. DOI: 10.1016/j.hbpd.2018.03.014. PMID: 29625836.
Article13. Baek YH, Kim HJ, Park JH, et al. 2009; Risk factors for recurrent bile duct stones after endoscopic clearance of common bile duct stones. Korean J Gastroenterol. 54:36–41. DOI: 10.4166/kjg.2009.54.1.36. PMID: 19696548.
Article14. Chong CC, Chiu PW, Tan T, et al. 2016; Correlation of CBD/CHD angulation with recurrent cholangitis in patients treated with ERCP. Endosc Int Open. 4:E62–E67. DOI: 10.1055/s-0035-1569689. PMID: 26788550. PMCID: PMC4713197.
Article15. Ando T, Tsuyuguchi T, Okugawa T, et al. 2003; Risk factors for recurrent bile duct stones after endoscopic papillotomy. Gut. 52:116–121. DOI: 10.1136/gut.52.1.116. PMID: 12477771. PMCID: PMC1773534.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Determination of Diameter and Angulation of the Normal Common Bile Duct using Multidetector Computed Tomography
- A Common Bile Duct Web Presenting with Obstructive Jaundice without Common Bile Duct Stone
- A Case of Villous Adenomas in the Common Bile Duct and Cystic Duct
- A case of limy bile accompanied with gallbladder stones and common bile duct stone
- Clinical Impact of Common Bile Duct Angulation for Recurrence of Bile Duct Stones
