Organ procurement in a deceased donor
- Affiliations
-
- 1Department of Surgery, Jeonbuk National University Medical School and Hospital, Jeonju, Korea
- 2Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 3Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 4Division of Transplantation and Vascular Surgery, Department of Surgery, Kyung Hee University College of Medicine, Seoul, Korea
- 5Department of Internal Medicine, Jeonbuk National University Medical School, Jeonju, Korea
- 6Department of Surgery, Yonsei University College of Medicine, Seoul, Korea
- 7Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea
- 8Department of Thoracic and Cardiovascular Surgery, Ajou University School of Medicine, Suwon, Korea
- 9Department of Surgery, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 10Department of Surgery, Research Institute of Clinical Medicine, Biomedical Research Institute, Jeonbuk National University Medical School and Hospital, Jeonju, Korea
- KMID: 2507153
- DOI: http://doi.org/10.4285/kjt.2020.34.3.134
Abstract
- With the increasing demand for organ transplantation, organ procurement from a deceased donor is an essential step for deceased donor organ transplantation. A proper surgical technique for the procurement of an organ graft from a deceased donor must be carried out to avoid any damage to it. Moreover, how to manage deceased donors until they enter the operating room in a stable condition is a critical point to be considered. The establishment of a surgical technique and preoperative management for organ procurement is encouraged to achieve a nationwide standard and consistency for organ graft sharing among the transplant units.
Keyword
Figure
-
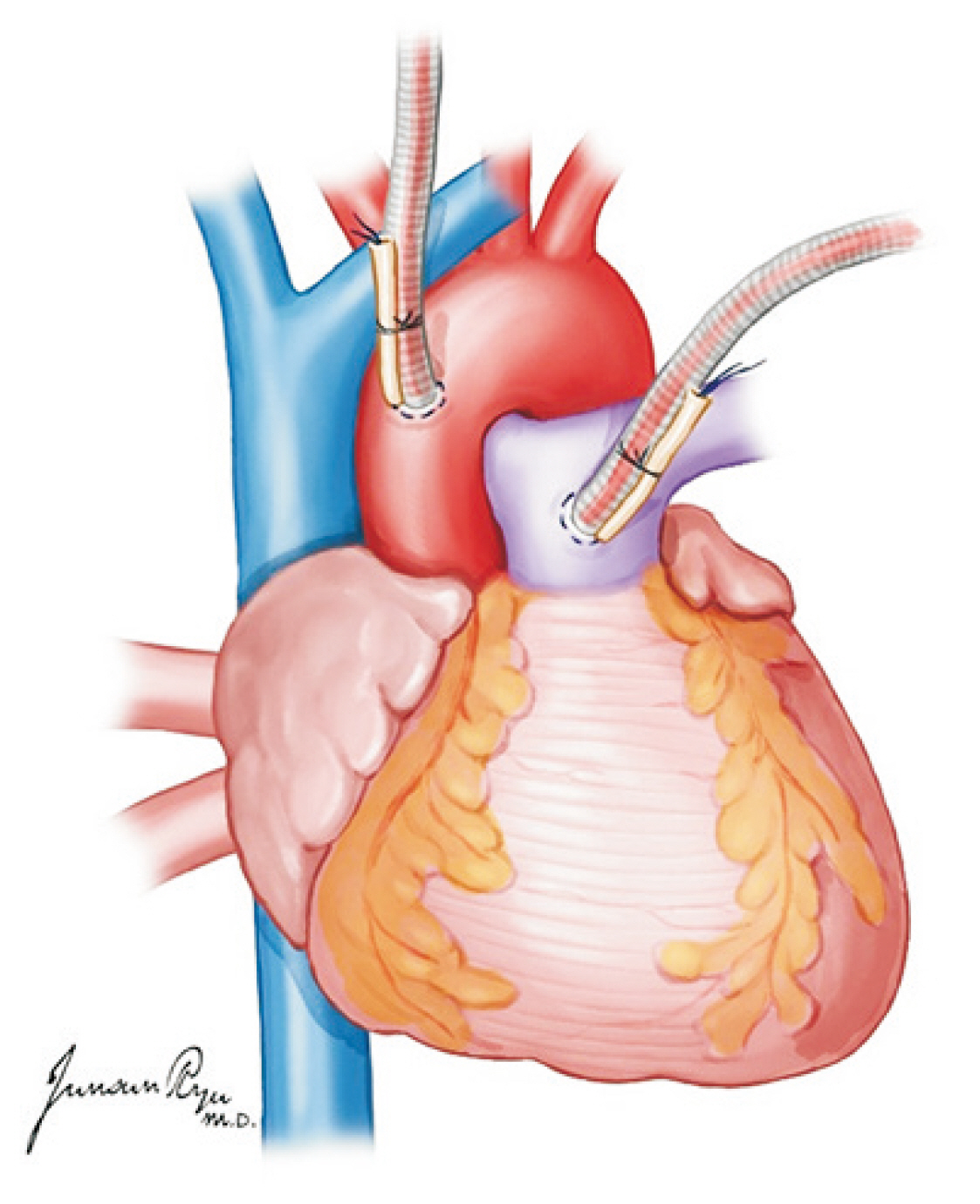
Fig. 1 An aortic cannula is inserted in the anterior ascending aorta, and a pulmonary artery (PA) is in the distal portion of the main PA. Placing the PA cannula too distally should be avoided because the cannula tip can enter either the right or left PA side.
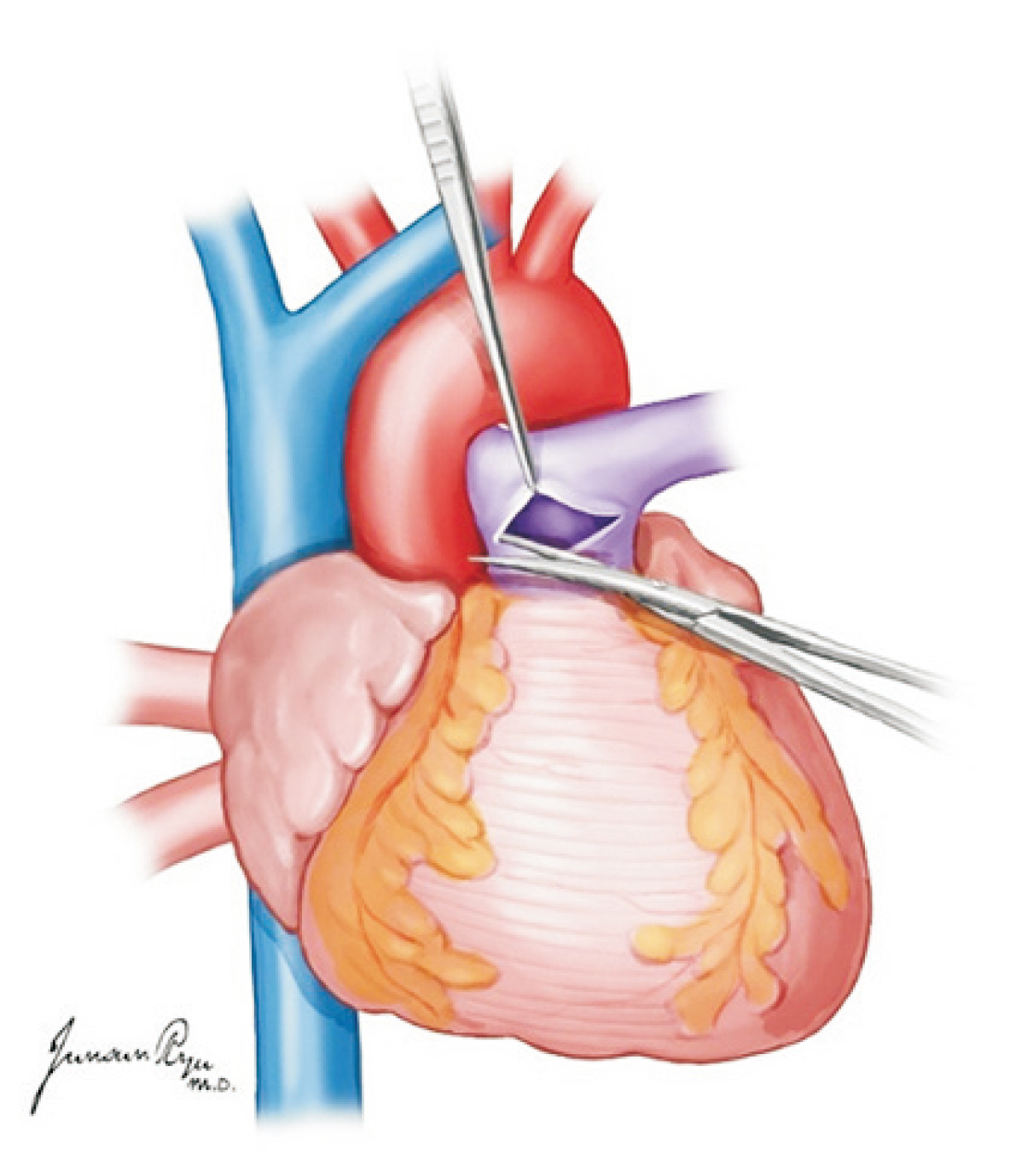
Fig. 2 The pulmonary artery (PA) is divided in the site where the cannula was inserted in the distal main PA while ensuring the left and right PA are not separated.
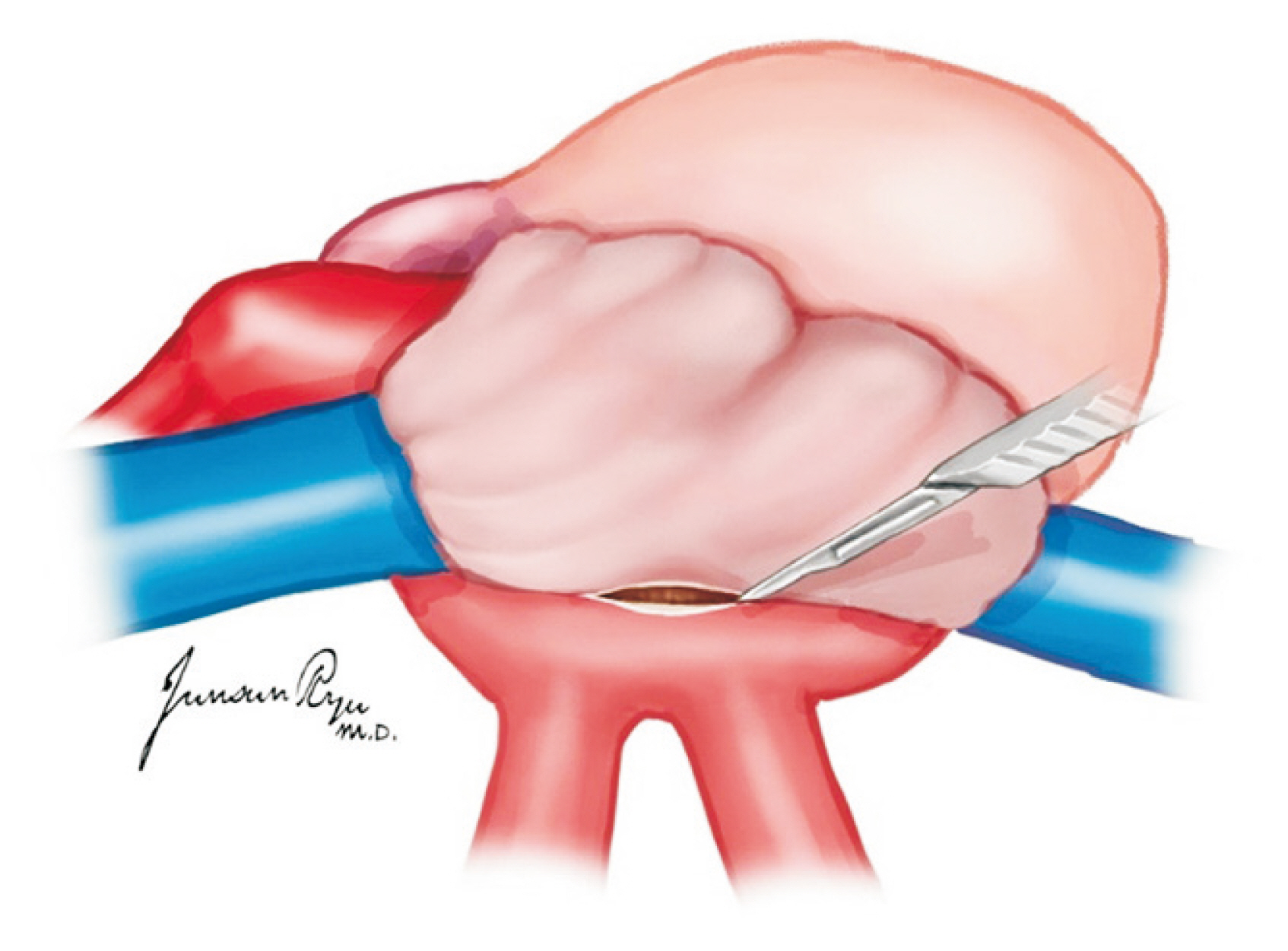
Fig. 3 When Waterston’s groove is incised, sufficient muscular cuff of the left atrium should be preserved. This cuff is most important when implanting the lung to the recipient.
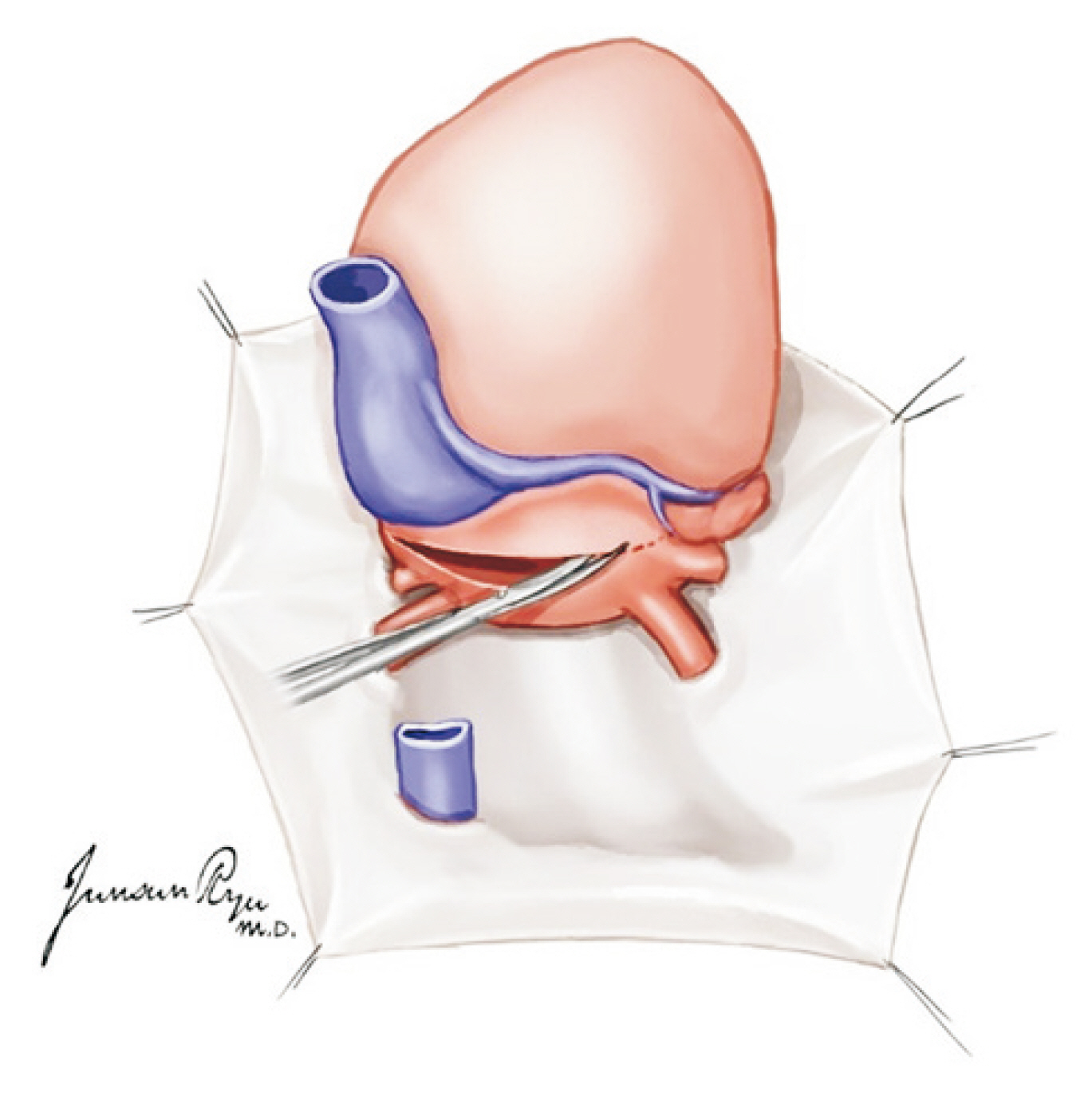
Fig. 4 After the incision of Waterston’s groove, the heart is lifted toward the head, and the left atrium is incised in a transverse manner. The heart should then be moved to the right, and the incision should be extended to dissect the left atrium.
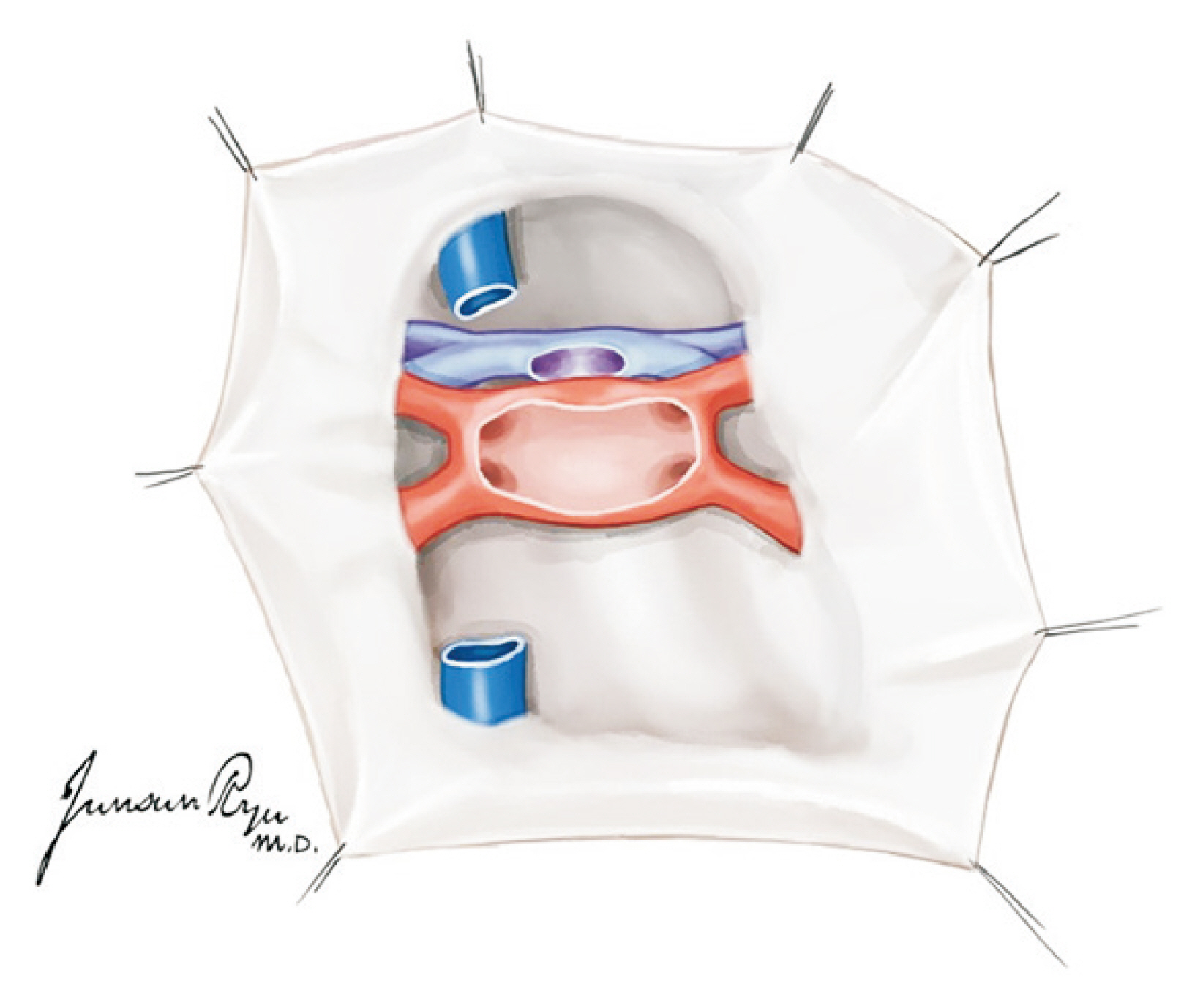
Fig. 5 After left atrium division, the left pulmonary veins should form a whole cuff.
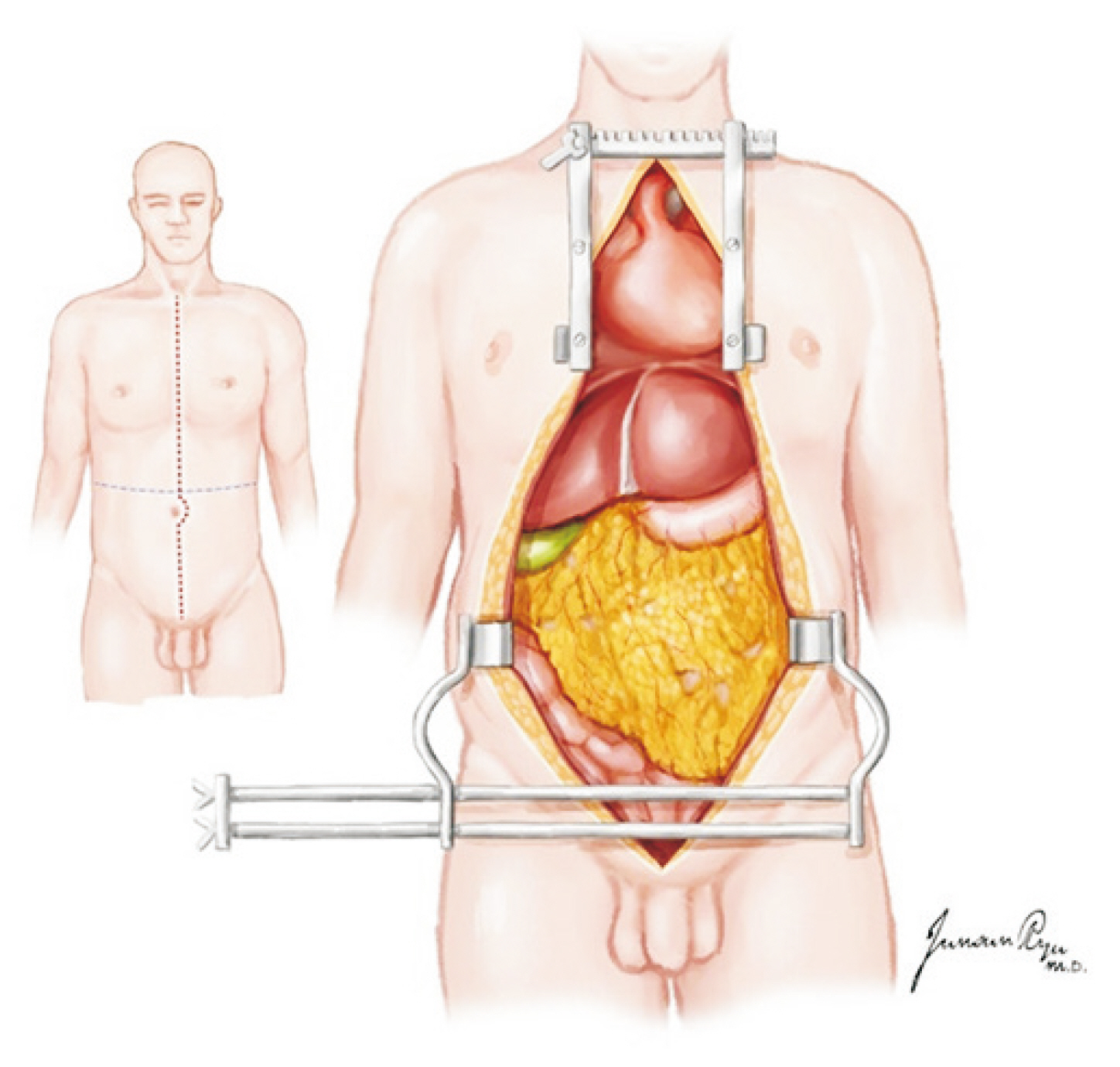
Fig. 6 An incision extending from the sternal notch to the pubis, which is cruciate at the level of the umbilicus, provides maximal exposure for multi-organ procurements.

Fig. 7 A Cattell–Braasch maneuver extending across the midline, with complete mobilization of the distal small bowel, right colon, and duodenum, allows for the identification of the distal aorta, iliac bifurcation, and distal inferior vena cava. Dotted line: initial dissection plane of Cattell-Braasch maneuver.

Fig. 8 Kocherization with the mobilization of the infrahepatic inferior vena cava and upper margin of both renal veins.

Fig. 9 After the mobilization of the left hepatic lobe, the supraceliac aorta should be exposed with movement of the esophagus toward the left and blunt dissection of the periaortic soft tissue.
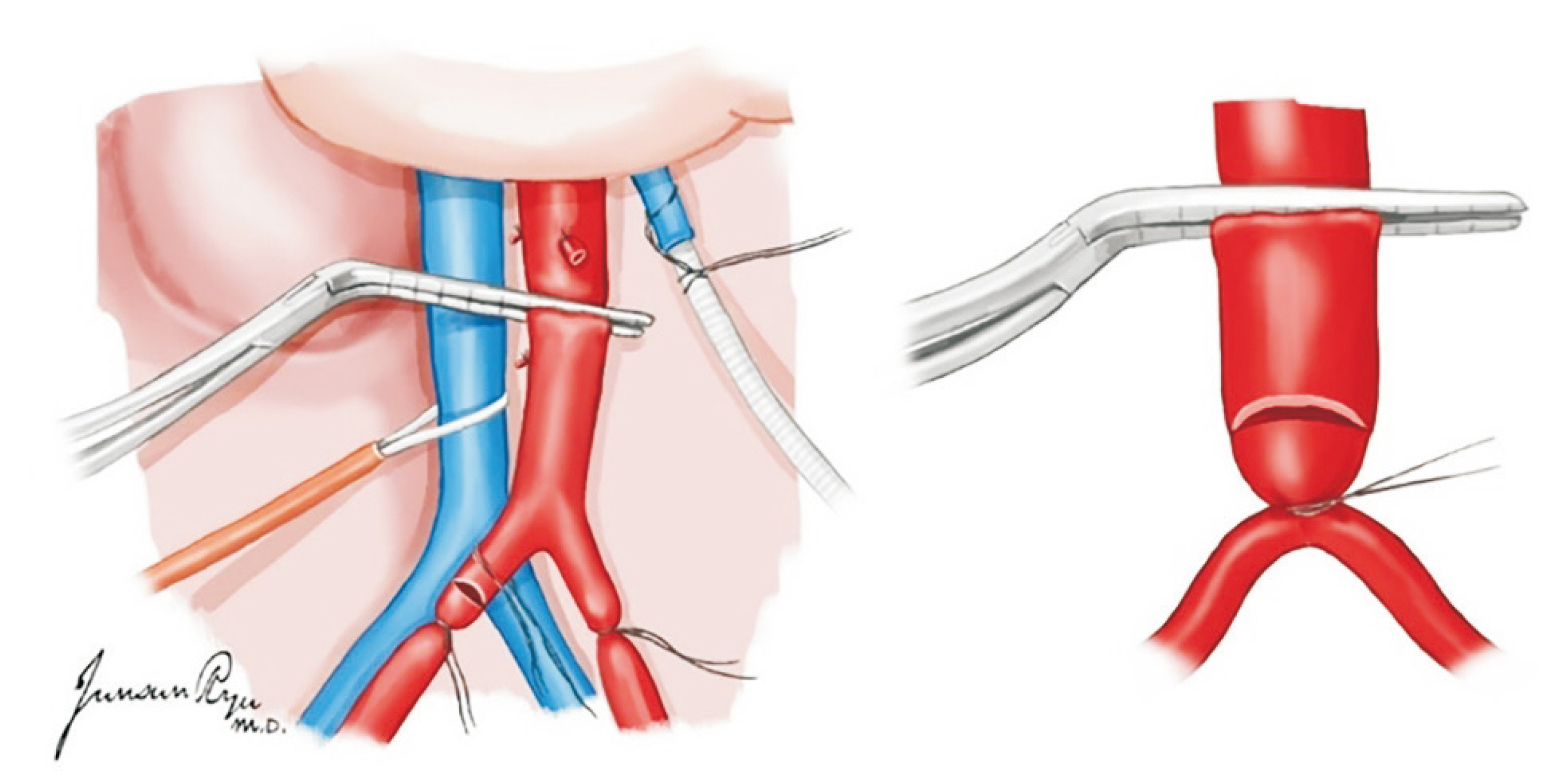
Fig. 10 A vascular clamp is placed onto the aorta approximately 5 cm proximally to this tie to block the blood flow to this segment of the aorta where an arteriotomy is made. After systemic heparinization (300 units/kg) is performed, the distal aorta is ligated, and a 24-Fr aortic cannula is placed at this site.

Fig. 11 The inferior mesenteric vein is ligated, and a 14-Fr perfusion cannula is placed.

Fig. 12 The portal vein is divided at the level of 1–2 cm proximal to the junction of the splenic vein and superior mesenteric vein (SMV) if the pancreas is retrieved for transplantation. Otherwise, the division can be at the level of the confluence of the splenic vein and SMV.
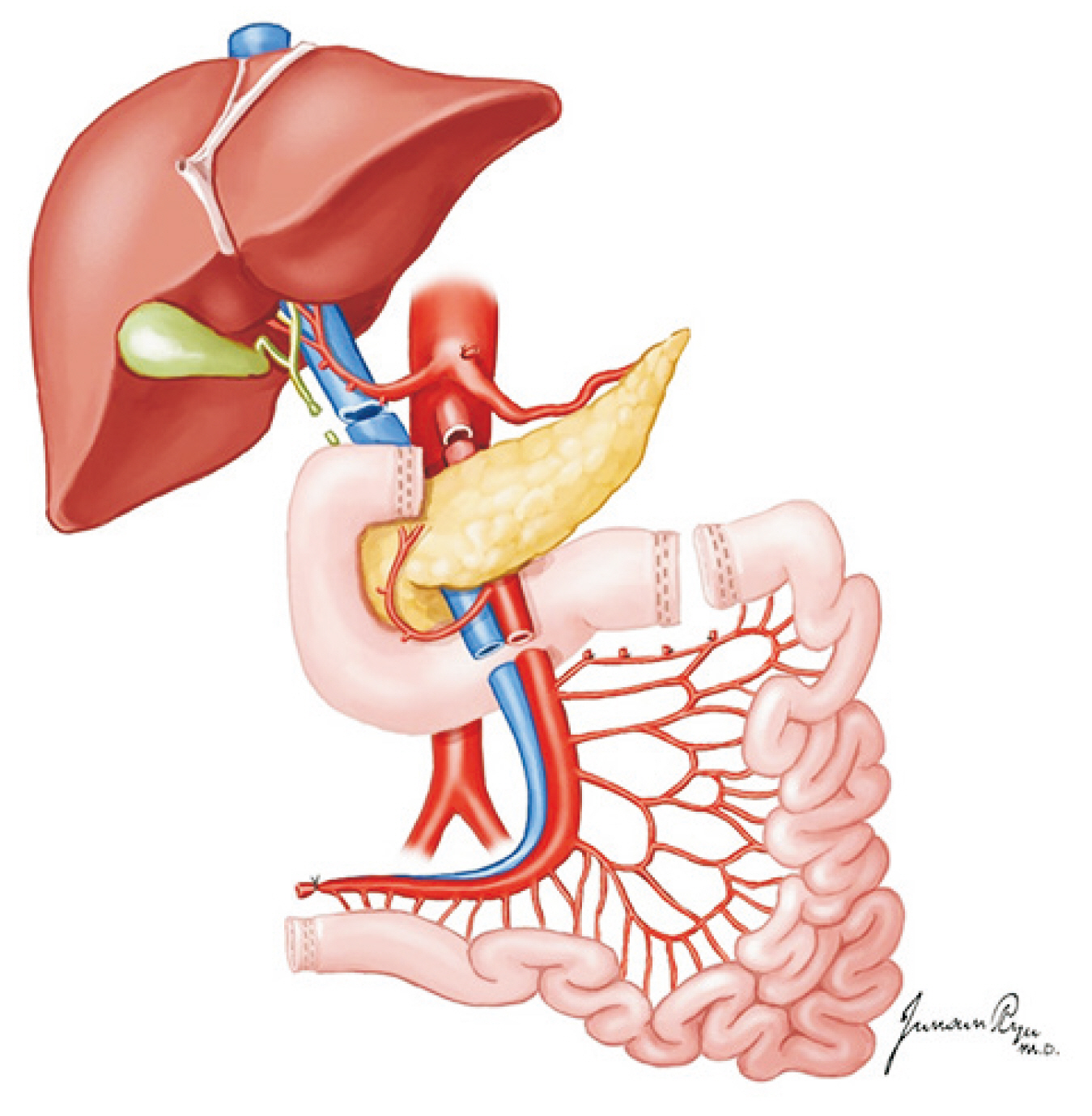
Fig. 13 Level of the transection for small bowel procurement.

Fig. 14 The surgical stapling device is placed immediately below the middle colic vessels.

Fig. 15 The greater omentum is separated from the transverse colon to open the lesser sac, and the whole pancreas is exposed for evaluation.
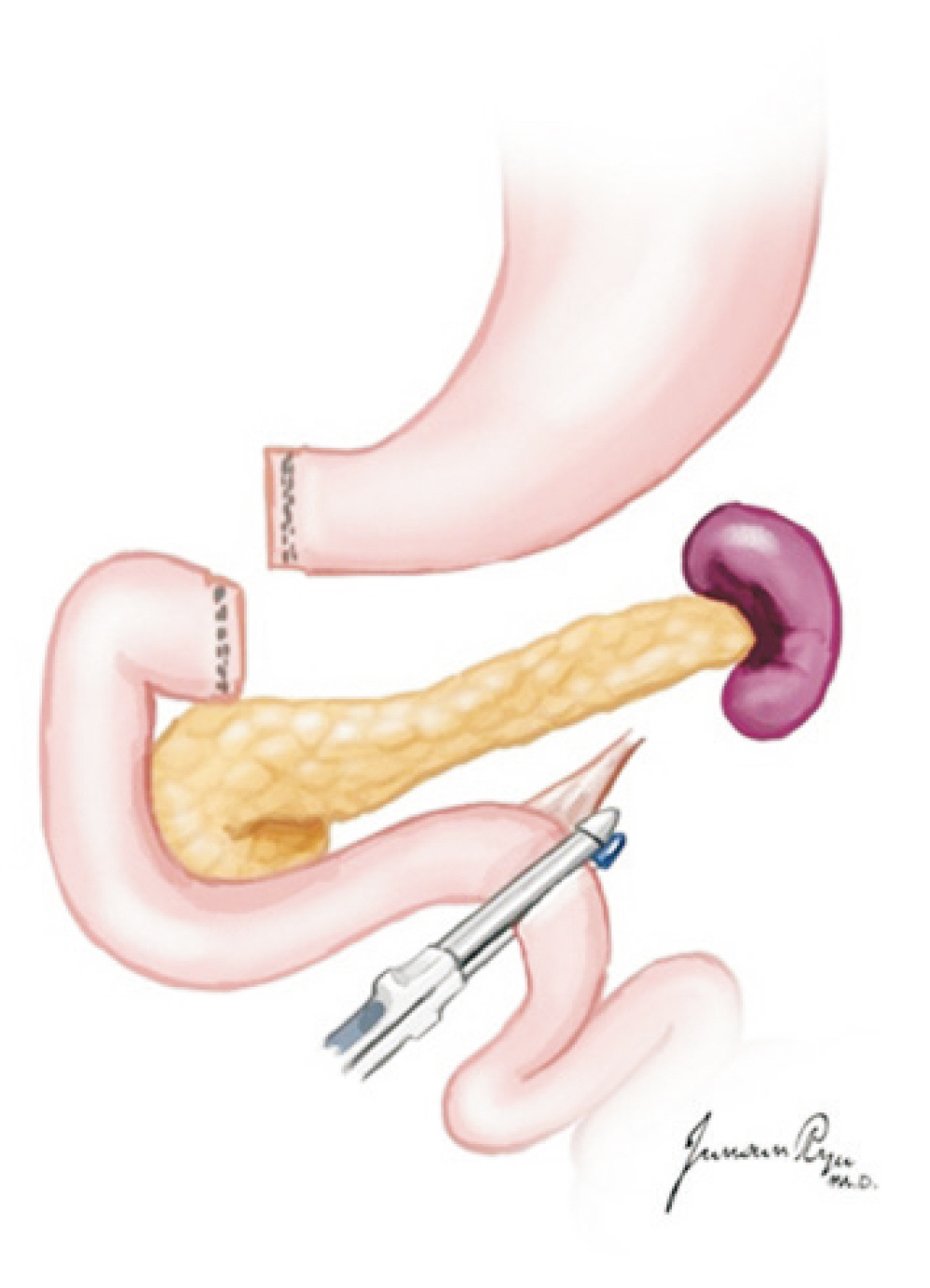
Fig. 16 The first portion of the duodenum is circumferentially dissected, and a mechanical stapler is used to divide the duodenum from the stomach just distal to the pylorus. The stapler is also used to divide the duodenum just distal to the ligament of Treitz.

Fig. 17 The superior mesenteric artery (SMA) is separated at its origin from the aorta. During the separation of the SMA, caution should be taken not to injure the renal arteries.
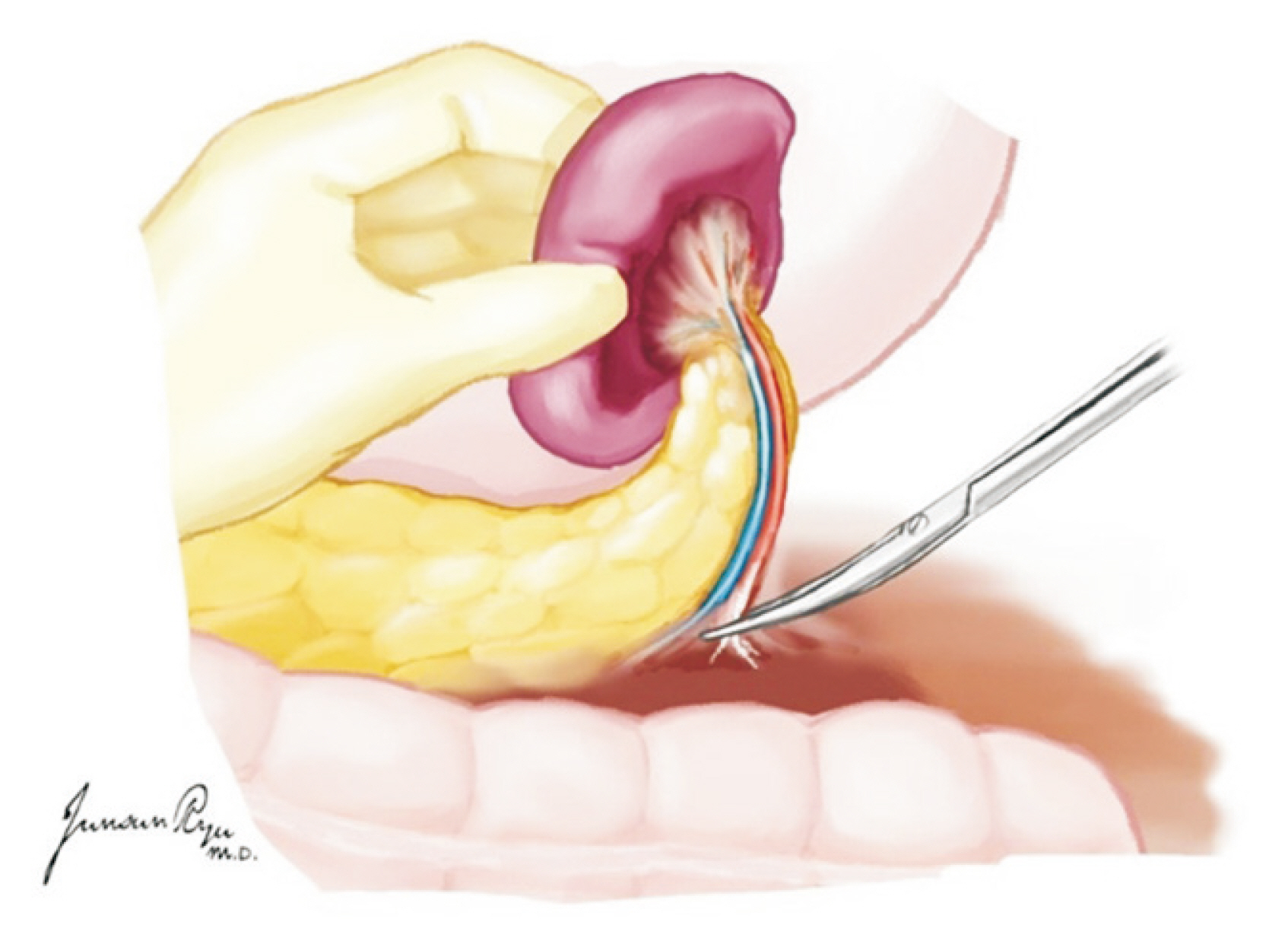
Fig. 18 While the spleen is held in the supporting hand, the distal pancreas and spleen are separated from adjacent tissues.
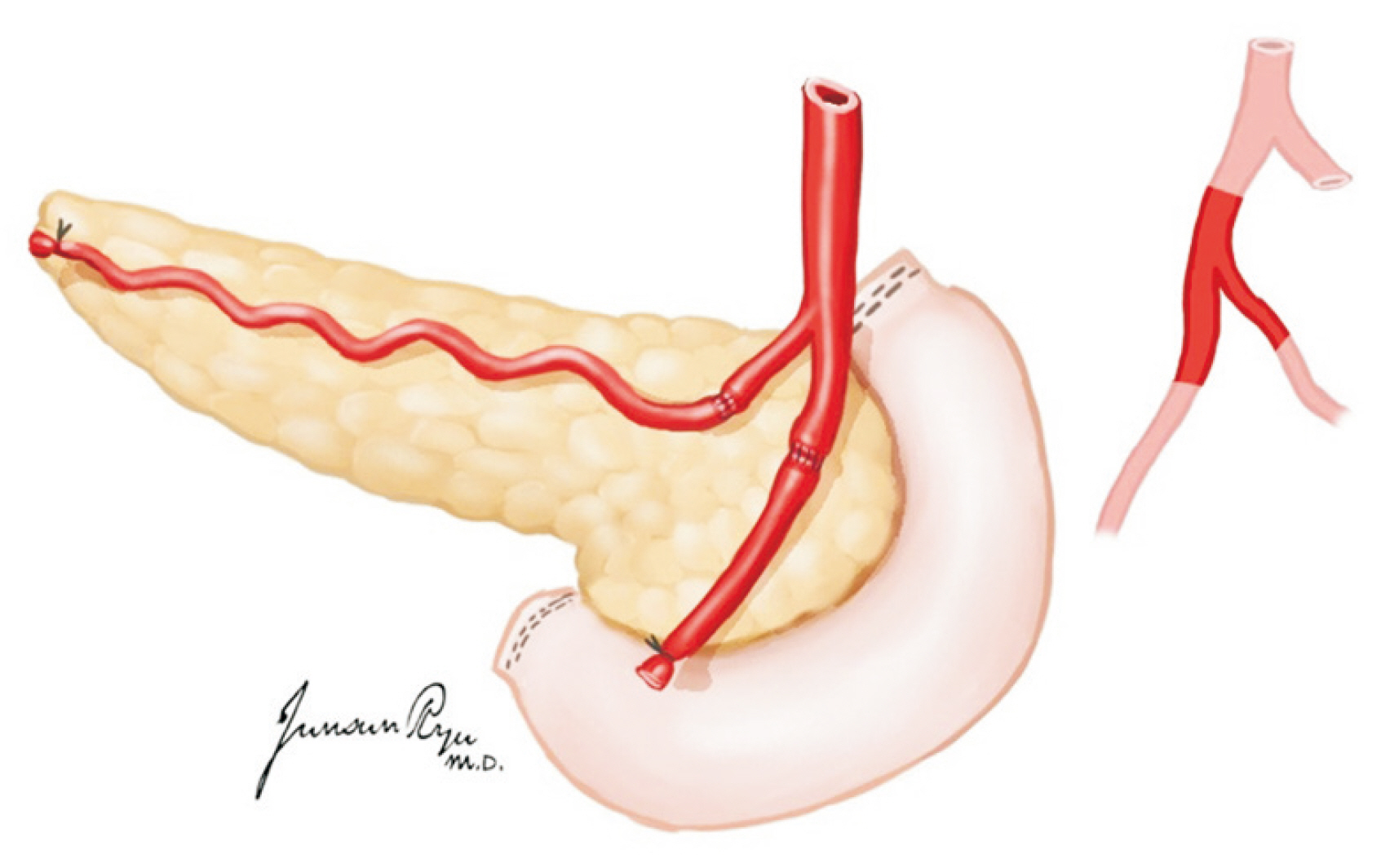
Fig. 19 The procurement of the common, external, and internal iliac arteries is performed for Y-graft interposition at the time of back-table procedures.
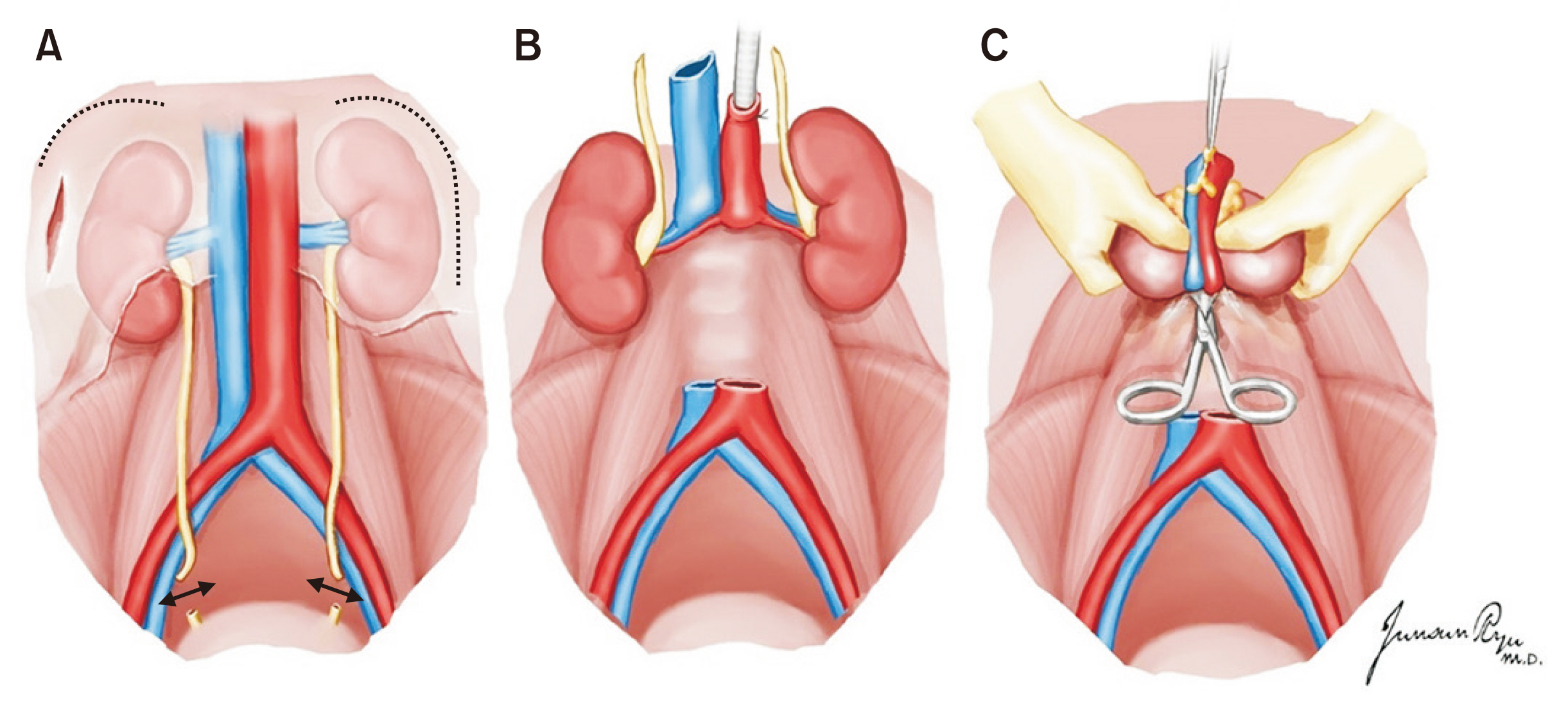
Fig. 20 The two kidneys are removed en bloc with the cava and aorta. The lateral attachments of the kidney is divided, and the ureters are traced caudally and transected distally near the bladder junction (A). The aorta and inferior vena cava are divided at their bifurcations. The ureters and these vessels are retracted cephalad and anteriorly, along with the two kidneys (B), and dissection proceeds along their posterior aspects, anterior to the surface of the vertebral bodies and psoas muscle (C).

Fig. 21 The left renal vein is identified and divided at its junction with the inferior vena cava.

Fig. 22 The aortic wall is divided longitudinally down its center aspect, which allows for inspection of the renal artery orifices.
Reference
-
1. Dare AJ, Bartlett AS, Fraser JF. 2012; Critical care of the potential organ donor. Curr Neurol Neurosci Rep. 12:456–65. DOI: 10.1007/s11910-012-0272-9. PMID: 22618126.
Article2. Patel MS, Abt PL. 2019; Current practices in deceased organ donor management. Curr Opin Organ Transplant. 24:343–50. DOI: 10.1097/MOT.0000000000000638. PMID: 31090647.
Article3. Souter MJ, Eidbo E, Findlay JY, Lebovitz DJ, Moguilevitch M, Neidlinger NA, et al. 2018; Organ donor management: part 1. toward a consensus to guide anesthesia services during donation after brain death. Semin Cardiothorac Vasc Anesth. 22:211–22. DOI: 10.1177/1089253217749053. PMID: 29276852.
Article4. van Erp AC, van Dullemen LF, Ploeg RJ, Leuvenink HG. 2018; Systematic review on the treatment of deceased organ donors. Transplant Rev (Orlando). 32:194–206. DOI: 10.1016/j.trre.2018.06.001. PMID: 30049604.
Article5. Chamorro-Jambrina C, Muñoz-Ramírez MR, Martínez- Melgar JL, Pérez-Cornejo MS. 2017; Organ donor management: eight common recommendations and actions that deserve reflection. Med Intensiva. 41:559–68. DOI: 10.1016/j.medin.2017.01.012. PMID: 28318674.
Article6. Chudoba P, Krajewski W, Wojciechowska J, Kamińska D. 2017; Brain death-associated pathological events and therapeutic options. Adv Clin Exp Med. 26:1457–64. DOI: 10.17219/acem/65068. PMID: 29442469.
Article7. Opdam HI. 2019; Hormonal therapy in organ donors. Crit Care Clin. 35:389–405. DOI: 10.1016/j.ccc.2018.11.013. PMID: 30784617.
Article8. Berthelsen PG, Marik PE. 2015; Therapeutic hypothermia in deceased organ donors and kidney-graft function. N Engl J Med. 373:2686. DOI: 10.1056/NEJMc1511744. PMID: 27186763.
Article9. Miñambres E, Pérez-Villares JM, Chico-Fernández M, Zabalegui A, Dueñas-Jurado JM, Misis M, et al. 2015; Lung donor treatment protocol in brain dead-donors: a multicenter study. J Heart Lung Transplant. 34:773–80. DOI: 10.1016/j.healun.2014.09.024. PMID: 25447580. PMCID: PMC6988327.
Article10. Nguyen DC, Loor G, Carrott P, Shafii A. 2019; Review of donor and recipient surgical procedures in lung transplantation. J Thorac Dis. 11(Suppl 14):S1810–6. DOI: 10.21037/jtd.2019.06.31. PMID: 31632758. PMCID: PMC6783720.
Article11. Inci I. 2017; Donors after cardiocirculatory death and lung transplantation. J Thorac Dis. 9:2660–9. DOI: 10.21037/jtd.2017.07.82. PMID: 28932573. PMCID: PMC5594200.
Article12. de Perrot M, Fischer S, Liu M, Jin R, Bai XH, Waddell TK, et al. 2001; Prostaglandin E1 protects lung transplants from ischemia-reperfusion injury: a shift from pro- to anti-inflammatory cytokines. Transplantation. 72:1505–12. DOI: 10.1097/00007890-200111150-00006. PMID: 11707737.13. Oto T, Rabinov M, Negri J, Marasco S, Rowland M, Pick A, et al. 2006; Techniques of reconstruction for inadequate donor left atrial cuff in lung transplantation. Ann Thorac Surg. 81:1199–204. DOI: 10.1016/j.athoracsur.2005.11.057. PMID: 16564243.
Article14. Slama A, Schillab L, Barta M, Benedek A, Mitterbauer A, Hoetzenecker K, et al. 2017; Standard donor lung procurement with normothermic ex vivo lung perfusion: a prospective randomized clinical trial. J Heart Lung Transplant. 36:744–53. DOI: 10.1016/j.healun.2017.02.011. PMID: 28314503.
Article15. Huddleston CB, Richey SR. 2014; Heart-lung transplantation. J Thorac Dis. 6:1150–8. DOI: 10.3109/9781420019285-5. PMID: 23456080.16. Yu HC, Cho BH. 2006; How to do I make an organ procurement in deceased donor? J Korean Soc Transplant. 20:14–24.17. Choi YR, Lee KW. 2015; Liver procurement. J Korean Soc Transplant. 29:109–17. DOI: 10.4285/jkstn.2015.29.3.109.
Article18. Keutgen XM, Petrowsky H. 2014; Procurement for visceral organ transplantation: where to cannulate and how to perfuse? Curr Opin Organ Transplant. 19:92–9. DOI: 10.1097/MOT.0000000000000066. PMID: 24565959.19. Makowka L, Stieber AC, Sher L, Kahn D, Mieles L, Bowman J, et al. 1988; Surgical technique of orthotopic liver transplantation. Gastroenterol Clin North Am. 17:33–51.
Article20. Nickkholgh A, Contin P, Abu-Elmagd K, Golriz M, Gotthardt D, Morath C, et al. 2013; Intestinal transplantation: review of operative techniques. Clin Transplant. 27 Suppl 25:56–65. DOI: 10.1111/ctr.12190. PMID: 23909503.
Article21. Wunderlich H, Brockmann JG, Voigt R, Rauchfuss F, Pascher A, Brose S, et al. 2011; DTG procurement guidelines in heart beating donors. Transpl Int. 24:733–57. DOI: 10.1111/j.1432-2277.2011.01266.x. PMID: 21668528.
Article22. Humar A, Payne WD, Matas AJ. 2006. Atlas of organ transplantation. Springer;London, UK: DOI: 10.1007/978-1-84628-316-1.23. Yersiz H, Renz JF, Hisatake GM, Gordon S, Saggi BH, Feduska NJ Jr, et al. 2003; Multivisceral and isolated intestinal procurement techniques. Liver Transpl. 9:881–6. DOI: 10.1053/jlts.2003.50155. PMID: 12884206. PMCID: PMC6445255.
Article24. Hakim NS SR, Gray D, Friend P, Colman A. 2010. Pancreas, islet and stem cell transplantation for diabetes. 2nd ed. Oxford University Press;Oxford, UK: DOI: 10.1093/med/9780199565863.001.0001.25. Yang HC, Gifford RR, Dafoe DC, Neumyer MM, Thiele BL. 1991; Arterial reconstruction of the pancreatic allograft for transplantation. Am J Surg. 162:262–4. DOI: 10.1016/0002-9610(91)90083-P. PMID: 1928589.
Article26. Morris PJ, Tilney NL, editors. PM. 1984. Techniques of multiple organ harvesting. Progress in transplantation. Edinburgh. Churchill Livingstone;burgh, UK:27. Knechtle S, Morris P. 2008. Kidney transplantation. 6th ed. Saunders Elsevier;Philadelphia, PA:
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Activation Policy for Brain-dead Organ Donation
- Optimal System for Deceased Organ Donation and Procurement in Korea
- How to Do I Make an Organ Procurement in Deceased Donor?
- Current Status of Deceased Donor Organ Recovery and Sharing in Korea
- Donor Selection, Management, and Procurement for Lung Transplantation
