Unilateral Diaphragm Paralysis Associated With Neurosyphilis: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea
- 2Department of Pulmonology, Allergy and Critical Care Medicine, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea
- 3Department of Ophthalmology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea
- KMID: 2505394
- DOI: http://doi.org/10.5535/arm.19216
Abstract
- Diaphragm dysfunction can originate from various etiologies, and bilaterality of the dysfunction depends on the cause. Symptoms of diaphragm dysfunction vary depending on the degree of phrenic nerve denervation, spinal cord lesion, and involvement of the diaphragm. Several infectious diaphragmatic dysfunctions have been reported, including the human immunodeficiency virus, poliovirus, West Nile virus, and dengue virus. Here, we report a case of unilateral diaphragm paralysis in a 34-year-old man with neurosyphilis.
Keyword
Figure
-
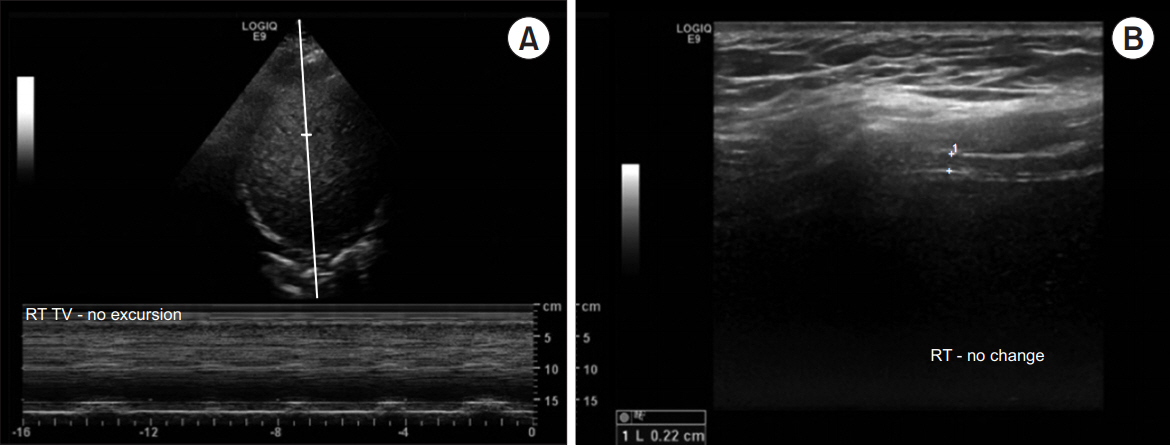
Fig. 1. Initial ultrasonography of the right diaphragm. Ultrasonography was performed in two different views. The hyperechoic right diaphragm in the 7th intercostal space was identified at the distal end of the liver, which served as an acoustic window. (A) The excursion of the diaphragm was viewed through M-mode and there was no movement of the right diaphragm. (B) The thickness of the right diaphragm is viewed through B-mode and the value revealed 0.22 cm.
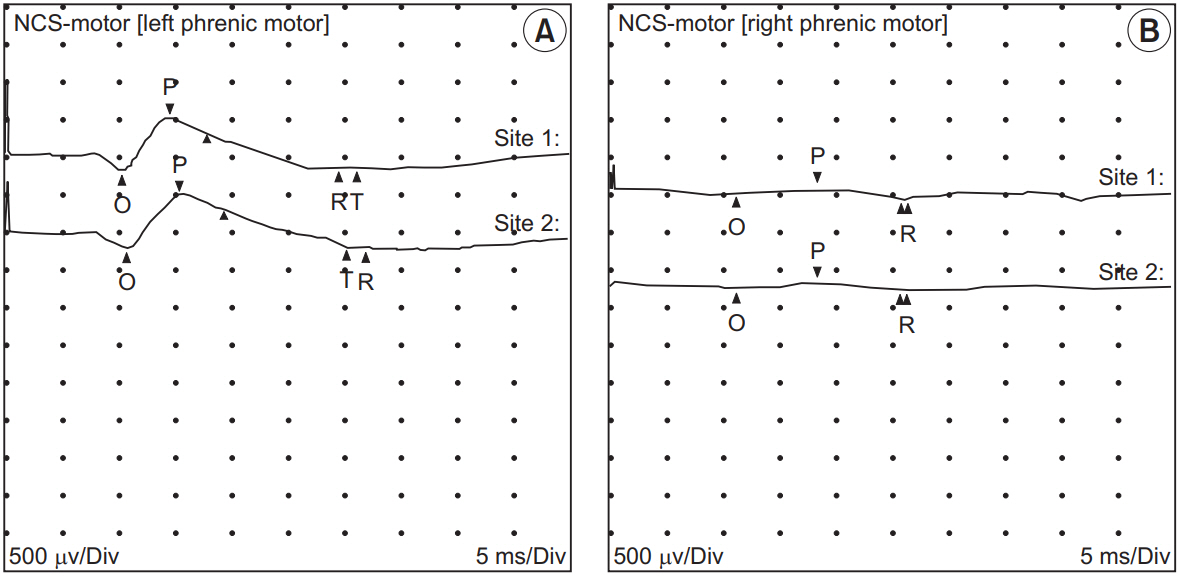
Fig. 2. Nerve conduction studies of (A) right and (B) left phrenic nerves. The compound muscle action potential of the right phrenic nerve showed a decreased amplitude (0.1 mV), while the left showed a normal amplitude (0.7 mV).
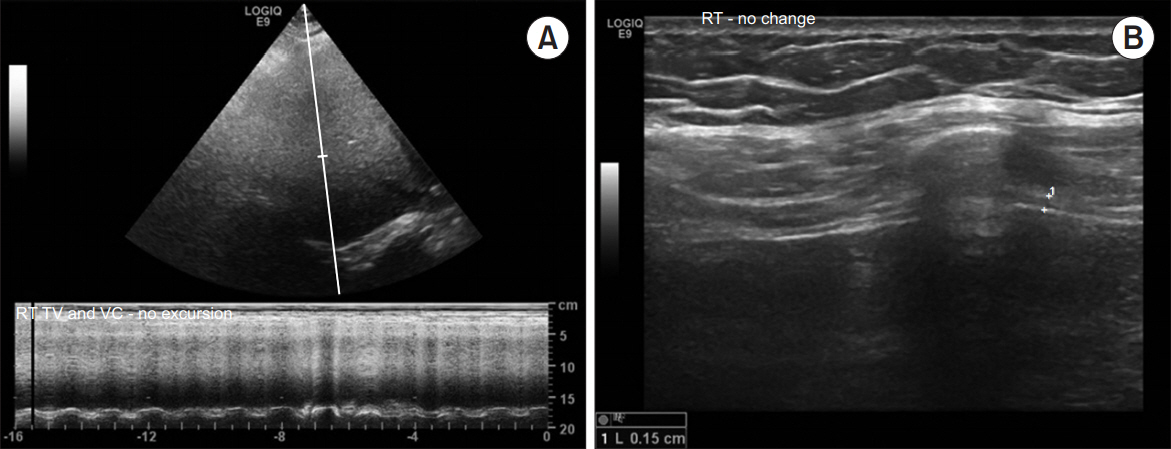
Fig. 3. Follow-up ultrasonography of the right diaphragm. (A) The follow-up ultrasonography after 2 months showed a paradoxical movement of the right diaphragm, which indicated complete paralysis. (B) The thickness of the right diaphragm revealed 0.15 cm.
Reference
-
1. Rudrappa M, Kokatnur L, Chernyshev O. Neurological respiratory failure. Diseases. 2018; 6:7.
Article2. Ratnayake EC, Shivanthan C, Wijesiriwardena BC. Diaphragmatic paralysis: a rare consequence of dengue fever. BMC Infect Dis. 2012; 12:46.
Article3. Betensley AD, Jaffery SH, Collins H, Sripathi N, Alabi F. Bilateral diaphragmatic paralysis and related respiratory complications in a patient with West Nile virus infection. Thorax. 2004; 59:268–9.
Article4. Brage D. Unilateral paralysis of the phrenic nerve of syphilitic origin. Sem Med. 1956; 108:939–43.5. Riley EA. Idiopathic diaphragmatic paralysis; a report of eight cases. Am J Med. 1962; 32:404–16.6. Briscoe C. The diagnosis of unilateral phrenic nerve paralysis: an important point in mediastinal localization. Lancet. 1925; 205:376–81.7. Mindel A, Tovey SJ, Timmins DJ, Williams P. Primary and secondary syphilis, 20 years’ experience. 2. Clinical features. Genitourin Med. 1989; 65:1–3.
Article8. Ricoy J, Rodriguez-Nunez N, Alvarez-Dobano JM, Toubes ME, Riveiro V, Valdes L. Diaphragmatic dysfunction. Pulmonology. 2019; 25:223–35.
Article9. Piliero PJ, Estanislao L, Simpson D. Diaphragmatic paralysis due to isolated phrenic neuropathy in an HIV-infected man. Neurology. 2004; 62:154–5.
Article10. Faul JL, Ruoss S, Doyle RL, Kao PN. Diaphragmatic paralysis due to Lyme disease. Eur Respir J. 1999; 13:700–2.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sonographic evaluation of the diaphragm in patients with unilateral diaphragmatic paralysis
- A Case of Diaphragmatic Eventration Complicated with Contralateral Traumatic Diaphragmatic Paralysis
- A Case of Unilateral Diaphragmatic Paralysis with Brachial Plexus Palsy in the Neonate
- Stuttering Priapism in a Patient with Neurosyphilis
- Diagnosis of diaphragmatic paralysis using ultrasound in a cervical herpes zoster patient: A case report
