Successful Management of Visceral Kaposiform Hemangioendothelioma with Kasabach‐Merritt Phenomenon Using Corticosteroids and Vincristine
- Affiliations
-
- 1Department of Pediatrics, Chungnam National University Hospital, Chungnam National University College of Medicine, Daejeon, Korea
- KMID: 2502092
- DOI: http://doi.org/10.5385/nm.2020.27.1.37
Abstract
- Kaposiform hemangioendothelioma (KHE) is a rare, locally aggressive vascular neoplasm that often develops a coagulopathy known as KasabachMerritt phenomenon (KMP). Visceral involvement denotes a poor prognosis. We report a case of visceral KHE with KMP successfully treated with corticosteroids and vincristine. The infant had been born vaginally at 34 weeks 6 days’ gestation, weighing 2,360 g. He was admi tted for the management of respiratory failure. Blood tests showed anemia and thrombocytopenia 1 hour after delivery. Additional blood tests revealed a prothrombin time of 12.1 seconds, activated partial thromboplastin time of 60.6 seconds, fibrinogen levels of 72.4 mg/dL, and Ddimer levels >3,200 ng/mL. Despite supportive measures and daily transfusions, the clinical condition and coagulopathy gradually worsened. Renal ultrasonography performed to find the origin of the coagulopathy revealed an echogenic mass measuring >3 cm in the abdominal cavity. A magnetic resonance imaging scan showed an illmarginated, infiltrative mass like lesion in the right anteromedial and posteromedial perirenal space that was hypointense with mild enhance ment on T1 and T2weighted images. Large vascular tumors adherent to other visceral organs were noted during exploratory laparotomy but could not be resected. Treatment with methylprednisolone was ineffective. Vincristine was administered weekly from the 17th hospital day, and the coagulation profile showed gradual impro vement after its initiation. Intravenous methylprednisolone was switched to oral prednisolone on the 57th hospital day. He was discharged on the 73rd hospital day and continued vincristine treatment every 2 weeks and oral prednisolone administration as an outpatient treatment for 8 weeks. He remained symptomfree at the 39month followup.
Keyword
Figure
-
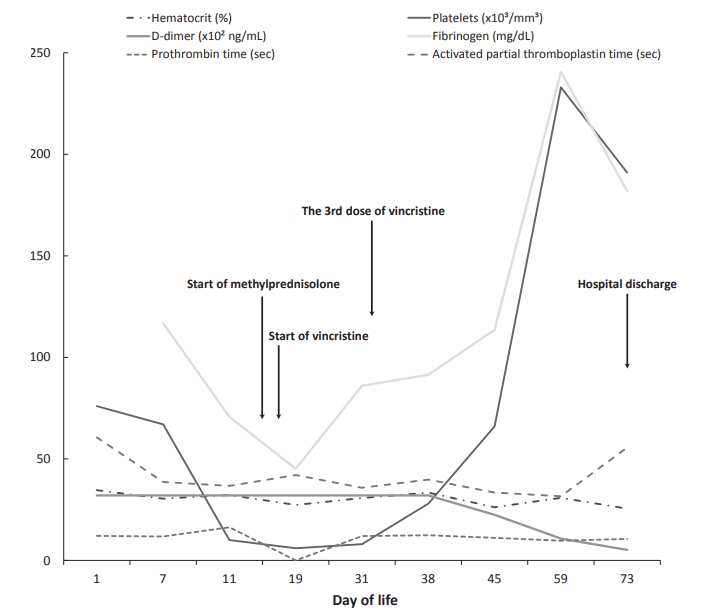
Figure 1. Hematologic laboratory values during the hospital course. D-dimer levels >3,200 ng/mL are indicated as 32×102 ng/mL in the graph.
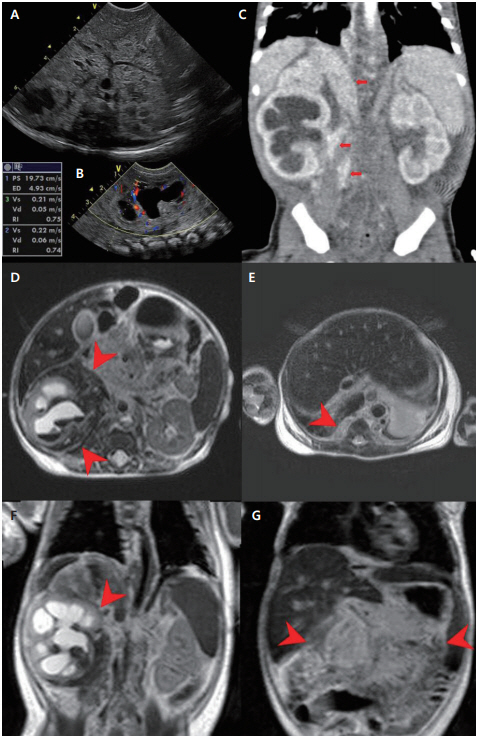
Figure 2. Imaging studies of the patient. (A) Renal ultrasonography performed on the 6th day of life showing diffusely echogenic soft tissue surrounding the inferior vena cava, aorta, and its branches. (B) Renal ultrasonography performed on the 6th day of life showing diffusely increased parenchymal echogenicity of the right kidney with hydronephrosis. (C) Abdominopelvic computed tomography performed on the 7th day of life showing diffuse, ill-marginated enhancing lesion surrounding the right renal hilum and right inferomedial aspects of the perirenal space (indicated by arrows). (D) Abdominal magnetic resonance imaging (MRI) scan showing diffuse, ill-marginated infiltrative mass like lesion on the right anteromedial and posteromedial aspects of the perirenal space. (E) Abdominal MRI scan showing asymmetric thickening of right crura. (F) Abdominal MRI scan showing right hydronephrosis and hemorrhage/hematoma inside the right kidney. (G) Abdominal MRI scan showing the mesentery with diffuse high signal intensity on a T1-weighted image (indicated by arrowheads).
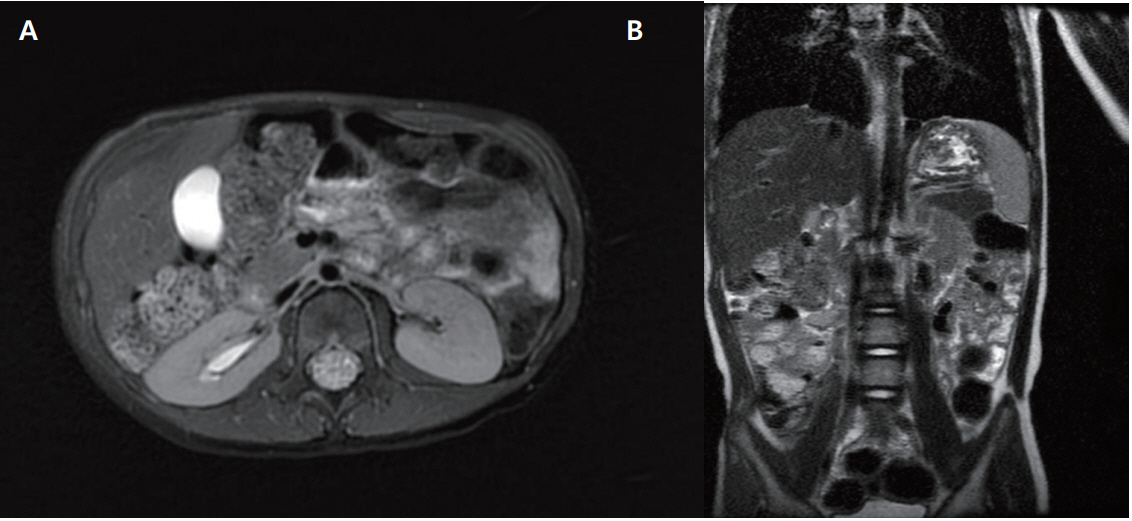
Figure 3. Follow-up magnetic resonance imaging performed at 39 months of age. (A, B) Unremarkable finding in the right perirenal space and the upper abdomen except for mild right hydronephrosis.
Reference
-
1. Fletcher CDM; World Health Organization. WHO classification of tumours of soft tissue and bone. 4th ed. Lyon: International Agency for Research on Cancer;2013. p. 110–1.2. Fernandez Y, Bernabeu-Wittel M, Garcia-Morillo JS. Kaposiform hemangioendothelioma. Eur J Intern Med. 2009; 20:106–13.3. Nakaya T, Morita K, Kurata A, Ushiku T, Igarashi T, Kuroda M, et al. Multifocal kaposiform hemangioendothelioma in multiple visceral organs: an autopsy of 9-day-old female baby. Hum Pathol. 2014; 45:1773–7.4. Kasabach HH, Merritt KK. Capillary hemangioma with extensive purpura: report of a case. Am J Dis Child. 1940; 59:1063–70.5. Gilon E, Ramot B, Sheba C. Multiple hemangiomata associated with thrombocytopenia: remarks on the pathogenesis of the thrombocytopenia in this syndrome. Blood. 1959; 14:74–9.6. Brizel HE, Raccuglia G. Giant hemangioma with thrombo cytopenia. Radioisotopic demonstration of platelet sequestra tion. Blood. 1965; 26:751–64.7. Seo SK, Suh JC, Na GY, Kim IS, Sohn KR. Kasabach-Merritt syndrome: identification of platelet trapping in a tufted angioma by immunohistochemistry technique using monoclonal anti body to CD61. Pediatr Dermatol. 1999; 16:392–4.8. Hall GW. Kasabach-Merritt syndrome: pathogenesis and mana gement. Br J Haematol. 2001; 112:851–62.9. Pascal S, Bettex Q, Andre N, Petit P, Casanova D, Degardin N. Successful surgical management of congenital KasabachMerritt syndrome. Pediatr Int. 2017; 59:89–92.10. Drolet BA, Trenor CC 3rd, Brandao LR, Chiu YE, Chun RH, Dasgupta R, et al. Consensus-derived practice standards plan for complicated Kaposiform hemangioendothelioma. J Pediatr. 2013; 163:285–91.11. Kim MG, Choi YS, Park SJ, Chong SM. Kaposiform hemangioendothelioma of the breast in an adult female. Clin Breast Can cer. 2011; 11:135–7.12. Drucker AM, Pope E, Mahant S, Weinstein M. Vincristine and corticosteroids as first-line treatment of Kasabach-Merritt syndrome in kaposiform hemangioendothelioma. J Cutan Med Surg. 2009; 13:155–9.13. Hauer J, Graubner U, Konstantopoulos N, Schmidt S, Pfluger T, Schmid I. Effective treatment of kaposiform hemangioendotheliomas associated with Kasabach-Merritt phenomenon using four-drug regimen. Pediatr Blood Cancer. 2007; 49:852–4.14. Barabash-Neila R, Garcia-Rodriguez E, Bernabeu-Wittel J, Bueno-Rodriguez I, Ramirez-Villar G, Lopez-Gutierrez JC. Kaposiform hemangioendothelioma with Kasabach-Merritt phenomenon: successful treatment with vincristine and ticlopidine. Indian J Pediatr. 2012; 79:1386–7.15. Greinwald JH Jr, Burke DK, Bonthius DJ, Bauman NM, Smith RJ. An update on the treatment of hemangiomas in children with interferon alfa-2a. Arch Otolaryngol Head Neck Surg. 1999; 125:21–7.16. Lopez V, Marti N, Pereda C, Martin JM, Ramon D, Mayordomo E, et al. Successful management of Kaposiform hemangio endothelioma with Kasabach-Merritt phenomenon using vincristine and ticlopidine. Pediatr Dermatol. 2009; 26:365–6.17. Mizutani K, Umaoka A, Tsuda K, Kakeda M, Habe K, Yamanaka K, et al. Successful combination therapy of propranolol and prednisolone for a case with congenital Kasabach-Merritt syndrome. J Dermatol. 2017; 44:1389–91.18. Cashell J, Smink GM, Helm K, Xavier F. Kaposiform hemangioendothelioma with Kasabach-Merritt phenomenon in an infant: Successful treatment with prednisolone, vincristine, and addition of sirolimus. Pediatr Blood Cancer. 2018; 65:e27305.19. Garcia-Monaco R, Giachetti A, Peralta O, Napoli N, Lobos P, Gioseffi L, et al. Kaposiform hemangioendothelioma with Kasa- bach-Merritt phenomenon: successful treatment with embolization and vincristine in two newborns. J Vasc Interv Radiol. 2012; 23:417–22.20. Hesselmann S, Micke O, Marquardt T, Baas S, Bramswig JH, Harms E, et al. Case report: Kasabach-Merritt syndrome. A review of the therapeutic options and a case report of successful treatment with radiotherapy and interferon alpha. Br J Radiol. 2002; 75:180–4.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Kaposiform Hemangioendothelioma Complicated by Kasabach - Merritt Phenomenon with Bone Involvement in an Adult
- Effective Management of Kaposiform Hemangioendotheliomas Associatedwith Kasabach-Merritt Syndrome Using Chemotherapy
- Successful Management with Vincristine after Failure of Prednisolone Therapy for Diffuse Neonatal Hemangiomatosis
- A Case of Kasabach-Merritt Syndrome
- Anesthetic management of a patient with Kasabach-Merritt syndrome: A case report
