Endoscopic Self-Expandable Metal Stent Placement for Malignant Afferent Loop Obstruction After Pancreaticoduodenectomy: A Case Series and Review
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Kobe University Graduate School of Medicine, Kobe, Japan
- 2Department of Gastroenterology, Kitaharima Medical Center, Ono, Japan
- KMID: 2504955
- DOI: http://doi.org/10.5946/ce.2019.145
Abstract
- In this study, we assessed a series of our cases in which endoscopic self-expandable metal stents (SEMSs) were used to treat malignant afferent loop obstruction (ALO) that arose after pancreaticoduodenectomy (PD). We retrospectively examined the records of 7 patients who underwent endoscopic SEMS placement for malignant ALO following PD. Clinical success was achieved in all cases. The median procedure time was 30 min (range, 15–50 min). There were no cases of stent occlusion, and no procedure-related adverse events were encountered. All patients died of their primary disease, and the median overall survival period was 155 days (range, 96–374 days). A re-intervention involving endoscopic ultrasound-guided hepaticogastrostomy combined with antegrade stenting was performed for obstructive jaundice and acute cholangitis in 1 case. In conclusion, endoscopic SEMS placement may be an effective and safe treatment for malignant ALO that arises after PD.
Keyword
Figure
-
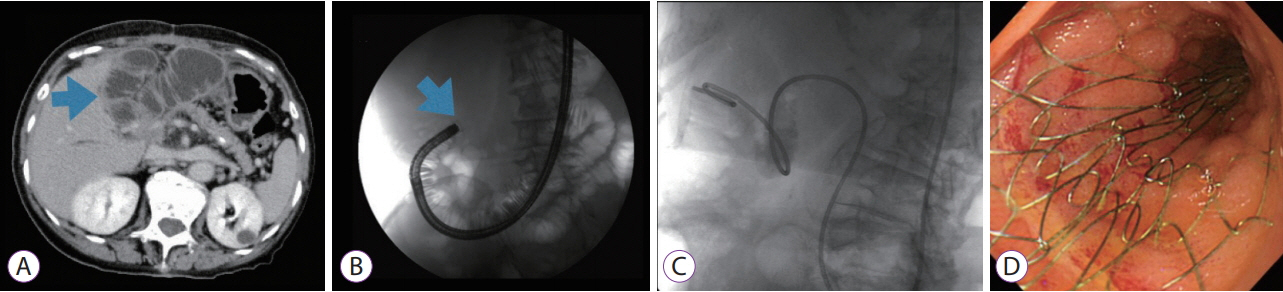
Fig. 1. (A) A computed tomography scan revealed marked distention of the afferent loop, which was suggestive of bowel obstruction caused by a recurrent tumor. (B) An endoscope was inserted into the afferent loop. A neoplastic stenotic lesion blocked further passage of the endoscope. (C) A nasojejunal tube was placed over a guidewire to decompress the dilated afferent loop. (D) A self-expandable metal stent was inserted using the standard through-the-scope technique.

Fig. 2. (A) Case 2 presented with obstructive jaundice due to invasive cancer involving a bilioenteric anastomosis after self-expandable metal stent (SEMS) insertion. (B) Endoscopic ultrasound-guided biliary drainage was selected. An echoendoscope was advanced into the stomach, and a 19-gauge fine needle aspiration needle was advanced into a left-sided intrahepatic bile duct (B3). Cholangiography showed stenosis of the bilioenteric anastomosis, and a guidewire was advanced through the stenotic lesion and into the afferent loop. (C) An uncovered SEMS was placed across the stenotic lesion, and a plastic stent was placed through the fistula between the gastric body and the intrahepatic bile duct.
Cited by 1 articles
-
Endoscopic Ultrasound-Guided Gastroenterostomy for Afferent Loop Syndrome
Hideyuki Shiomi, Arata Sakai, Ryota Nakano, Shogo Ota, Takashi Kobayashi, Atsuhiro Masuda, Hiroko Iijima
Clin Endosc. 2021;54(6):810-817. doi: 10.5946/ce.2021.234.
Reference
-
1. Chevallier P, Novellas S, Motamedi JP, Gugenheim J, Brunner P, Bruneton JN. Percutaneous jejunostomy and stent placement for treatment of malignant Roux-en-Y obstruction: a case report. Clin Imaging. 2006; 30:283–286.
Article2. Sakai A, Shiomi H, Okabe Y, et al. Effectiveness of endoscopic self-expandable metal stent placement for afferent loop obstruction caused by pancreatic cancer recurrence after pancreaticoduodenectomy. Clin J Gastroenterol. 2015; 8:103–107.
Article3. Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010; 71:446–454.
Article4. Morita S, Takemura T, Matsumoto S, Odani R. Septic shock after percutaneous transhepatic drainage of obstructed afferent loop: case report. Cardiovasc Intervent Radiol. 1989; 12:66–68.
Article5. Burdick JS, Garza AA, Magee DJ, Dykes C, Jeyarajah R. Endoscopic management of afferent loop syndrome of malignant etiology. Gastrointest Endosc. 2002; 55:602–605.
Article6. Kim JK, Park CH, Huh JH, et al. Endoscopic management of afferent loop syndrome after a pylorus preserving pancreatoduodenecotomy presenting with obstructive jaundice and ascending cholangitis. Clin Endosc. 2011; 44:59–64.
Article7. Kida A, Matsuda K, Noda Y. Endoscopic metallic stenting by double-balloon enteroscopy and its overtube for malignant gastrointestinal obstruction as palliative treatment. Dig Endosc. 2013; 25:552–553.
Article8. Kwong WT, Fehmi SM, Lowy AM, Savides TJ. Enteral stenting for gastric outlet obstruction and afferent limb syndrome following pancreaticoduodenectomy. Ann Gastroenterol. 2014; 27:413–417.9. Sasaki T, Isayama H, Kogure H, et al. Double-balloon enteroscope-assisted enteral stent placement for malignant afferent-loop obstruction after Roux-en-Y reconstruction. Endoscopy. 2014; 46 Suppl 1 UCTN:E541–E542.
Article10. Huang J, Hao S, Yang F, et al. Endoscopic metal enteral stent placement for malignant afferent loop syndrome after pancreaticoduodenectomy. Wideochir Inne Tech Maloinwazyjne. 2015; 10:257–265.
Article11. Fujii M, Ishiyama S, Saito H, et al. Metallic stent insertion with double-balloon endoscopy for malignant afferent loop obstruction. World J Gastrointest Endosc. 2015; 7:665–669.
Article12. Nakahara K, Okuse C, Matsumoto N, et al. Enteral metallic stenting by balloon enteroscopy for obstruction of surgically reconstructed intestine. World J Gastroenterol. 2015; 21:7589–7593.
Article13. Shimatani M, Takaoka M, Tokuhara M, et al. Through-the-scope self-expanding metal stent placement using newly developed short double-balloon endoscope for the effective management of malignant afferent-loop obstruction. Endoscopy. 2016; 48 Suppl 1 UCTN:E6–E7.
Article14. Minaga K, Kitano M, Takenaka M. Through-the-scope enteral metal stent placement using a short-type single-balloon enteroscope for malignant surgically reconstructed jejunal stenosis (with video). Dig Endosc. 2016; 28:758.
Article15. Kanno Y, Ohira T, Harada Y, et al. Metal stent placement in the afferent loop obstructed by peritoneal metastases-experience of five cases. Clin Endosc. 2018; 51:299–303.
Article16. Yane K, Katanuma A, Hayashi T, et al. Enteral self-expandable metal stent placement for malignant afferent limb syndrome using single-balloon enteroscope: report of five cases. Endosc Int Open. 2018; 6:E1330–E1335.
Article17. Ikeuchi N, Itoi T, Tsuchiya T, Nagakawa Y, Tsuchida A. One-step EUS-guided gastrojejunostomy with use of lumen-apposing metal stent for afferent loop syndrome treatment. Gastrointest Endosc. 2015; 82:166.
Article18. Toliopoulos P, Manière T, Désilets E. Treatment of neoplastic afferent limb syndrome by endoscopic gastrojejunostomy with a lumen-apposing metal stent. VideoGIE. 2018; 3:61–62.
Article19. Yamamoto K, Tsuchiya T, Tanaka R, et al. Afferent loop syndrome treated by endoscopic ultrasound-guided gastrojejunostomy, using a lumen-apposing metal stent with an electrocautery-enhanced delivery system. Endoscopy. 2017; 49:E270–E272.
Article20. Shiomi H, Kobayashi T, Sakai A, et al. Endoscopic ultrasound-guided gastrojejunostomy using fully covered metal stent combined with largeloop double-pigtail stent for malignant afferent loop syndrome. Endoscopy. 2019; 51:E303–E304.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Metal Stent Placement in the Afferent Loop Obstructed by Peritoneal Metastases—Experience of Five Cases
- A Case of Afferent Loop Syndrome Treated by Endoscopic Metal Stent Insertion Using Two Endoscopes
- Percutaneous Enteral Stent Placement Using a Transhepatic Access for Palliation of Malignant Bowel Obstruction after Surgery
- Extra-anatomic percutaneous stenting of a malignant afferent loop obstruction following pancreaticoduodenectomy
- Endoscopic Management of Afferent Loop Syndrome after a Pylorus Preserving Pancreatoduodenecotomy Presenting with Obstructive Jaundice and Ascending Cholangitis
