Ann Rehabil Med.
2020 Jun;44(3):210-217. 10.5535/arm.19117.
Efficacy of Modified Cervical and Shoulder Retraction Exercise in Patients With Loss of Cervical Lordosis and Neck Pain
- Affiliations
-
- 1Department of Rehabilitation Medicine, Seoul National University Hospital, Seoul, Korea
- 2Department of Rehabilitation Medicine, Seoul National University Bundang Hospital, Bundang, Korea
- 3Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2504441
- DOI: http://doi.org/10.5535/arm.19117
Abstract
Objective
To explore if the modified cervical and shoulder retraction exercise program restores cervical lordosis and reduces neck pain in patients with loss of cervical lordosis.
Methods
This study was a retrospective analysis of prospectively collected data. Eighty-three patients with loss of cervical lordosis were eligible. The eligible patients were trained to perform the modified cervical and shoulder retraction exercise program by a physiatrist, and were scheduled for a follow-up 6 to 8 weeks later to check the post-exercise pain intensity and lateral radiograph of the cervical spine in a comfortable position. The parameters of cervical alignment (4-line Cobb’s angle, posterior tangent method, and sagittal vertical axis) were measured from the lateral radiograph.
Results
Forty-seven patients were included. The mean age was 48.29±14.47 years. Cervical alignment and neck pain significantly improved after undergoing the modified cervical and shoulder retraction exercise program (p≤0.001). The upper cervical lordotic angle also significantly improved (p=0.001). In a subgroup analysis, which involved dividing the patients into two age groups (<50 years and ≥50 years), the change of the sagittal vertical axis was significantly greater in the <50 years group (p=0.021).
Conclusion
The modified cervical and shoulder retraction exercise program tends to improve cervical lordosis and neck pain in patients with loss of cervical lordosis.
Figure
-

Fig. 1. The modified cervical and shoulder retraction exercise. Two steps: raise head up and push the chin backward simultaneously within the pain free range (A), and keep upright and try to pull back the shoulder and head within the pain free range (B).
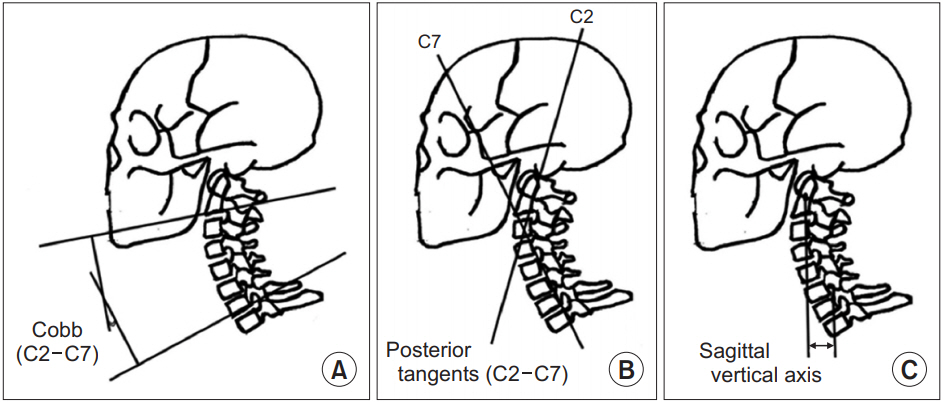
Fig. 2. Radiologic parameters: the 4-line Cobb’s angle (A), posterior tangent method (B), and sagittal vertical axis (C).

Fig. 3. Improvement of cervical lordosis in the patients after the exercise: the 4-line Cobb’s angle (A), posterior tangent method (B), and sagittal vertical axis (C).
Reference
-
1. Alpayci M, Ilter S. Isometric exercise for the cervical extensors can help restore physiological lordosis and reduce neck pain: a randomized controlled trial. Am J Phys Med Rehabil. 2017; 96:621–6.2. Been E, Shefi S, Soudack M. Cervical lordosis: the effect of age and gender. Spine J. 2017; 17:880–8.
Article3. McAviney J, Schulz D, Bock R, Harrison DE, Holland B. Determining the relationship between cervical lordosis and neck complaints. J Manipulative Physiol Ther. 2005; 28:187–93.
Article4. Ferrara LA. The biomechanics of cervical spondylosis. Adv Orthop. 2012; 2012:493605.
Article5. Hansraj KK. Assessment of stresses in the cervical spine caused by posture and position of the head. Surg Technol Int. 2014; 25:277–9.6. Iwasaki M, Yamamoto T, Miyauchi A, Amano K, Yonenobu K. Cervical kyphosis: predictive factors for progression of kyphosis and myelopathy. Spine (Phila Pa 1976). 2002; 27:1419–25.7. Okada E, Matsumoto M, Ichihara D, Chiba K, Toyama Y, Fujiwara H, et al. Does the sagittal alignment of the cervical spine have an impact on disk degeneration? Minimum 10-year follow-up of asymptomatic volunteers. Eur Spine J. 2009; 18:1644–51.
Article8. Alpayci M, Senkoy E, Delen V, Sah V, Yazmalar L, Erden M, et al. Decreased neck muscle strength in patients with the loss of cervical lordosis. Clin Biomech (Bristol, Avon). 2016; 33:98–102.
Article9. Harman K, Hubley-Kozey CL, Butler H. Effectiveness of an exercise program to improve forward head posture in normal adults: a randomized, controlled 10-week trial. J Man Manip Ther. 2005; 13:163–76.
Article10. Pearson ND, Walmsley RP. Trial into the effects of repeated neck retractions in normal subjects. Spine (Phila Pa 1976). 1995; 20:1245–51.
Article11. Ordway NR, Seymour RJ, Donelson RG, Hojnowski LS, Edwards WT. Cervical flexion, extension, protrusion, and retraction: a radiographic segmental analysis. Spine (Phila Pa 1976). 1999; 24:240–7.12. Ohara A, Miyamoto K, Naganawa T, Matsumoto K, Shimizu K. Reliabilities of and correlations among five standard methods of assessing the sagittal alignment of the cervical spine. Spine (Phila Pa 1976). 2006; 31:2585–92.
Article13. Ames CP, Blondel B, Scheer JK, Schwab FJ, Le Huec JC, Massicotte EM, et al. Cervical radiographical alignment: comprehensive assessment techniques and potential importance in cervical myelopathy. Spine (Phila Pa 1976). 2013; 38(22 Suppl 1):S149–60.14. Park J, Kim J, Kim J, Kim K, Kim N, Choi I, et al. The effects of heavy smartphone use on the cervical angle, pain threshold of neck muscles and depression. Adv Sci Technol Lett. 2015; 91:12–7.
Article15. Wilder DG, Pope MH, Frymoyer JW. The biomechanics of lumbar disc herniation and the effect of overload and instability. J Spinal Disord. 1988; 1:16–32.
Article16. Ruivo RM, Pezarat-Correia P, Carita AI. Effects of a resistance and stretching training program on forward head and protracted shoulder posture in adolescents. J Manipulative Physiol Ther. 2017; 40:1–10.
Article17. Buckwalter JA. Aging and degeneration of the human intervertebral disc. Spine (Phila Pa 1976). 1995; 20:1307–14.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Impact of Fat Infiltration in Cervical Extensor Muscles on Cervical Lordosis and Neck Pain: A Cross-Sectional Study
- Radiologic Assessment of Forward Head Posture and Its Relation to Myofascial Pain Syndrome
- The Effect of Cervical Kyongrak Massage on Shoulder Pain, Shoulder Exercise Range and Mood in the Elderly
- Correlation of Cervical Disc Degeneration with Sagittal Alignments of Cervical Spine
- Radiologic Finding of Patients with Neck Pain
