Coexistent Papillary Thyroid Carcinoma and Its Anaplastic Transformation in Cervical Lymph Node Metastasis
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Gyeongsang National University College of Medicine, Gyeongsang National University Changwon Hospital, Changwon, Korea
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- 3Department of Pathology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- KMID: 2502262
- DOI: http://doi.org/10.11106/ijt.2020.13.1.55
Abstract
- The transformation of papillary thyroid carcinoma (PTC) to anaplastic thyroid carcinoma (ATC) is well documented in the literature but is an exceptionally rare occurrence in metastatic foci outside the primary thyroid lesion. Even rarer is the simultaneous occurrence of PTC and ATC in the cervical lymph nodes. We report the case of an 85–year–old man who presented with a rapidly growing neck mass diagnosed as PTC. Following surgery, multiple ATC foci in the metastatic cervical lymph node were found coexisting with PTC, whereas in the thyroid, only PTC was found. This case is of high clinical significance because transformation of PTC to ATC outside the thyroid gland per se is very rare and because it suggests rapidly growing tumors in an elderly patient. The use of core needle biopsies in cases with suspected rapid tumor growth can aid in proper diagnosis, surgical decision making, and patient counselling.
Keyword
Figure
-
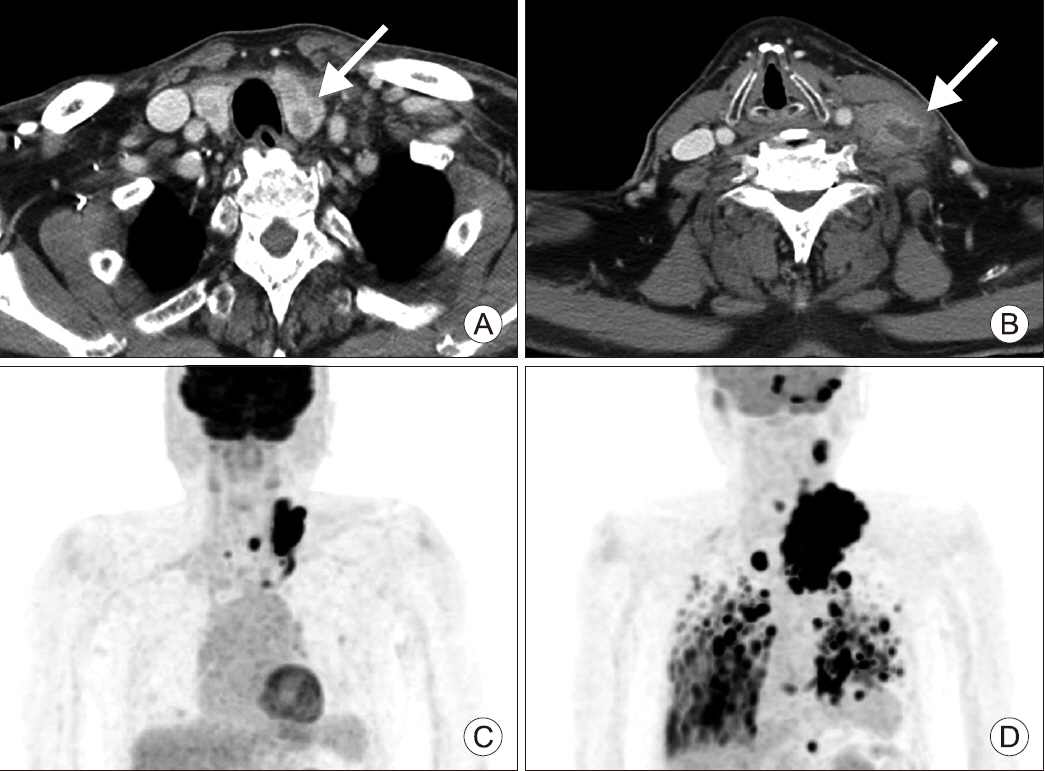
Fig. 1 (A) Computed tomography of the neck shows a large-sized mass (2×2×3.2 cm) in the left thyroid gland (arrow). (B) Computed tomography of the neck shows the left level IV lymph node with enlarged size (4.7×3.1 cm) (arrow). (C) Positron emission tomography-computed tomography (PET-CT) scan. Hypermetabolic nodule in the left thyroid lobe. Hypermetabolic enlarged lymph nodes in left neck level III, IV, right level VI and superior mediastinum. Small nodules with hypermetabolism in both lungs. (D) PET-CT scan. Local recurrence with disseminated metastasis to lymph nodes, lungs, bones, cerebellum, left adrenal gland, and cardiac RV wall.
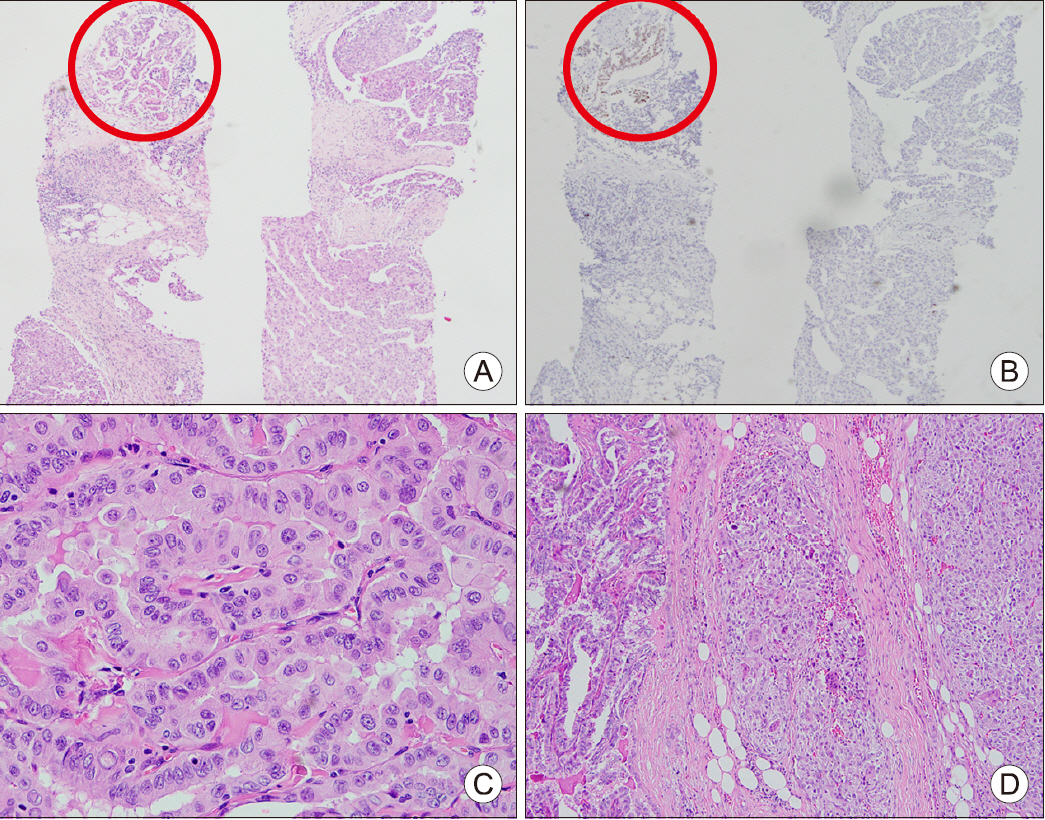
Fig. 2 Pathology finding of cervical lymph node core needle biopsy specimen. (A) The metastatic tumor composed of a minor papillary thyroid carcinoma component (left upper, red circle) and the majority of the biopsied specimen with poorly differentiated histology different from PTC; Hematoxylin & Eosin staining (H&E) ×40. (B) Immunohistochemical staining of PAX8. PAX8 was expressed only in the papillary thyroid carcinoma component (left upper, red circle) and negative in the poorly differentiated tumor component; H&E ×40. Pathology finding of surgically resected specimen. (C) Thyroid; H&E ×400. (D) Lymph node; H&E ×400.
Reference
-
1. Nishiyama RH, Dunn EL, Thompson NW. 1972; Anaplastic spindle-cell and giant-cell tumors of the thyroid gland. Cancer. 30(1):113–27. DOI: 10.1002/1097-0142(197207)30:1<113::AID-CNCR2820300118>3.0.CO;2-E. PMID: 5040735.
Article2. Papp S, Asa SL. 2015; When thyroid carcinoma goes bad: a morphological and molecular analysis. Head Neck Pathol. 9(1):16–23. DOI: 10.1007/s12105-015-0619-z. PMID: 25804379. PMCID: PMC4382495.
Article3. Kawahara E, Ooi A, Oda Y, Katsuda S, Terahata S, Michigishi T. 1986; Papillary carcinoma of the thyroid gland with anaplastic transformation in the metastatic foci. An immunohistochemical study. Acta Pathol Jpn. 36(6):921–7. DOI: 10.1111/j.1440-1827.1986.tb03125.x. PMID: 3766138.
Article4. Wiseman SM, Loree TR, Rigual NR, Hicks WL Jr, Douglas WG, Anderson GR, et al. 2003; Anaplastic transformation of thyroid cancer: review of clinical, pathologic, and molecular evidence provides new insights into disease biology and future therapy. Head Neck. 25(8):662–70. DOI: 10.1002/hed.10277. PMID: 12884350.
Article5. Togashi S, Oka K, Kanayama R, Koyamatsu S, Tobita T, Yatabe Y, et al. 2004; Thyroid anaplastic carcinoma transformed from papillary carcinoma in extrathyroid area. Auris Nasus Larynx. 31(3):287–92. DOI: 10.1016/j.anl.2004.03.006. PMID: 15364366.
Article6. Sato K, Waseda R, Tatsuzawa Y, Soma R, Ueda Y, Katsuda S. 2006; Papillary thyroid carcinoma with anaplastic transformation showing a rhabdoid phenotype solely in the cervical lymph node metastasis. Pathol Res Pract. 202(1):55–9. DOI: 10.1016/j.prp.2005.10.004. PMID: 16310972.
Article7. Sotome K, Onishi T, Hirano A, Nakamaru M, Furukawa A, Miyazaki H, et al. 2007; A rare case of anaplastic transformation within the metastatic site of the retroperitoneal region in a patient 17 years after total thyroidectomy for papillary carcinoma of the thyroid beginning with multiple bone metastases. Thyroid. 17(12):1309–11. DOI: 10.1089/thy.2006.0322. PMID: 18177259.
Article8. Ito Y, Higashiyama T, Hirokawa M, Fukushima M, Inoue H, Yabuta T, et al. 2008; Prognosis of patients with papillary carcinoma showing anaplastic transformation in regional lymph nodes that were curatively resected. Endocr J. 55(6):985–9. DOI: 10.1507/endocrj.K08E-148. PMID: 18612180.
Article9. Sung TY, Hong SW, Kang SW, Lee SC, Jeong JJ, Lee YS, et al. 2008; Anaplastic transformation of metastatic papillary thyroid carcinomas in the cervical lymph nodes: report of 3 cases. Korean J Endocr Surg. 8(3):210–4. DOI: 10.16956/kjes.2008.8.3.210.
Article10. Takeshita Y, Takamura T, Minato H, Misu H, Ando H, Yamashita T, et al. 2008; Transformation of p53-positive papillary thyroid carcinoma to anaplastic carcinoma of the liver following postoperative radioactive iodine-131 therapy. Intern Med. 47(19):1709–12. DOI: 10.2169/internalmedicine.47.1190. PMID: 18827421.
Article11. Angeles-Angeles A, Chable-Montero F, Martinez-Benitez B, Albores-Saavedra J. 2009; Unusual metastases of papillary thyroid carcinoma: report of 2 cases. Ann Diagn Pathol. 13(3):189–96. DOI: 10.1016/j.anndiagpath.2008.02.010. PMID: 19433299.
Article12. Al-Qsous W, Miller ID. 2010; Anaplastic transformation in lung metastases of differentiated papillary thyroid carcinoma: an autopsy case report and review of the literature. Ann Diagn Pathol. 14(1):41–3. DOI: 10.1016/j.anndiagpath.2009.04.003. PMID: 20123456.
Article13. Deutschmann M, Khalil M, Bhayana S, Chandarana S. 2013; Occult multifocal papillary thyroid microcarcinoma presenting as a supraclavicular mass containing anaplastic thyroid carcinoma. JAMA Otolaryngol Head Neck Surg. 139(4):415–8. DOI: 10.1001/jamaoto.2013.227. PMID: 23599079.
Article14. Na DG, Baek JH, Sung JY, Kim JH, Kim JK, Choi YJ, et al. 2016; Thyroid imaging reporting and data system risk stratification of thyroid nodules: categorization based on solidity and echogenicity. Thyroid. 26(4):562–72. DOI: 10.1089/thy.2015.0460. PMID: 26756476.
Article15. Albores-Saavedra J, Henson DE, Glazer E, Schwartz AM. 2007; Changing patterns in the incidence and survival of thyroid cancer with follicular phenotype--papillary, follicular, and anaplastic: a morphological and epidemiological study. Endocr Pathol. 18(1):1–7. DOI: 10.1007/s12022-007-0002-z. PMID: 17652794.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anaplastic Transformation of Metastatic Papillary Thyroid Carcinomas in the Cervical Lymph Nodes: Report of 3 Cases
- A Case of Cystic Lymph Node Metastasis from Thyroid Papillary Microcarcinoma
- Retropharyngeal Lymph Node Metastasis of Thyroid Papillary Carcinoma
- Kikuchi-Fujimoto Disease Coexistent with Papillary Thyroid Carcinoma in a Single Lymph Node
- The Pattern of Cervical Lymph Node Metastases in Papillary Thyroid Cancer
