Pneumothorax Following Gastric Endoscopic Mucosal Resection
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Dong-A University Hospital, Busan, Korea
- KMID: 2505870
- DOI: http://doi.org/10.4166/kjg.2020.76.2.83
Abstract
- An endoscopic mucosal resection (EMR) is used widely as an alternative treatment to a surgical resection for early gastric neoplasticlesions. Among the unusual complications of gastric EMR, perforation is usually manifested as a pneumoperitoneum. Thispaper reports a patient with a left-side pneumothorax without pneumoperitoneum as a complication of gastric EMR. The patientdeveloped a left side pneumothorax after gastric EMR in the gastric fundus and recovered without further complications afterconservative treatment, including endoscopic clipping.
Figure
-
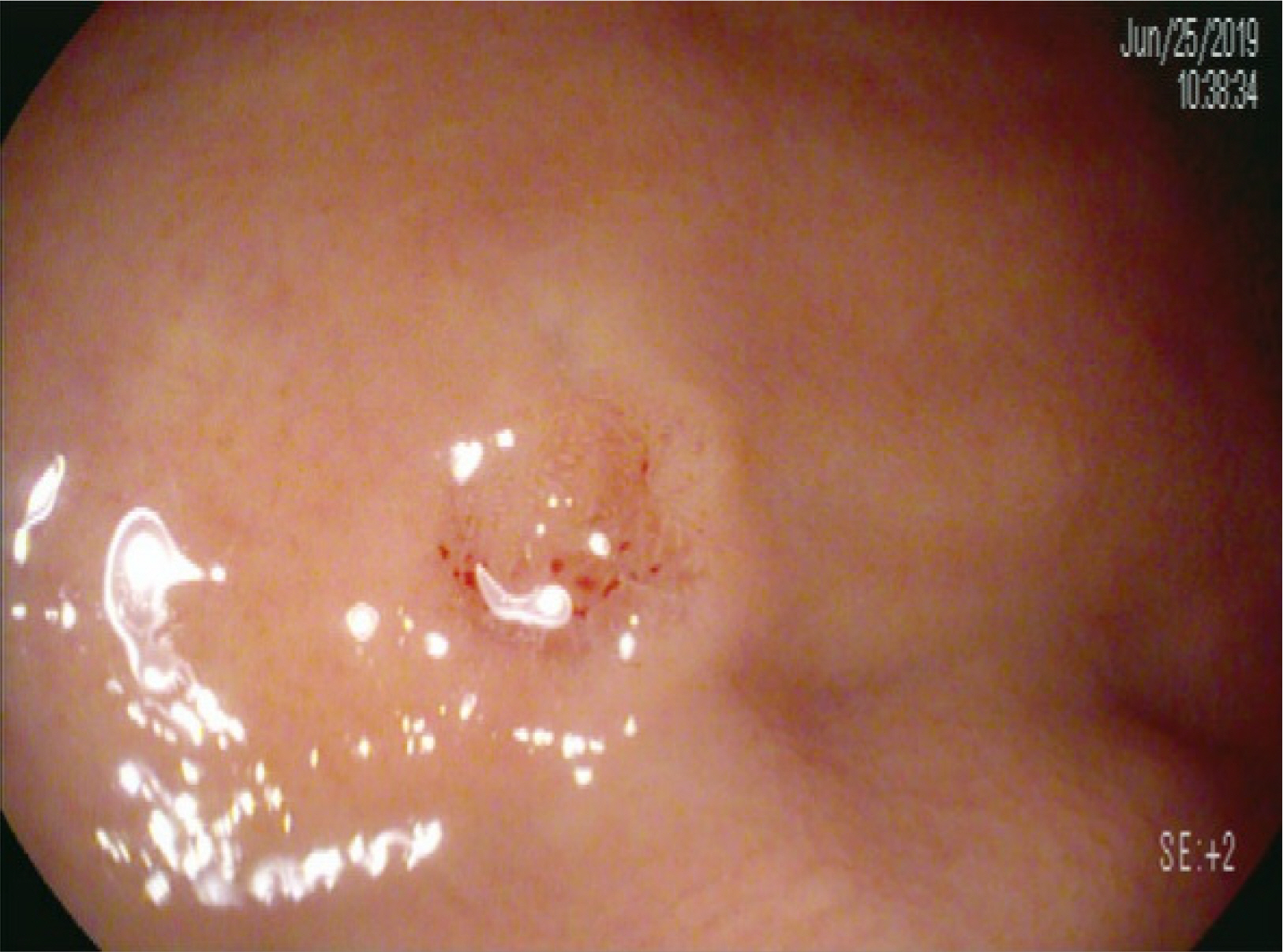
Fig. 1 Endoscopic finding of the patient before the procedure. The lesion (tubular adenoma, type IIa+IIc, 10×10 mm in diameter) was located at the fundus of the stomach.

Fig. 2 Endoscopic findings of the patient during the procedure. (A) After confirming the lesion boundary, marking was performed using an endoscopic dual knife. (B) After the endoscope equipped with the endoscopic band ligation equipment was inserted to allow the entire lesion to fit inside the rubber band, the lesion was completely ligated into the band after inhalation. (C) Resection was performed using a snare.
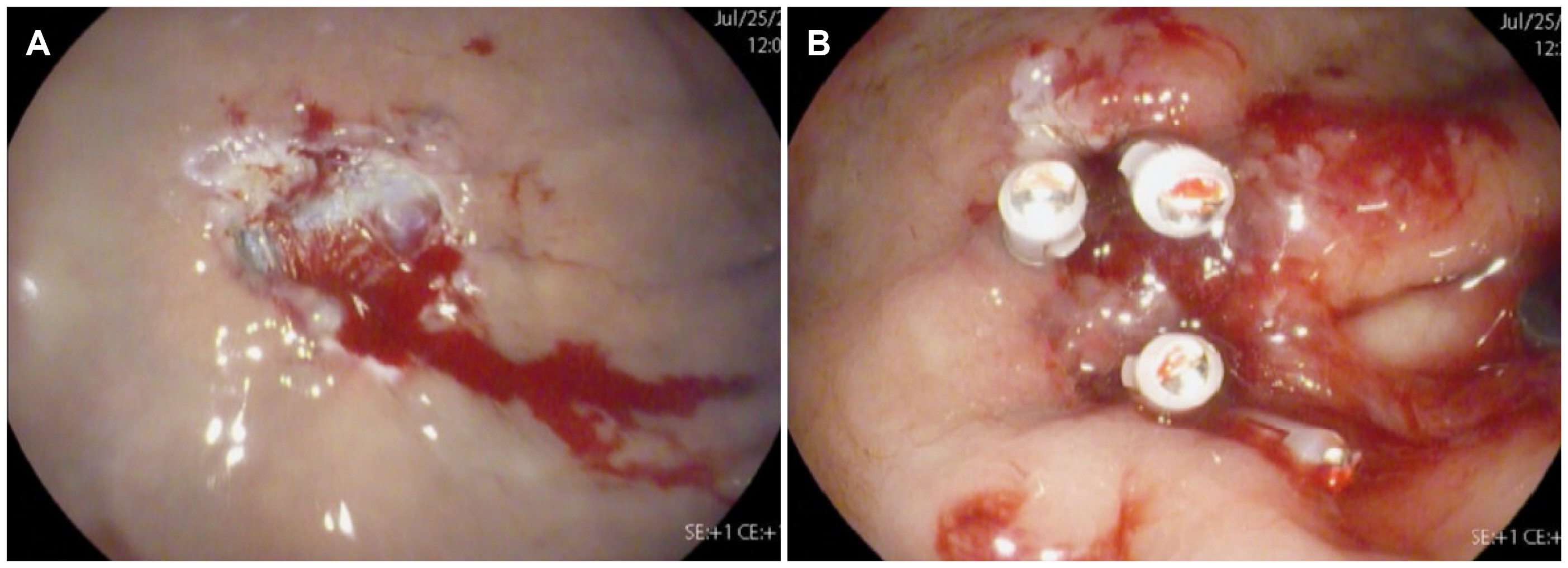
Fig. 3 Endoscopic findings of the patient after the procedure. (A) No definite perforating hole was seen immediately after the endoscopic mucosal resection, but a deep muscular site was exposed, and there was bleeding from vascular exposure. (B) Endoscopic clipping was performed at the suspicious micro-perforated site.

Fig. 4 Plain chest and abdominal radiographs. (A) Plain chest radiography performed immediately after the endoscopic mucosal resection (EMR). This panel shows the left-sided pneumothorax and no free air at both sub-diaphragm. (B) Plain abdominal radiography performed immediately after the EMR. This panel shows no gas within the peritoneal space. (C) Plain chest radiography taken the day after EMR. This photograph shows an improved pneumothorax without a chest tube.

Fig. 5 Follow-up endoscopy findings. (A) The micro-perforated site had completely healed with a scar and two hemo-clips two months later. (B) After six months, the post- endoscopic mucosal resection site area had completely healed with scars.
Reference
-
1. Ko WJ, Song GW, Kim WH, Hong SP, Cho JY. 2016; Endoscopic resection of early gastric cancer: current status and new approaches. Transl Gastroenterol Hepatol. 1:24. DOI: 10.21037/tgh.2016.03.22. PMID: 28138591. PMCID: PMC5244754.
Article2. Oda I, Gotoda T, Hamanaka H, et al. 2005; Endoscopic submucosal dissection for early gastric cancer: technical feasibility, operation time and complications from a large consecutive series. Dig Endosc. 17:54–58. DOI: 10.1111/j.1443-1661.2005.00459.x.
Article3. Lee YR, Heo J, Jung MK, et al. 2015; A case of pneumothorax following gastric endoscopic submucosal dissection. Korean J Med. 88:54–59. DOI: 10.3904/kjm.2015.88.1.54.
Article4. Kang KJ, Lee JH. 2010; Characteristics of gastric cancer in Korea-with an emphasis on the increase of the early gastric cancer (EGC). J Korean Med Assoc. 53:283–305. DOI: 10.5124/jkma.2010.53.4.283.5. Choi KS, Jung HY. 2010; Endoscopic resection of early gastric cancer. J Korean Med Assoc. 53:299–305. DOI: 10.5124/jkma.2010.53.4.299.
Article6. Gotoda T, Yanagisawa A, Sasako M, et al. 2000; Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer. 3:219–225. DOI: 10.1007/PL00011720. PMID: 11984739.
Article7. Choi KD. 2011; Endoscopic resection of early gastric cancer. Korean J Med. 81:40–46. DOI: 10.5772/24614.
Article8. Meng FS, Zhang ZH, Wang YM, Lu L, Zhu JZ, Ji F. 2016; Comparison of endoscopic resection and gastrectomy for the treatment of early gastric cancer: a meta-analysis. Surg Endosc. 30:3673–3683. DOI: 10.1007/s00464-015-4681-0. PMID: 26659235.
Article9. Saito I, Tsuji Y, Sakaguchi Y, et al. 2014; Complications related to gastric endoscopic submucosal dissection and their managements. Clin Endosc. 47:398–403. DOI: 10.5946/ce.2014.47.5.398. PMID: 25324997. PMCID: PMC4198554.
Article10. Soetikno RM, Gotoda T, Nakanishi Y, Soehendra N. 2003; Endoscopic mucosal resection. Gastrointest Endosc. 57:567–579. DOI: 10.1067/mge.2003.130. PMID: 12665775.
Article11. Yoo JH, Shin SJ, Lee KM, et al. 2012; Risk factors for perforations associated with endoscopic submucosal dissection in gastric lesions:emphasis on perforation type. Surg Endosc. 26:2456–2464. DOI: 10.1007/s00464-012-2211-x. PMID: 22398962.12. Lee DW, Jeon SW. 2012; Management of complications during gastric endoscopic submucosal dissection. Diagn Ther Endosc. 2012:624835. DOI: 10.1155/2012/624835. PMID: 23091341. PMCID: PMC3471425.
Article13. Ono H, Kondo H, Gotoda T, et al. 2001; Endoscopic mucosal resection for treatment of early gastric cancer. Gut. 48:225–229. DOI: 10.1136/gut.48.2.225. PMID: 11156645. PMCID: PMC1728193.
Article14. Kim GJ, Park SM, Kim JS, Ji JS, Kim BW, Choi H. 2017; Risk factors for additional surgery after iatrogenic perforations due to endoscopic submucosal dissection. Gastroenterol Res Pract. 2017:6353456. DOI: 10.1155/2017/6353456. PMID: 28316622. PMCID: PMC5338066.
Article15. Kim YJ, Park DK. 2011; Management of complications following endoscopic submucosal dissection for gastric cancer. World J Gastrointest Endosc. 3:67–70. DOI: 10.4253/wjge.v3.i4.67. PMID: 21603034. PMCID: PMC3098436.
Article16. Mannath J, Ragunath K. 2011; Endoscopic mucosal resection: who and how? Therap Adv Gastroenterol. 4:275–282. DOI: 10.1177/1756283X10388683. PMID: 21941594. PMCID: PMC3165204.
Article17. Neofytou K, Petrou A, Savva C, et al. 2013; Pneumothorax following ERCP: report of two cases with different pathophysiology. Case Rep Med. 2013:206564. DOI: 10.1155/2013/206564. PMID: 23864863. PMCID: PMC3707261.
Article18. Pourmand A, Shokoohi H. 2013; Tension pneumothorax, pneumoperitoneum, and cervical emphysema following a diagnostic colonoscopy. Case Rep Emerg Med. 2013:583287. DOI: 10.1155/2013/583287. PMID: 23819071. PMCID: PMC3683440.
Article19. Loiselle A, Parish JM, Wilkens JA, Jaroszewski DE. 2013; Managing iatrogenic pneumothorax and chest tubes. J Hosp Med. 8:402–408. DOI: 10.1002/jhm.2053. PMID: 23765922.
Article20. MacDuff A, Arnold A, Harvey J. BTS Pleural Disease Guideline Group. 2010; Management of spontaneous pneumothorax: British thoracic society pleural disease guideline 2010. Thorax. 65(Suppl 2):ii18–ii31. DOI: 10.1136/thx.2010.136986. PMID: 20696690.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Histological Comparison of Endoscopic Forceps Biopsy with Endoscopic Resection in Gastric Mucosal Elevated Lesion
- Follow-up of endoscopic mucosal resection for gastric adenoma and early gastric cancer
- Clinicopathologic Evaluation of Endoscopic Mucosal Resection of Early Gastric Carcinomas and Gastric Adenomas
- Endoscopic Management of Gastric Subepithelial Tumor
- Endoscopic Treatment for Early Gastric Cancer
