Surgical Management of Complex Spinal Cord Lipomas : A New Perspective
- Pang D
 1,2
1,2
- Affiliations
-
- 1Department of Paediatric Neurosurgery, Great Ormond Street Hospital for Children, NHS Trust, London, UK
- 2Department of Paediatric Neurosurgery, University of California, Davis, CA, USA
- KMID: 2501716
- DOI: http://doi.org/10.3340/jkns.2020.0024
Abstract
- This review summarises the classification, anatomy and embryogenesis of complex spinal cord lipomas, and describes in some detail the new technique of total lipoma resection and radical reconstruction of the affected neural placode. Its specific mission is to tackle two main issues surrounding the management of complex dysraphic lipomas : whether total resection confers better long term benefits than partial resection, and whether total resection does better than conservative treatment, i.e., no surgery, for asymptomatic lipomas. Accordingly, the 24 years progression-free survival data of the author and colleagues’ series of over 350 cases of total resection are compared with historical data from multiple series (including our own) of partial resection, and total resection data specifically for asymptomatic lesions are compared with the two known series of non-surgical treatment of equivalent patients. These comparisons amply support the author’s recommendation of total resection for most complex lipomas, with or without symptoms. The notable exception is the asymptomatic chaotic lipoma, whose peculiar anatomical relationship with the neural tissue defies even our aggressive surgical approach, and consequently projects worse results (admittedly of small number of cases) than for the other two lipoma subtypes of dorsal and transitional lesions. Prophylactic resection of asymptomatic chaotic lipomas is therefore not currently endorsed.
Figure
-
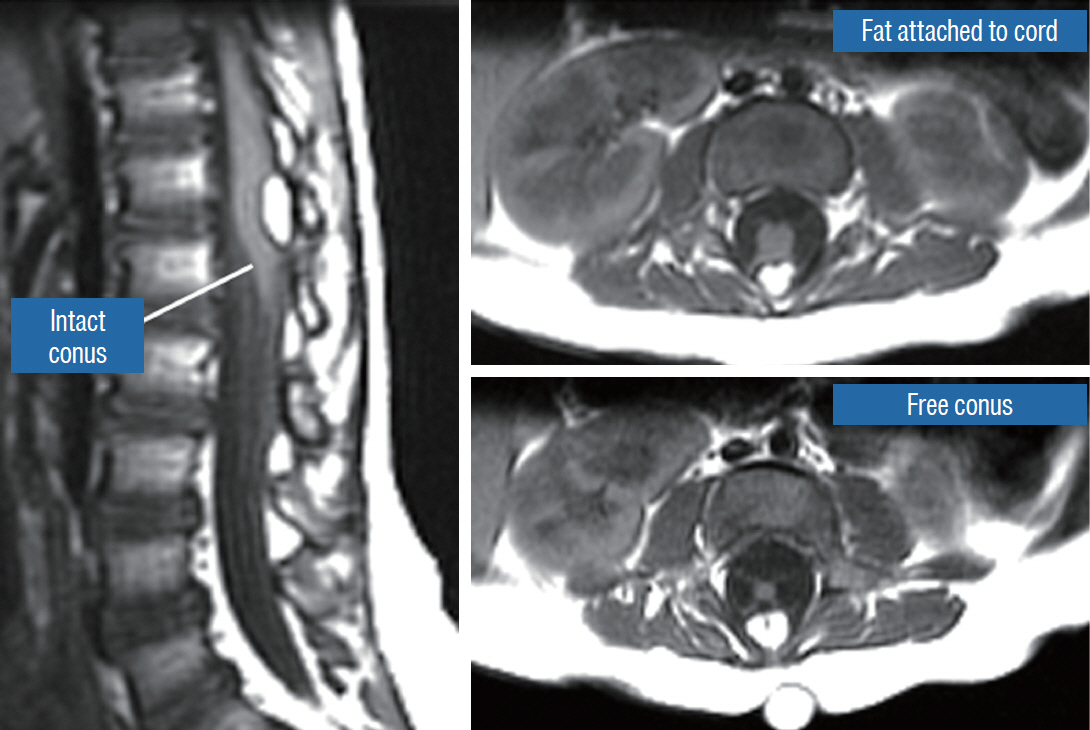
Fig. 1. Dorsal lipoma on magnetic resonance imaging. Sagittal image shows intact conus caudal to lipoma stalk. Axial images : upper shows site of lipoma attachment to cord; lower shows free conus just caudal to the level of lipoma attachment. Reprinted from Pang et al. [61] with permission from Springer Nature.
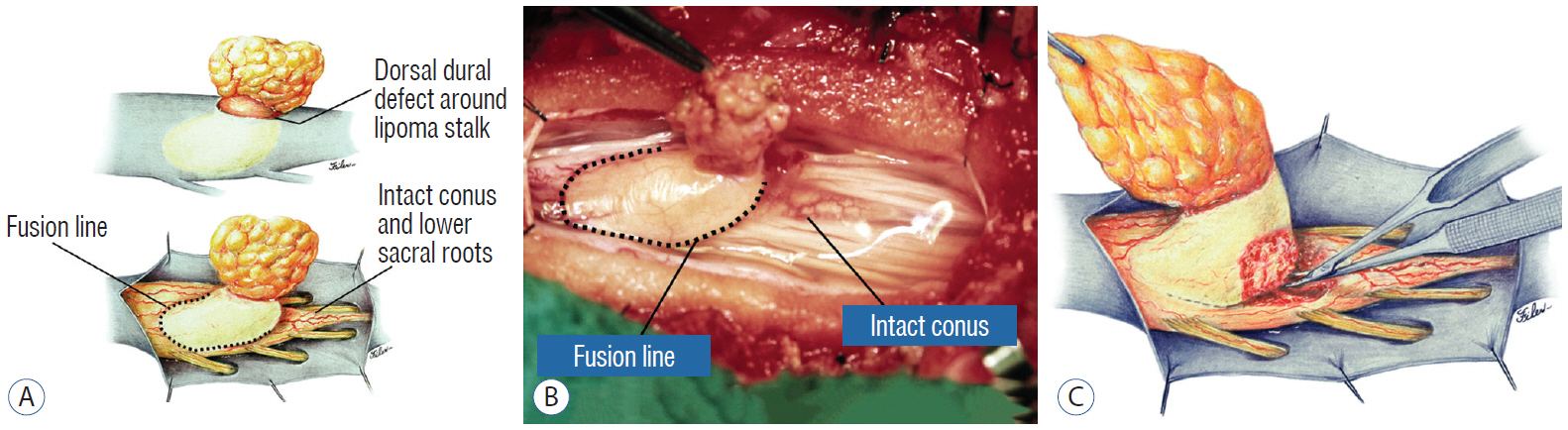
Fig. 2. Dorsal lipoma. A : Intraoperative drawings : upper shows neat dorsal dural defect through which lipoma stalk goes. Lower shows circumferential fusion line and intact conus. B : Intraoperative picture shows neat oval fusion line around lipoma-cord interface on a horizontal plane. Note intact conus and caudal sacral roots. C : Resection of dorsal lipoma can be executed with a completely circumscribed perspective from all sides of the fusion line, impossible with transitional lipoma. Reprinted from Pang et al. [61] with permission from Springer Nature.
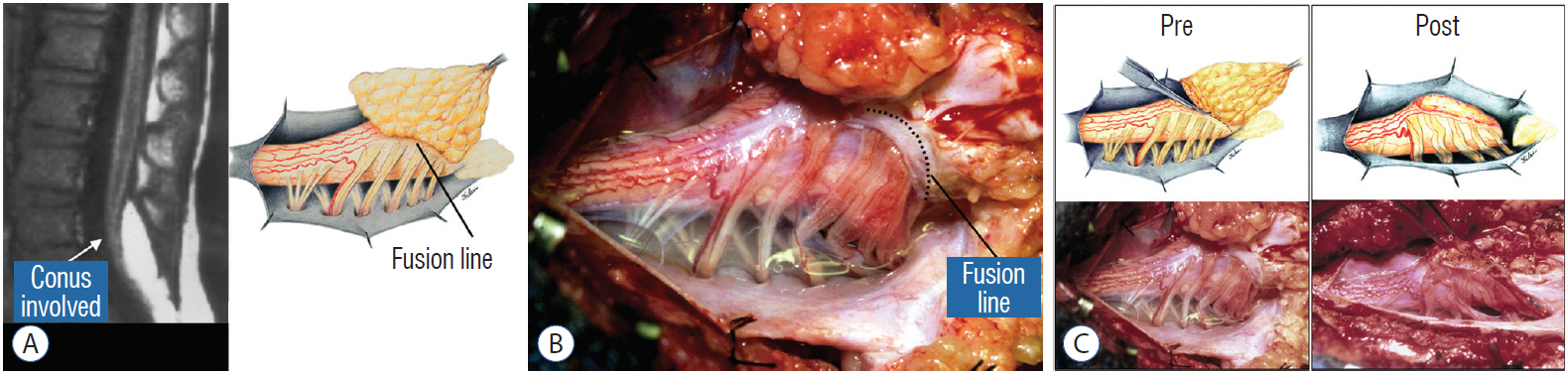
Fig. 3. Transitional lipoma. A : Left : sagittal MRI shows lipoma begins dorsally but involves entire conus. Ventral side of neural placode is free of fat. Right : the plane of the fusion line begins dorsally then cuts obliquely towards the tip of the conus. The array of DREZ and dorsal roots is also forced to slant dorso-ventrally. B : Intraoperative picture showing massive lipoma but very distinct dorso-ventral fusion line separating fat from the DREZ and dorsal roots, which always lie lateral and ventral to the fusion line. The ventral side of the placode is always free of fat in a regular transitional lipoma. C : Top : idealised drawings of pre- and post-resection of a relatively “standard” transitional lipoma, along an asymmetrical and oblique plane bound by the fusion line on each side, over an occasionally undulating lipoma-cord interface. Bottom shows pre- and post-resection intraoperative pictures. Reprinted from Pang et al. [61] with permission from Springer Nature. MRI : magnetic resonance imaging, DREZ : dorsal root entry zone.
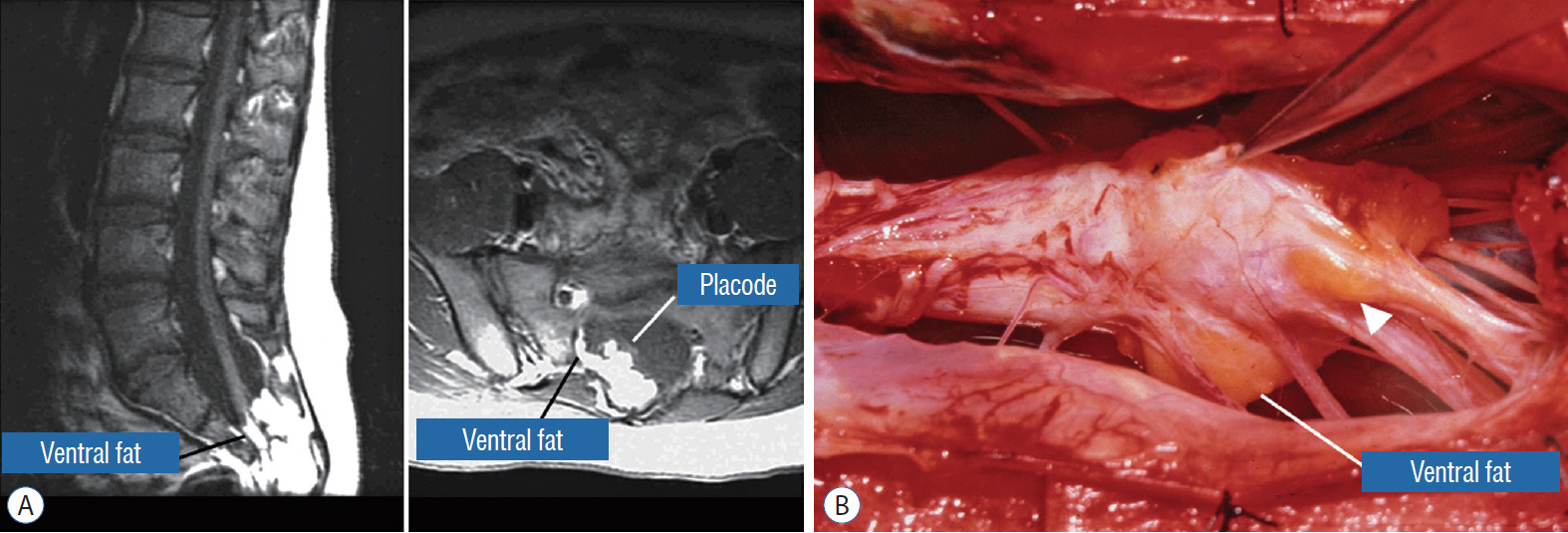
Fig. 4. Chaotic lipoma. A : Left : sagittal magnetic resonance imaging shows ventral as well as dorsal fat in relation to the neural placode. Note sacral agenesis with only two visible sacral segments. Right : axial image shows ventral fat and extremely irregular lipoma-fat interface. B : Intraoperative picture showing fat ventral to placode and on one of the sacral roots (arrowhead). Note absence of discrete fusion line. Reprinted from Pang et al. [61] with permission from Springer Nature.
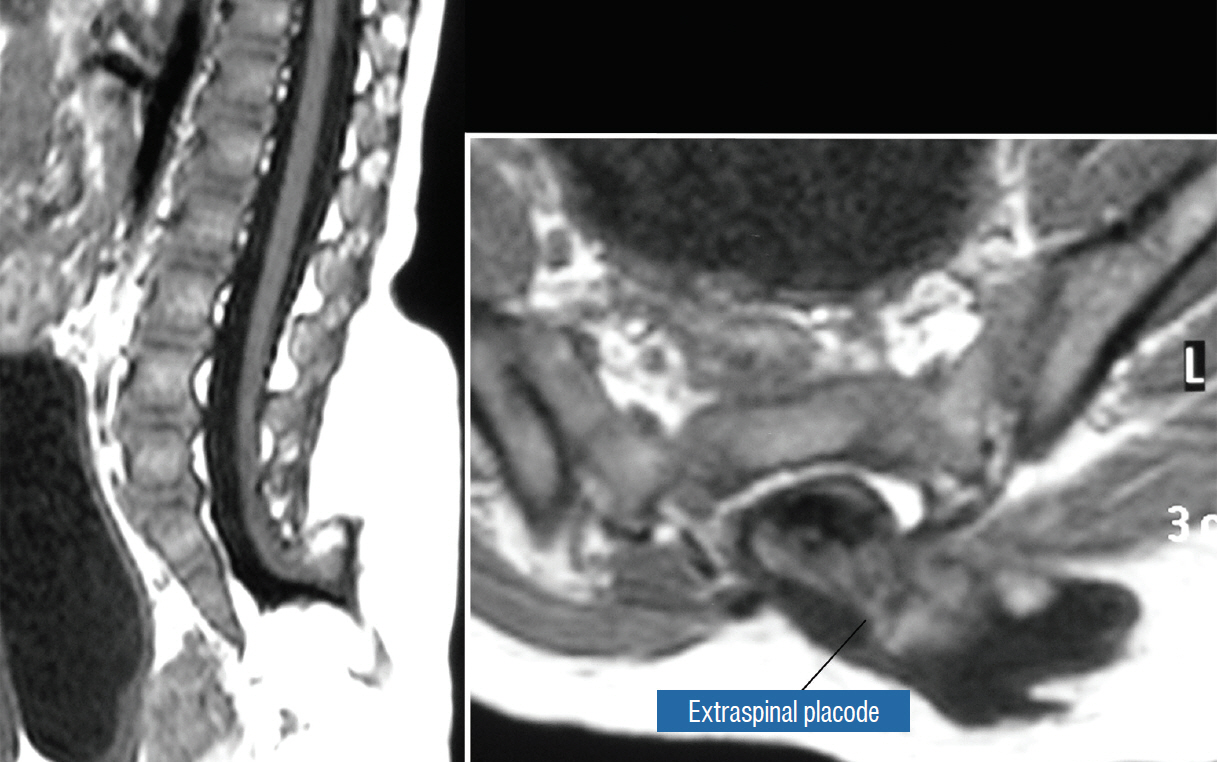
Fig. 5. Transitional lipoma with extraspinal extension (“lipomyelomeningocoele”), with the lipoma, cerebrospinal fluid sac, and part of the neural placode extending out of the spinal canal through a dorsal defect. Reprinted from Pang et al. [61] with permission from Springer Nature.

Fig. 6. Embryogenesis of dorsal lipoma, a pure primary neurulation defect. A and B : Premature disjunction before complete closure of neural plates allows migration of mesenchymal cells into neural groove to establish contact with the ependymal surface. C and D : Formation of fusion line between lipoma, cord, and pia-arachnoid. DREZ and dorsal root are always lateral to the fusion line and thus not entangled in fat. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society. CE : cutaneous ectoderm, NC : neural crest, Me : mesenchyme, SL : subcutaneous lipoma, DR : dorsal root, IL : intramedullary lipoma, DREZ : dorsal root entry zone, D : dura, P-A : pia-arachnoid, M : muscle, LF : lumbodorsal fascia.
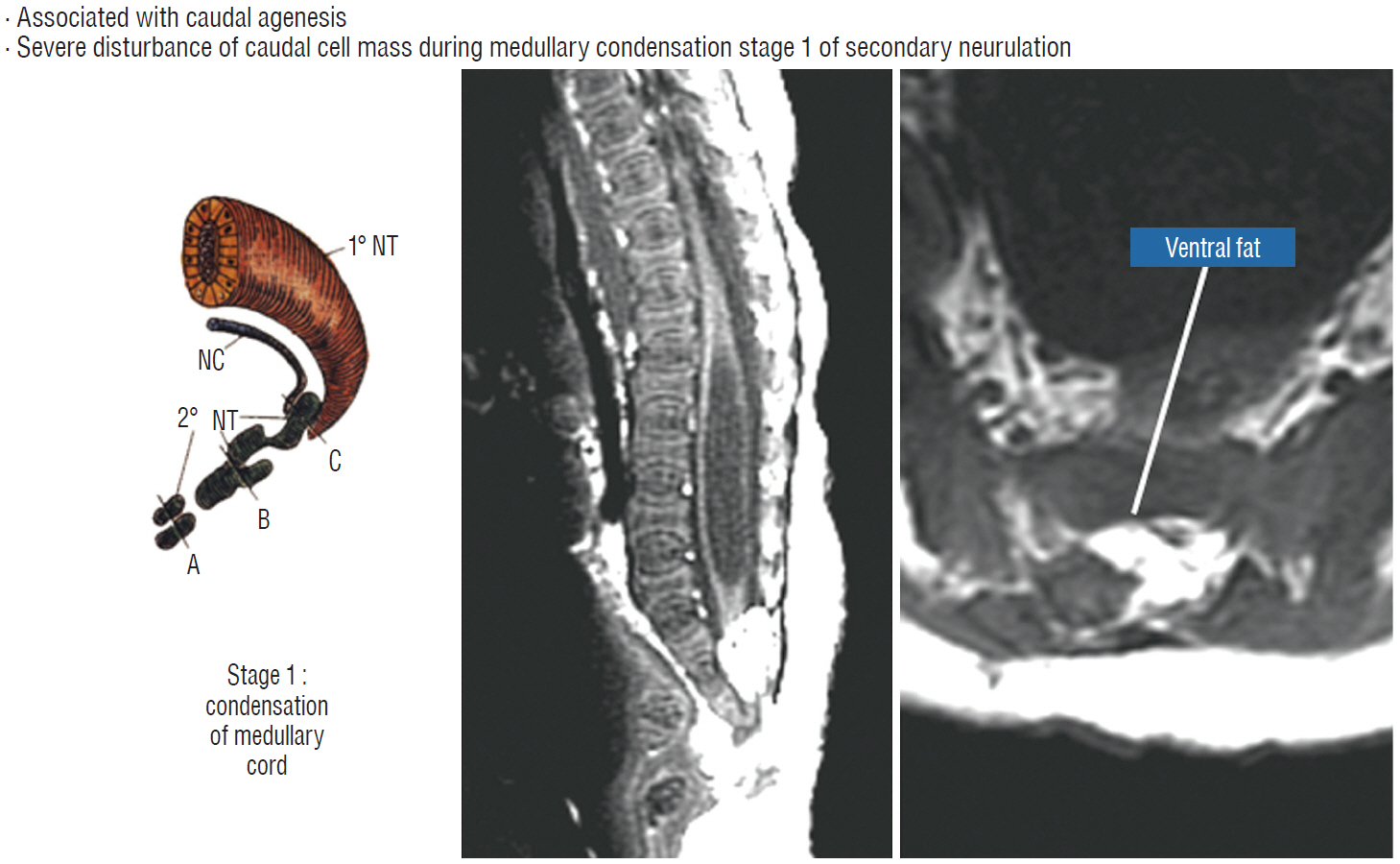
Fig. 7. Embryogenesis of chaotic lipomas. Left : basic error probably occurs with accelerated differentiation of lipogenic mesenchymal cells within the caudal cord during condensation stage (stage 1) of secondary neurulation and formation of the medullary cord, thereby incorporating fat tissue in the substance of the mature neural placode. Middle and right show dorsal and ventral fat and associated sacral agenesis. Reprinted from Pang et al. [61] with permission from Springer Nature. 1˚ NT : primary neural tube, 2˚ NT : secondary neural tube, NC : notochord.
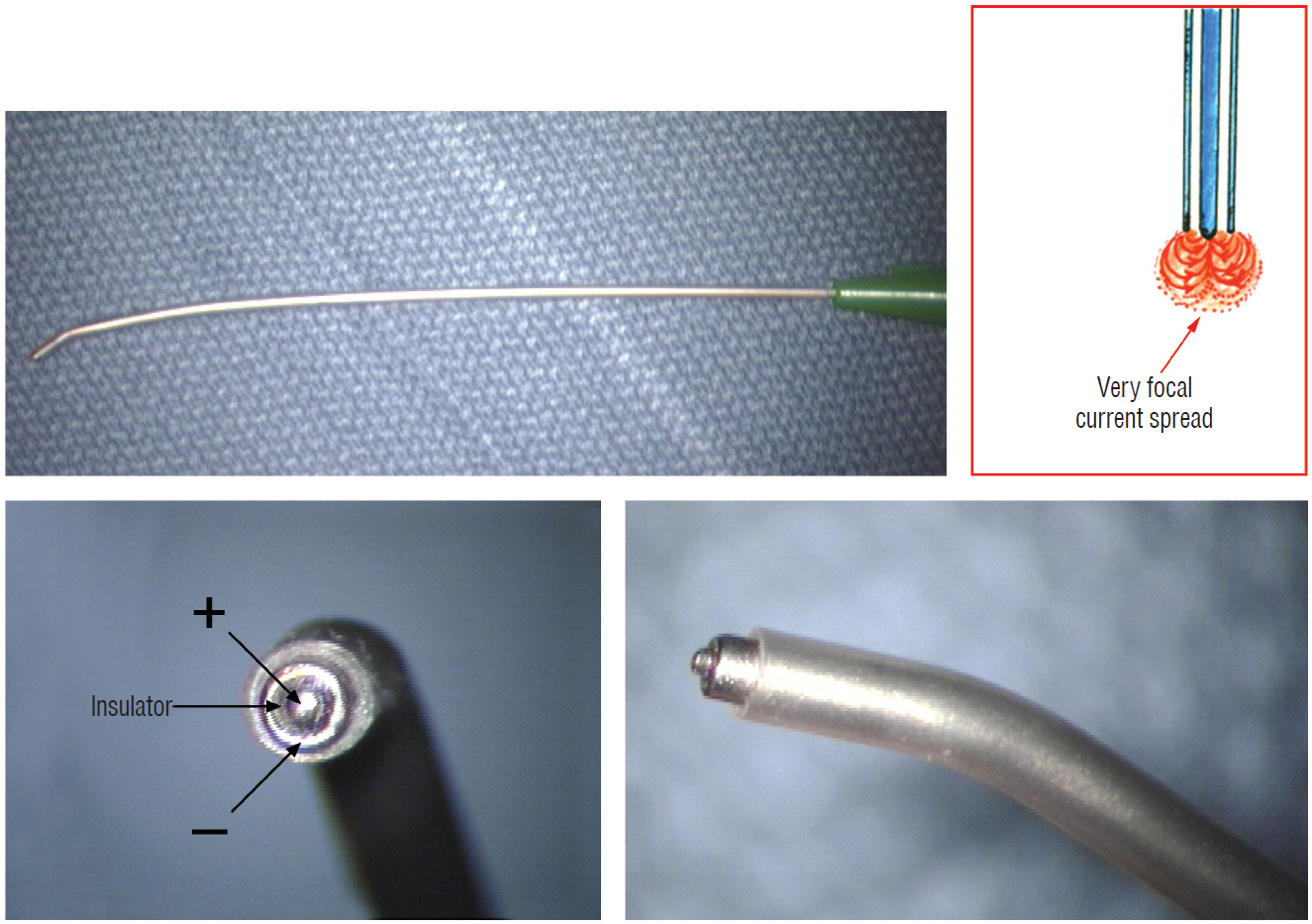
Fig. 8. Concentric coaxial bipolar microprobe stimulator in which the concentric cathode and anode are separated by a coaxial insulator. Tip diameter is approximately 1.75 mm. The microprobe delivers very focal current spread (Inset).
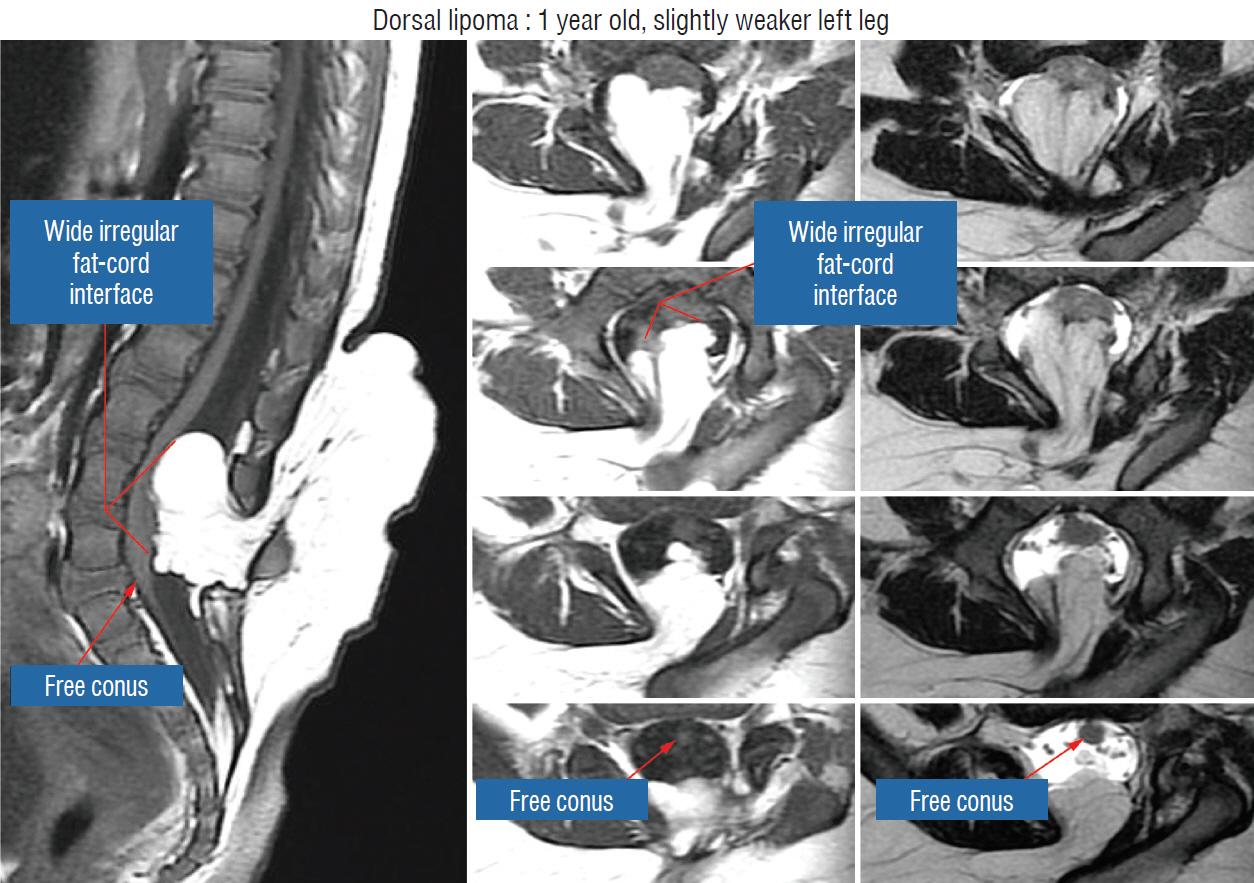
Fig. 9. Magnetic resonance imaging of a 12 months old girl with left leg weakness shows a large dorsal lipoma. The sagittal image shows a long stretch of lipomacord interface, but the conus is clearly free of fat. The axial images reveal the irregular nature of the lipoma-cord interface, but the neural placode is not excessively tilted to one side. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 10. Large extradural portion of the lipoma before dural opening. Note huge dural defect through which the extradural lipoma extends. Rostral exposure is to the right. Note the essential wide bony exposure. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 11. Drawing depicting the relationship between the lipoma, neural placode, nerve roots and dural sac in an axial slice. Upper : the lipoma-cord assembly is suspended at the dural edges at far lateral adhesion points like a hammock against side hinges. The dotted transverse line that joins the two side hinges divides the assembly into a dorsal disorderly, fibrofatty half that completely blocks the surgeon’s view to a much more orderly ventral half, containing the important anatomical landmarks of fusion line, DREZ, dorsal roots, fat-free ventral placode, and pristine ventral CSF space. Lower : after detaching the far lateral adhesion points (the hinges) by careful “crotch dissection”, and folding-in the fatty mass, the ventral anatomical landmarks can now be visualized. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society. DREZ : dorsal root entry zone, CSF : cerebrospinal fluid.
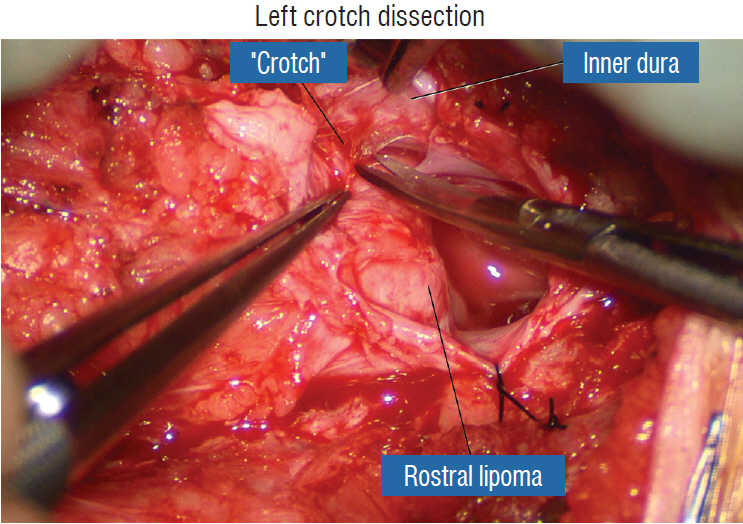
Fig. 12. Left crotch dissection in the large dorsal lipoma shown in Fig. 10. The lipoma is grasped firmly and pulled gently away from the adherent points on the inner dura, stretching the adhesion bands and thick arachnoid, creating the “crotch” and making the adhesions safe to be cut. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 13. Right crotch dissection. A : Cutting of the “crotch” on the right side as in Fig. 12. B : Lysing the crotch exposes the hidden nerve roots, the ventral neural placode, and the ventral free subarachnoid space. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 14. After crotch dissection on the right side and complete detachment of the lipoma (hammock) from the right inner dural lining, the fat-free ventral subarachnoid space, caudal nerve roots, and conus are well seen. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
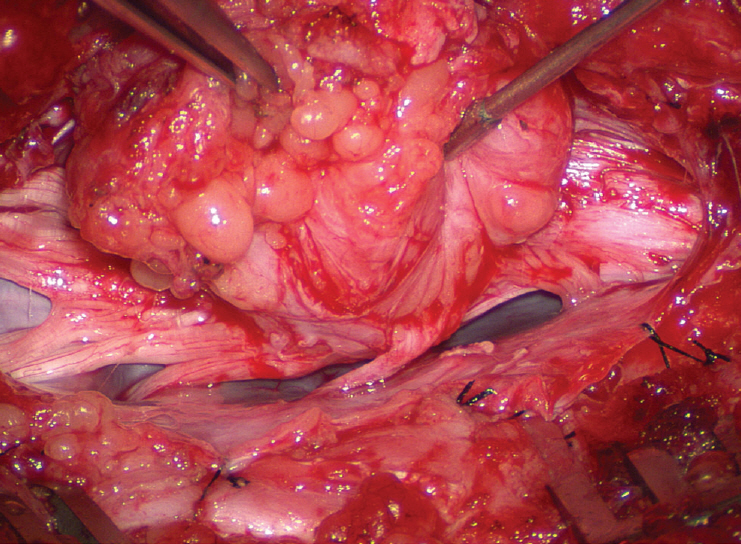
Fig. 15. Crotch dissection is complete on both sides. The entire right array of nerve roots are seen, but not the dorsal root entry zone or the fusion line, which are covered by the lateral overhang of the large lipoma. The entire hammock is now unsuspended from the dura. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
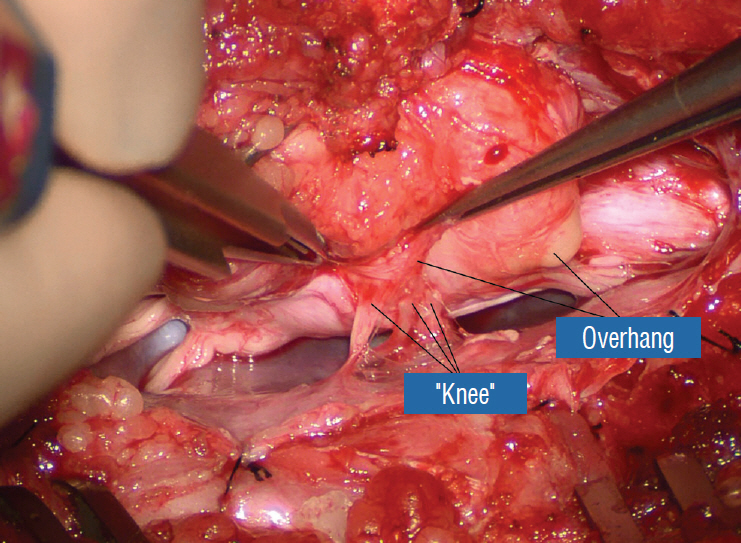
Fig. 16. The lateral overhang of the lipoma is well appreciated. Only the “knees” of the dorsal roots are seen. The “thighs”, or the most proximal portions of the roots, are hidden by and adherent to the overhanging fat. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
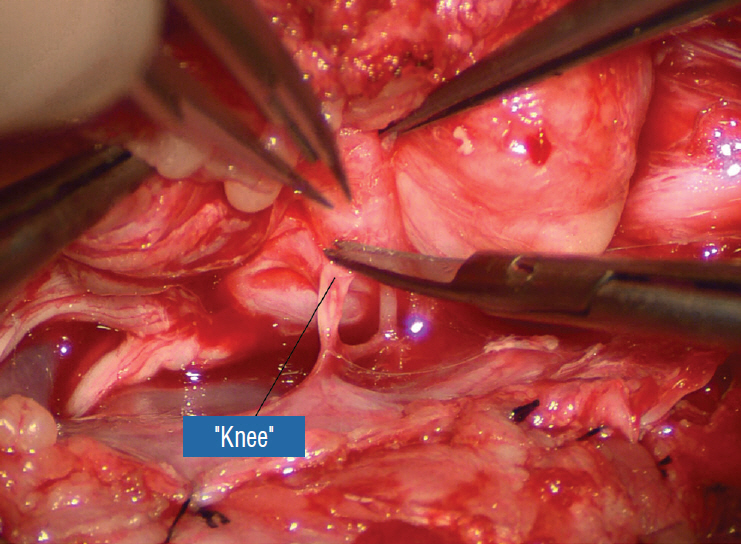
Fig. 17. “Knee dissection”: the adhesions covering the “thigh” of the dorsal roots are sharply taken down. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
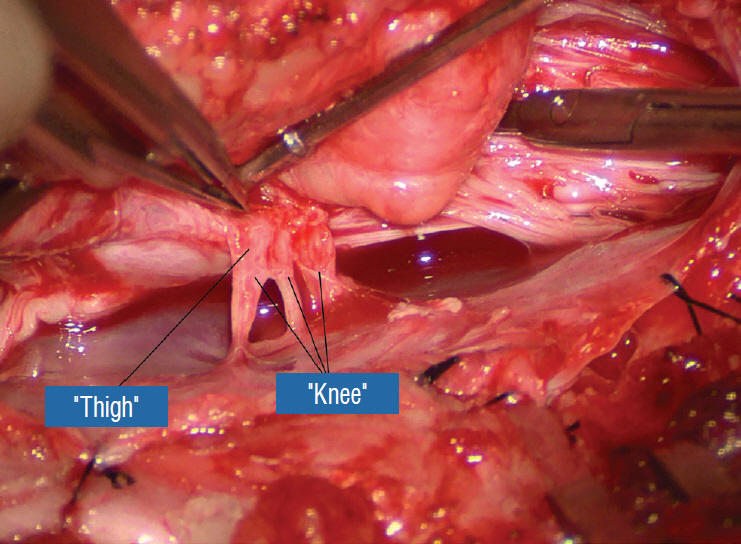
Fig. 18. After ridding the adhesions, the proximal “thigh” portions of the dorsal roots are exposed. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
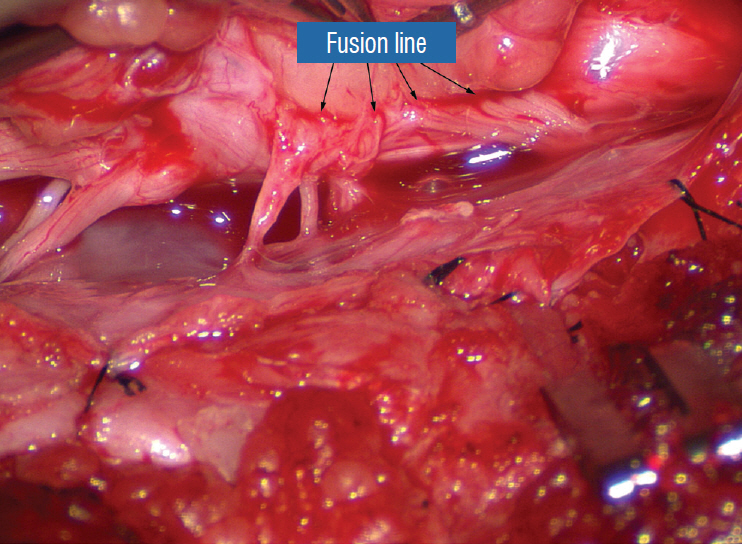
Fig. 19. The “true” fusion line on the right is revealed. Resection of lipoma on the lateral margin of the placode is now made safe. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
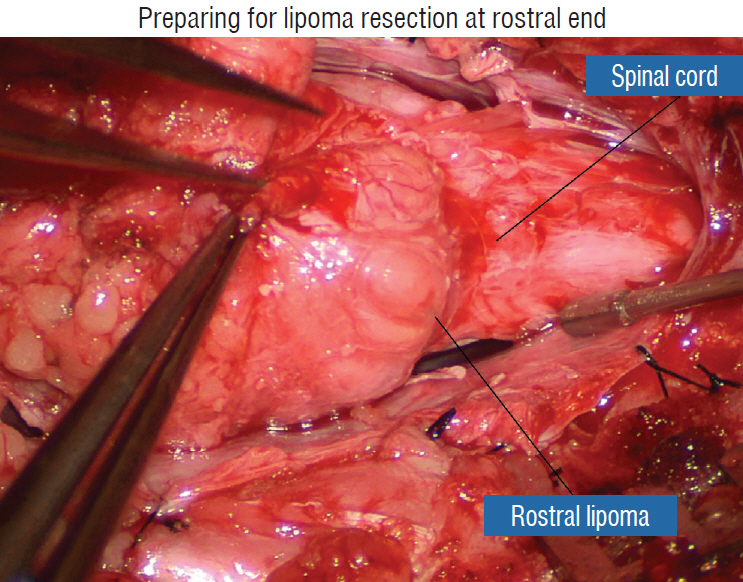
Fig. 20. Preparing for lipoma resection commencing on the rostral end of the fat where the lipoma-cord junction, the rostral dorsal roots, and beginning of the fusion lines are most distinct. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 21. Finding the white plane. A : Beginning resection at the rostral extremity of the lipoma. B : White plane located, which is a discrete though thin layer of whitish fibrous netting separating fat from spinal cord. C : Resection of lipoma along the right fusion line. Note the pial fringe, carefully preserved for neurulation. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
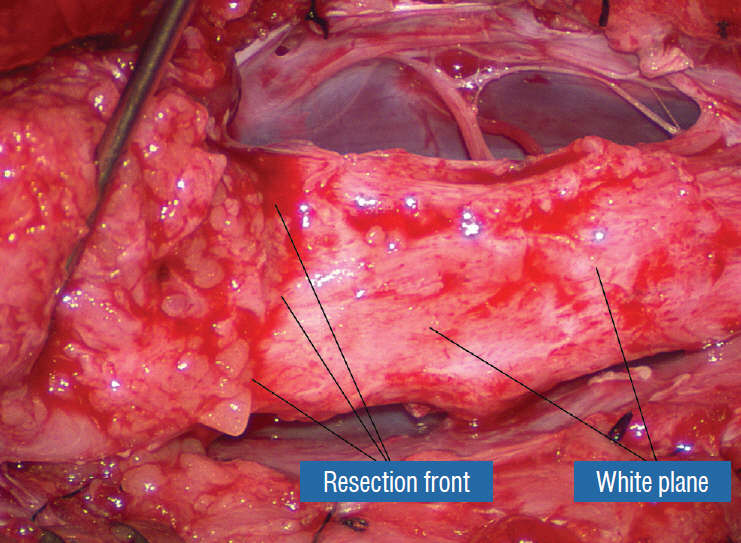
Fig. 22. The white plane, with the unresected portion of the lipoma on the left lifted up to show the resection front as a well defined transverse line across the body of the neural placode. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
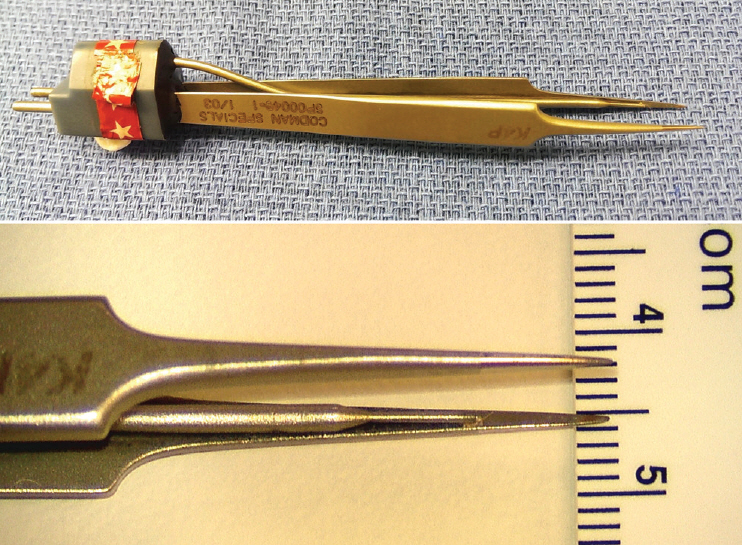
Fig. 23. Micro-irrigating bipolar cautery with super-fine tips measuring less than 0.2 mm. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 24. Lateral white plane dissection along the right fusion line is almost complete. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 25. Resection of the most caudal portion of the lipoma in the caudal to rostral direction, possible because this is a dorsal lipoma. The caudal white plane thus created will eventually merge with the proximal white plane resulting from the previous rostral-to-caudal dissection. A : Beginning white plane dissection from the conus side. B : More caudal white plane exposed. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
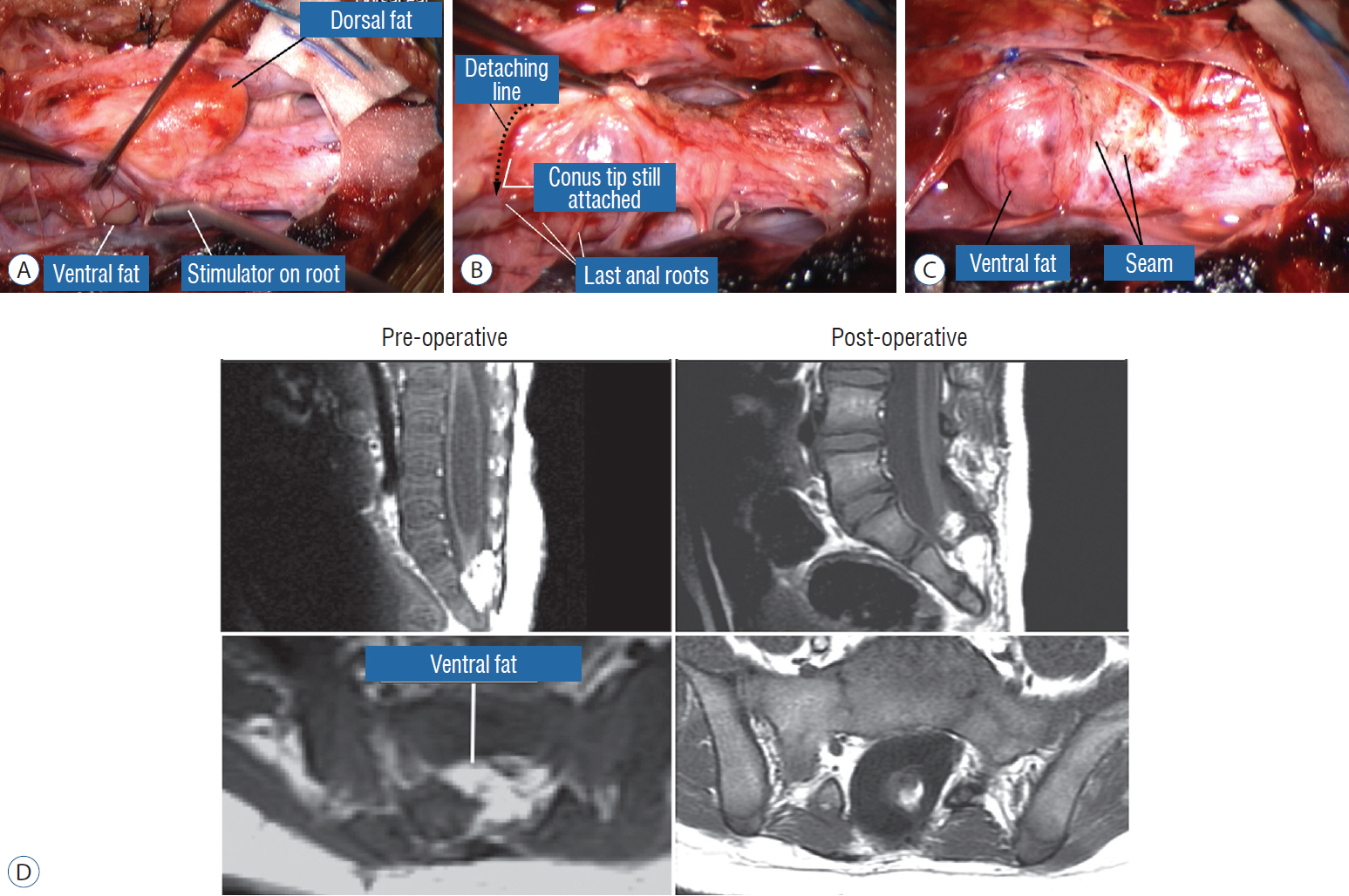
Fig. 26. Surgery for chaotic lipoma. A : Note ventral pia-covered fat medial to ventral nerve roots (being stimulated by concentric microprobe stimulator), and dorsal fat perched on the dorsal side of the placode. B : Terminal disconnection of neural placode from residual caudal lipoma stump after identification of 3 healthy pairs of anal sphincter motor roots. C : Caudal placode pulled up dorsally width-wise to be neurulated with the more proximal pial edge to form the seam, displaying the unviolated pia-covered ventral fat as a blunt stump. D : Pre- and postoperative magnetic resonance imaging shows residual fat on the detached cord stump. The cord is untethered, the thecal sac is augmented, and the syrinx has collapsed. A-C are reprinted from Pang [55] with permission from the Japanese Neurosurgical Society. D is reprinted from Pang et al. [61] with permission from Springer Nature.
Fig. 27. Continuing from Fig. 25B, the “naked” neural placode after complete resection of the dorsal lipoma. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
Fig. 28. Temporary small Weck Clips are applied to the apposed pial fringes to absorb the tissue torque tending to unfurl the dorsal bending of the placode. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 29. On pulling the pial fringes together to check the ease of the dorsal neurulation, considerable lateral tugging is felt on the right, due to the “short” nerve roots. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
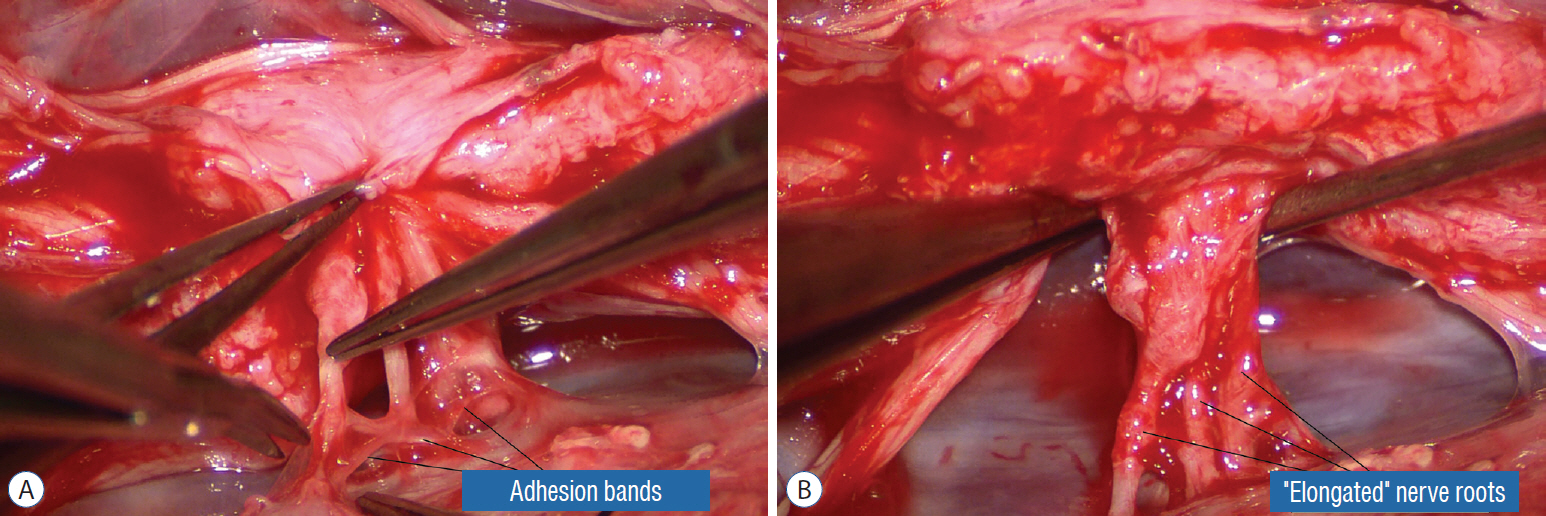
Fig. 30. Dealing with “short” nerve roots. A : The impression of shortness is spurious; these functional and supple roots appear short because they were bound tightly to the inner lining of the dura by adhesion bands that are being cut. B : After having been detached from the inner lining of the dura, these “short” nerve roots become magically “lengthened”. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 31. Pia-to-pia neurulation of the neural placode. A : Pia-to-pia suturing with 8-0 nylon sutures with knots buried. B : Tying of micro sutures, apposing the pial fringes from each side of the placode. C : Pia-to-pia neurulation completed with interrupted 8-0 nylon micro-sutures. The reconstituted neural tube is entirely piacovered, with an unobtrusive dorsal seam. Note intact conus. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 32. Dorsal lipoma with bulky pyramid placode – lesson learned. A : Note tall pyramid-shaped neural placode on axial MRI, with steep sides slopes interfacing with the lipoma. B : Lipoma stalk and dorsal lipoma. C : After lipoma resection, the placode is bulky in the middle and has thin pial fringes. D : Only the loose caudal part of the placode was neurulated. Rostral bulky part is left open because of TcMEP deterioration on forced attempts to suture. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society. MRI : magnetic resonance imaging, TcMEP : transcortical motor evoked potentials.
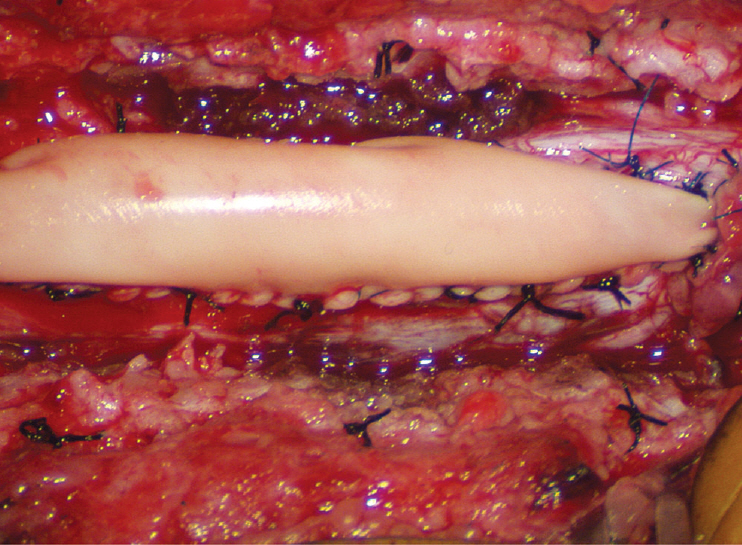
Fig. 33. Back to the dorsal lipoma in Fig. 31, after graft sutures are in place, water-tightness of the suture line is tested by several Valsalva manoeuvres. An optimal graft is one that does not leak, puffs up with expiration, and registers no inward folding, as this one. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 34. Pre- and post-operative magnetic resonance imaging of a case of transitional lipoma with no residual fat after total lipoma resection. Note neurulated oblong-shaped fat-free neural placode within a large dural sac. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
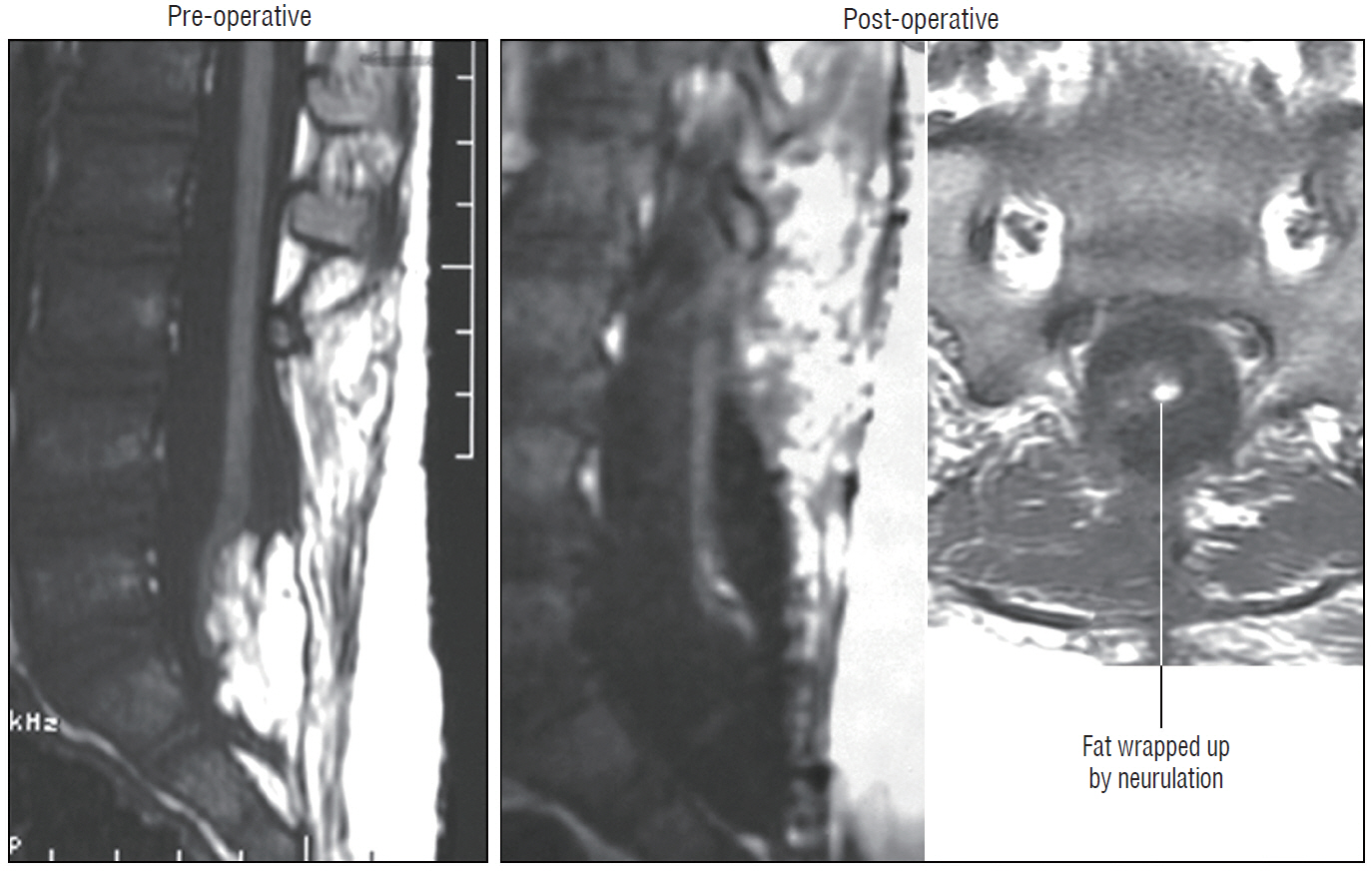
Fig. 35. Pre- and post-operative magnetic resonance imaging of a case of complex transitional lipoma with a very small amount (<20 mm3) of residual fat after resection. Axial image shows the small round piece of fat is wrapped up within the roundly neurulated neural placode and therefore not exposed on the surface. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
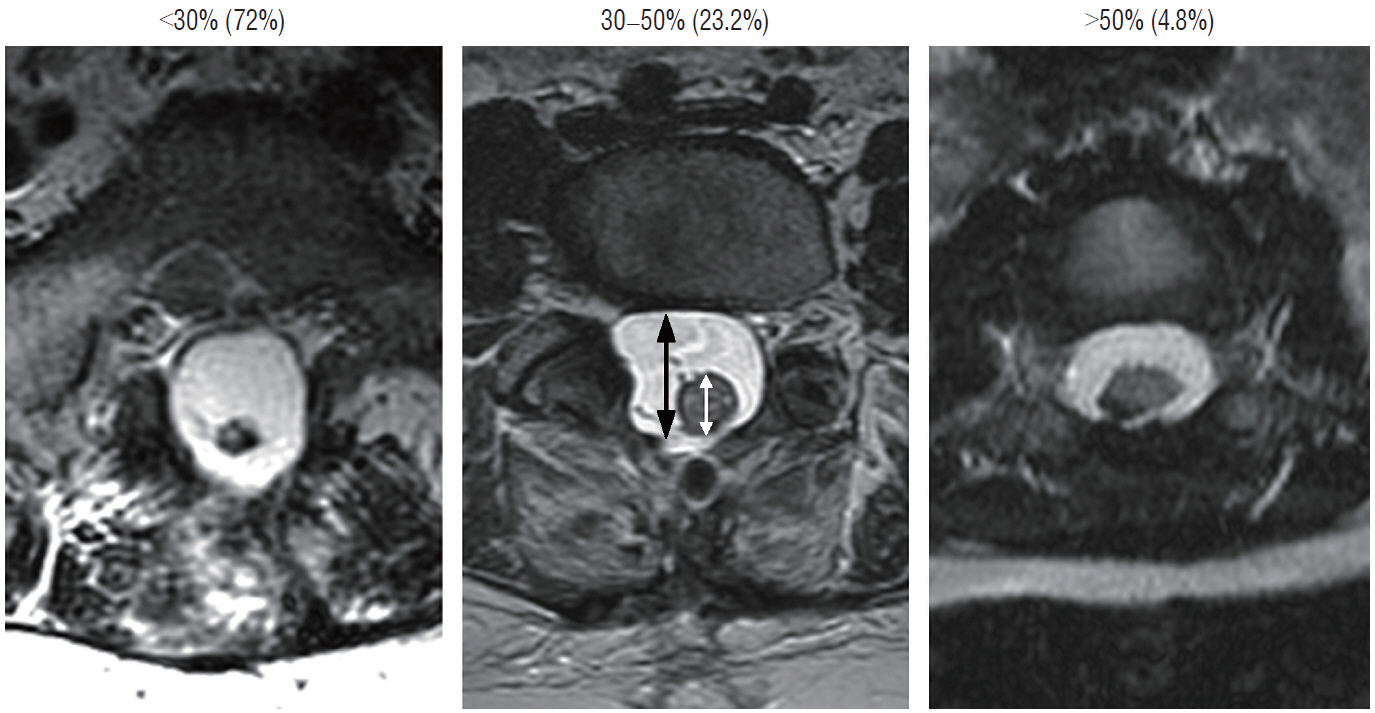
Fig. 36. Cord-sac ratios in the post-operative axial magnetic resonance imaging after total/near-total resection of lipoma. This ratio is obtained by dividing the sagittal diameter of the most bulbous portion of the post-neurulated neural placode (white arrow) by the sagittal diameter of the dural sac (black arrow). 72% in our series have very loose sacs with cord-sac ratios <30%; 23.2% have intermediate ratios 30–50%; and 4.8% have ratios >50% with the least commodious cordsac relationship. Cord-sac ratio estimates the degree of freedom of motion of the post-neurulated spinal cord within its container sac. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 37. Outcomes of total versus partial resection. Kaplan-Meier (KM) analysis for progression-free survival probability in total and partial resection of lipoma. The progression-free probability for total resection is 88.1% at 20 years, and 34.6% for partial resection at 10.5 years. The difference is highly significant (p<0.0001 by log-rank & Wilcoxon). Note stabilization of disease after 8 years with total resection, but inexorable deterioration without disease arrest with partial resection. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society. Pt : patients, Total : total resection, Partial : partial resection.
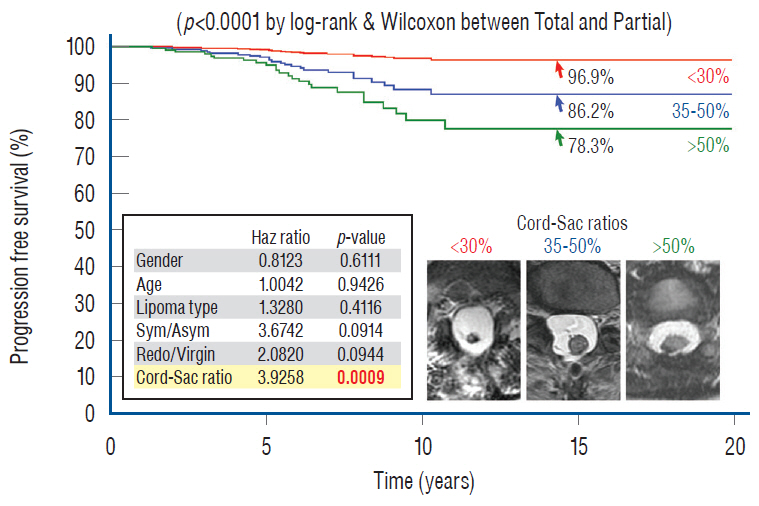
Fig. 38. Cox Multivariate Proportional Hazard Regression model analyzing the combined influence of six predictor variables (gender; age; lipoma type; symptoms; redo versus virgin; and cord-sac ratio) on PFS after total resection, featuring the resultant effect of the three cord-sac ratios of <30%, 30–50%, and >50%. The hazard ratios and p values for all six predictor variables are listed in the miniaturized table, showing that cord-sac ratio exerts the only significant independent influence on outcome. The respective progression-free probabilities, as indicated by the arrows, are 96.9% for low ratio, 86.2% for intermediate ratio, and 78.3% for high ratio. The differences in hazard prediction for the three ratios are highly significant (p=0.0009 in bold). <30%; 30–50%, and >50% indicate the three cord-sac ratios as shown in magnetic resonance imaging insets. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society. Sym/Asym : symptomatic versus asymptomatic lipomas.

Fig. 39. Cox Multivariate analysis for the influence of cord-sac ratios on outcome in 117 redo lipomas that underwent total resection. Progression-free probabilities are indicated by arrows. A high progression-free survival of 88.4% can still be managed even in redo lipomas if a cord-sac ratio <30% can be achieved, indicating the dominant role of cord-sac ratio, and conversely the subordinate role of other unidentified attributes of previous surgery, on long-term outcome (p=0.0214 between <30% and >50% cord-sac ratios). Reprinted from Pang et al. [61] with permission from Springer Nature. Pt : patients.

Fig. 40. Distribution of cord-sac ratios between the total resection and partial resection groups. Note 72% of patients who had total resection had cord-sac ratio <30%, versus less than 3% of patients who had partial resection. Conversely, only 6% of patients who had total resection had high ratio of >50%, versus over 90% of patients who had partial resection. The difference is significant (p=0.00026). <30%; 30–50%; and >50% indicate the cord-sac ratios. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.

Fig. 41. The pre- and post-operative sagittal and axial magnetic resonance imaging of a 10 years old girl who has had two previous partial resections of a large transitional lipoma, and who developed new leg weakness. The achieved post-operative cord-sac ratio is 20% (lower right); and she enjoyed long term progression-free status. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society.
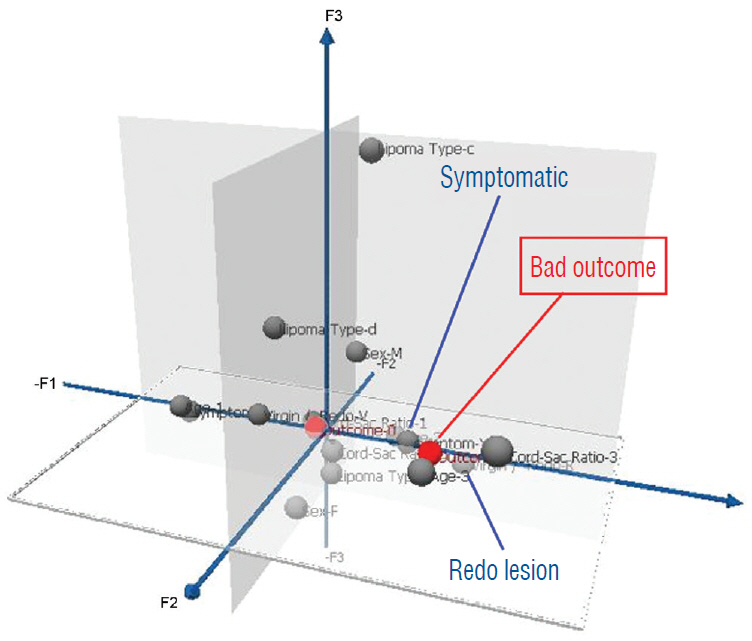
Fig. 42. Pre-operative profiling of good versus poor risk patients for total resection using three dimensional Multiple Correspondence Analysis plot, which displays the respective strength of influence of the six predictor variables (gender, age, lipoma type, symptoms, redo versus virgin lipomas, and cord-sac ratio) on outcome after total resection. The grey balls represent predictor variables and red balls represent outcomes. Only the statistically significant predictors are flagged. Bad outcome implies recurrence and good outcome the absence of recurrence during the follow-up period. Close clustering of variables (with flags) around an Outcome signifies strong influence; remote scattering of variables (without flags) from an outcome signifies weak influence. Bad outcome is associated with pre-operative symptoms and redo lesions. Reprinted from Pang et al. [61] with permission from Springer Nature.
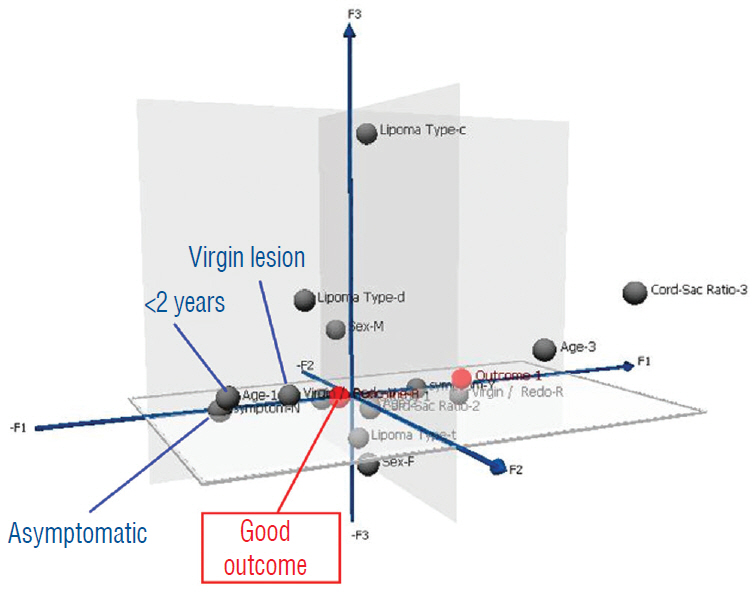
Fig. 43. Same pre-operative profiling as in Fig. 42 for good outcome, using the same Multiple Correspondence Analysis plot. Good outcome is associated with children less than 2 years, asymptomatic lesions, and virgin lipomas. Reprinted from Pang et al. [61] with permission from Springer Nature.

Fig. 44. Kaplan-Meier analysis for progression-free survival showing the predicted outcome of the 84 “ideal patients” who had had total resection; i.e., asymptomatic children younger than 2 years with virgin lipomas. The progression-free probability at 20 years is 99.2%, with disease stabilization after 5 years from surgery. Reprinted from Pang et al. [61] with permission from Springer Nature.

Fig. 45. Non-surgical treatment of asymptomatic lipomas. The blue line denotes the Paris series of 53 patients followed prospectively for 9 years [66], with a PFS of 67%. The yellow line denotes the retrospective London series of 56 patients followed for 10 years [68], with a PFS of 60%. In the London series, females, those with transitional lipomas and conus syrinx did worse, thus with an even worse PFS (dotted yellow line). Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society. Pt : patients, PFS : progression-free survival.
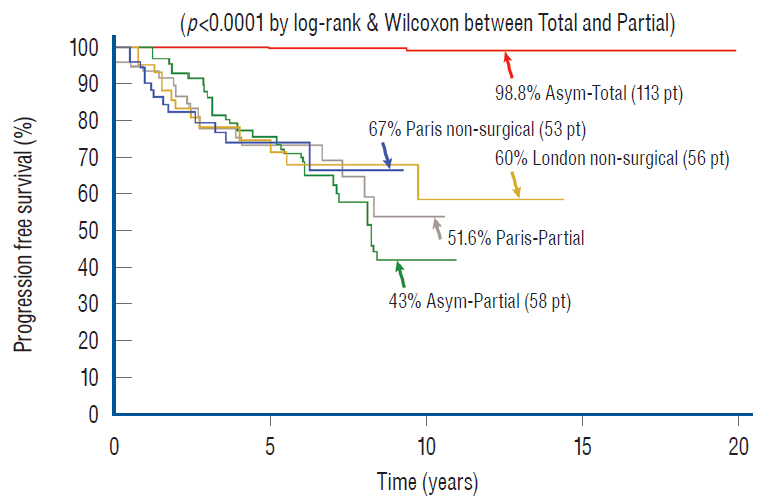
Fig. 46. Outcome differences between total resection, partial resection, and non-surgical management of asymptomatic virgin lipomas by Kaplan-Meier analysis. The non-surgical progressive-free survival graphs (“Paris non-surgical asym”) from the Parisian study [66] and from the London study [68] (“London non-surgical asym”) are inserted for visual comparison only and not meant to imply a true “head-to-head” comparison. Progression-free probability at 20 years for the 113 asymptomatic virgin lipomas that had undergone total resection is 98.8%, much better than 67% of the Parisian series or the 60% of the London series, and far superior to the 43.3% of our own partial resection series and the 51.6% of the Parisians’ own partial resection series. The difference between total and partial resection for asymptomatic virgin lipomas is highly significant (p<0.0001). The Paris partial resection and our own partial resection series are as labelled. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society. Pt : patients, Asym-Total : asymptomatic virgin lipomas treated by total resection, Asym-Partial : asymptomatic virgin lipomas treated by partial resection, Paris non-surgical : asymptomatic virgin lipomas managed non-surgically in Paris [66], London non-surgical asym : asymptomatic virgin lipomas from London [68].
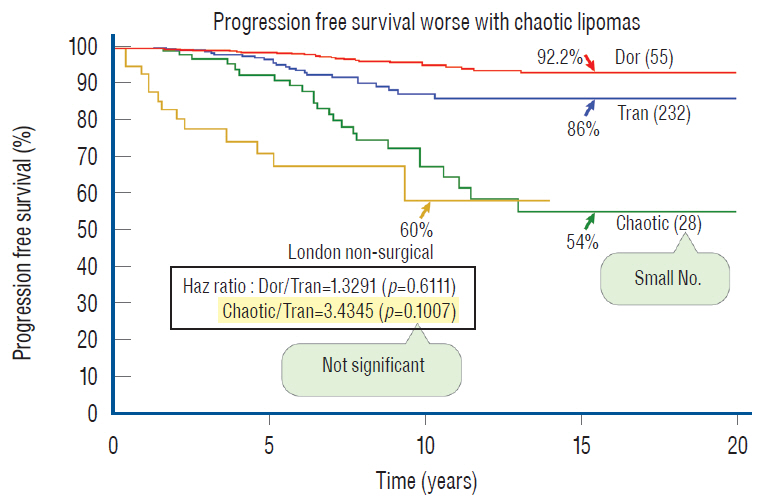
Fig. 47. The influence of lipoma type on outcome after total resection by KM analysis. The progression-free probabilities for the three lipoma types are indicated by arrows. There is no significant difference in outcome between dorsal and transitional lipomas (p=0.458 by log-rank and 0.904 by Wilcoxon) even after adjusting for sample size. The hazard ratio between chaotic and transitional lipomas is not statistically significant but that may be due to the small number in the chaotic group. The London non-surgical treatment progression-free survival curve [68] is now inserted on to the 3 PFS curves of the different lipoma types obtained with the Cox proportional hazards analysis. The 10 years PFS from the London series is very similar to the PFS of the chaotic lipomas, which raises the question whether there is merit in resecting asymptomatic chaotic lipomas. Reprinted from Pang [55] with permission from the Japanese Neurosurgical Society. KM : Kaplan-Meier, PFS : progression-free survival.

Fig. 48. Paired Cox Univariate (upper) and Multivariate (lower) analyses of the influence of pre-operative symptoms on PFS. The respective progression-free probabilities for asymptomatic and symptomatic lipomas are indicated by arrows, and their hazard ratios and relevant p values are listed for each Cox analysis. This shows the individual influence (expressed in univariate analysis) of pre-operative symptoms on outcome disappears when the influences of the other predictor variables are jointly considered (by multivariate analysis). Significant p values are in bold. Reprinted from Pang et al. [61] with permission from Springer Nature. Pt : patients, Asym : asymptomatic lipomas, Sym : symptomatic lipomas.
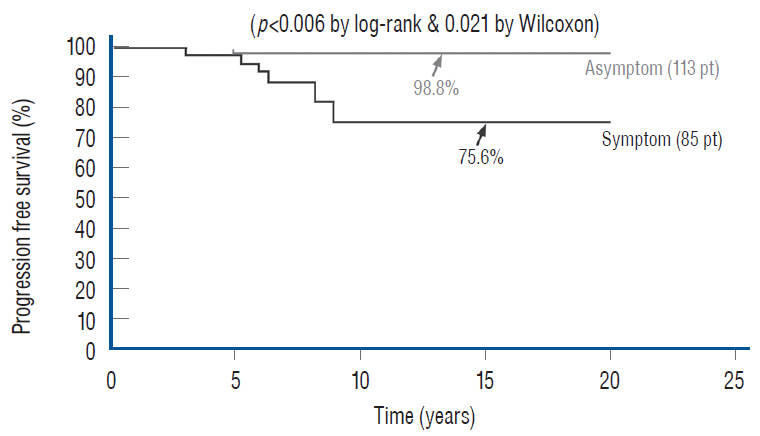
Fig. 49. The influence of pre-operative symptoms on outcome for virgin lipomas after total resection. Kaplan-Meier analysis for asymptomatic virgin and symptomatic virgin lipomas after total resection. Progression-free probability at 20 years for asymptomatic virgin lipomas is 98.8%, versus 75.6% for symptomatic virgin lipomas. The difference is significant (p=0.006 by log-rank and 0.021 by Wilcoxon). Reprinted from Pang et al. [61] with permission from Springer Nature. Pt : patients, Asymptom : asymptomatic virgin lipomas, Symptom : symptomatic virgin lipomas.
Reference
-
References
1. Arai H, Sato K, Wachi A. Surgical management in 81 patients with congenital intraspinal lipoma. Child Nerv Syst. 8:171. 1992.2. Atala A, Bauer SB, Dyro FM, Shefner J, Shillito J, Sathi S, et al. Bladder functional changes resulting from lipomyelomeningocele repair. J Urol. 148(2 Pt 2):592–594. 1992.
Article3. Barson AJ. The vertebral level of termination of the spinal cord during normal and abnormal development. J Anat. 106(Pt 3):489–497. 1970.4. Bruce DA, Schut L. Spinal lipomas in infancy and childhood. Childs Brain. 5:192–203. 1979.
Article5. Brunelle F, Sebag G, Baraton J, Carteret M, Martinat P, Pierre-Kahn A. Lumbar spinal cord motion measurement with phase-contrast MR imaging in normal children and in children with spinal lipomas. Pediatr Radiol. 26:265–270. 1996.
Article6. Byrne RW, Hayes EA, Georg TM, McLone DG. Operative resection of 100 spinal lipomas in infants less than 1 year of age. Pediatr Neurosurg. 23:182–186. discussion 186-187. 1995.
Article7. Caldarelli M, McLone DG, Colins JA, Suwa J, Knepper PA. Vitamin A induced neural tube defects in a mouse. Concepts Pediatr Neurosurg. 6:161–171. 1985.8. Chapman PH. Congenital intraspinal lipomas: anatomic considerations and surgical treatment. Childs Brain. 9:37–47. 1982.9. Chapman PH, Davis KR. Surgical treatment of spinal lipomas in childhood. Pediatr Neurosurg. 19:267–275. discussion 274. 1993.
Article10. Cochrane DD, Finley C, Kestle J, Steinbok P. The patterns of late deterioration in patients with transitional lipomyelomeningocele. Eur J Pediatr Surg 10 Suppl. 1:13–17. 2000.
Article11. Colak A, Pollack IF, Albright AL. Recurrent tethering: a common long-term problem after lipomyelomeningocele repair. Pediatr Neurosurg. 29:184–190. 1998.
Article12. Cornette L, Verpoorten C, Lagae L, Plets C, Van Calenbergh F, Casaer P. Closed spinal dysraphism: a review on diagnosis and treatment in infancy. Eur J Paediatr Neurol. 2:179–185. 1998.
Article13. Detwiler SR, Hotzer H. The inductive and formative influence of the spinal cord upon the vertebral column. Bull Hosp Joint Dis. 15:114–123. 1954.14. Dias M, Pang D. Human neural embryogenesis: a description of neural morphogenesis and a review of embryonic mechanisms. In : Pang D, editor. Disorders of the Pediatric Spine. New York: Raven Press;1994.15. Dick EA, de Bruhn R. Ultrasound of the spinal cord in children: its role. Eur Radiol. 13:552–562. 2003.
Article16. Dorward NL, Scatliff JH, Hayward RD. Congenital lumbosacral lipomas: pitfalls in analysing the results of prophylactic surgery. Childs Nerv Syst. 18:326–332. 2002.
Article17. Hamilton HL, Boyd JD, Mossman HM. Human Embryology. ed 4. Baltimore: Williams & Wilkins;1972.18. Hoffman HJ, Hendrick EB, Humphreys RP. The tethered spinal cord: its protean manifestations, diagnosis and surgical correction. Childs Brain. 2:145–155. 1976.
Article19. Hoffman HJ, Taecholarn C, Hendrick EB, Humphreys RP. Management of lipomyelomeningoceles. Experience at the Hospital for Sick Children, Toronto. J Neurosurg. 62:1–8. 1985.20. James CC, Lassman LP. Diastematomyelia and the tight filum terminale. J Neurol Sci. 10:193–196. 1970.
Article21. James HE, Canty TG. Human tails and associated spinal anomalies. Clin Pediatr (Phila). 34:286–288. 1995.
Article22. James HE, Williams J, Brock W, Kaplan GW, U HS. Radical removal of lipomas of the conus and cauda equina with laser microneurosurgery. Neurosurgery. 13:340–345. 1984.
Article23. Jones PH, Love JG. Tight filum terminale. AMA Arch Surg. 73:556–566. 1956.
Article24. Källén B. Early embryogenesis of the central nervous system with special reference to closure defects. Dev Med Child Neurol. 10(Suppl 6):44–53. 1968.25. Kanev PM, Lemire RJ, Loeser JD, Berger MS. Management and long-term follow-up review of children with lipomyelomeningocele, 1952-1987. J Neurosurg. 74:48–52. 1990.
Article26. Koyanagi I, Iwasaki Y, Hida K, Abe H, Isu T, Akino M. Surgical treatment supposed natural history of the tethered cord with occult spinal dysraphism. Childs Nerv Syst. 13:268–274. 1997.
Article27. Kulkarni AV, Pierre-Kahn A, Zerah M. Conservative Management of asymptomatic spinal lipomas of the conus. Neurosurgery. 54:868–873. discussion 873-875. 2004.
Article28. Kunitomo K. The development and reduction of the tail and of the caudal end of the spinal cord. Carnegie Contr Embryol. 8:161–203. 1918.29. La Marca F, Grant JA, Tomita T, McLone DG. Spinal lipomas in children: Outcome of 270 procedures. Pediatr Neurosurg. 26:8–16. 1997.
Article30. Marin-Padilla M. Clinical and experimental rachischisis. In : Vinken PS, Bruyn GW, editors. Handbook of clinical neurology. Amsterdam: North-Holland;1978. 32:p. 159–191.31. Marin-Padilla M. Mesodermal alterations induced by hypervitaminosis A. J Embryol Exp Morphol. 15:261–269. 1966.
Article32. Marin-Padilla M. Morphogenesis of anencephaly and related malformations in Current topics in pathology. Heidelberg: Springer;1921. p. 145–174.33. Marin-Padilla M. Morphogenesis of experimental encephalocele (Cranioschisis occulta). J Neurol Sci. 46:83–99. 1980.
Article34. Marin-Padilla M. Notochordal-basichondrocranium relationships: abnormalities in experimental axial skeletal (dysraphic) disorders. J Embryol Exp Morphol. 53:15–38. 1979.
Article35. Marin-Padilla M. The tethered cord syndrome: developmental considerations. In : Holtzmann RNN, Stein BM, editors. The tethered spinal cord. New York: Thieme;1985. p. 3–13.36. Marin-Padilla M, Marin-Padilla TM. Morphogenesis of experimentally induced Arnold--Chiari malformation. J Neurol Sci. 50:29–55. 1981.
Article37. McGuire EJ, Woodside JR, Borden TA, Weiss RM. Prognostic value of urodynamic testing in myelodysplastic patients. J Urol. 126:205–209. 1981.
Article38. McGuire EJ. The innervation and function of the lower urinary tract. J Neurosurg. 65:278–285. 1986.
Article39. McLone DG, Knepper PA. Role of complex carbohydrates and neurulation. Pediatr Neurosci. 1(2-9):1985–1986.
Article40. McLone DG, Mutluer S, Naidich TP. Lipomeningoceles of the conus medullaris. In : Karger S, editor. Concepts in Pediatric Neurosurgery. Basel: Karger;1982. p. 171–177.41. McLone DG, Naidich TP. Laser resection of fifty spinal lipomas. Neurosurgery. 18:611–615. 1986.
Article42. McLone DG, Naidich TP. Spinal dysraphism: Experimental and clinical. In : Holtzman RN, Stein BM, editors. The Tethered Spinal Cord. New York: Thieme-Stratton;1985.43. McLone DG, Suwa J, Collins JA, Poznaski S, Knepper PA. Neurulation: biochemical and morphological studies on primary and secondary neural tube defects. Concepts Pediatr Neurosurg. 4:15–29. 1983.44. Morriss-Kay GM, Crutch B. Culture of rat embryos with beta-D-xyloside: evidence of a role for proteoglycans in neurulation. J Anat. 134(Pt 3):491–506. 1982.45. Müller F, O’Rahilly R. The development of the human brain, the closure of the caudal neuropore, and the beginning of secondary neurulation at Stage 12. Anat Embryol (Berl). 176:413–430. 1987.
Article46. O’Rahilly R, Meyer DB. The timing and sequence of events in the development of the human vertebral column during the embryonic period proper. Anat Embryol (Berl). 157:167–176. 1979.
Article47. O’Shea KS, Kaufman MH. Phospholipase C-induced neural tube defects in the mouse embryo. Experientia. 36:1217–1219. 1980.
Article48. Pang D. Commentary to the article: asymptomatic lumbosacral lipomas- -a natural history study, by Wykes V, Desai D, and Thompson DNP. Childs Nerv Syst. 28:1741–1742. 2012.
Article49. Pang D. Electrophysiological monitoring for tethered cord surgery. In : Yamada S, editor. Tethered cord syndrome. ed 2. New York: Thieme Medical Publishers;2010. p. 199–209.50. Pang D. Intraoperative neurophysiology of the conus medullaris and cauda equina. Childs Nerv Syst. 26:411–412. 2010.
Article51. Pang D. Spinal Cord Lipoma. In : Batjer H, Loftus C, editors. Textbook of Neurological Surgery. New Jersey: Lippincott, Williams and Wilkins;2002.52. Pang D. Spinal Cord Lipomas. In : Pang D, editor. Disorders of the Pediatric Spine. New York: Raven Press;1995. p. 175–201.53. Pang D. Surgical management of complex spinal cord lipomas: how, why, and when to operate. A review. J Neurosurg Pediatr. 23:537–556. 2019.
Article54. Pang D. Tethered Cord Syndrome. In : Hoffman HJ, editor. Advances in Pediatric Neurosurgery. Philadelphia: Hanley and Belfus, Inc;1986. p. 45–79.55. Pang D. Total resection of complex spinal cord lipomas: how, why, and when to operate? Neurol Med Chir (Tokyo). 55:695–721. 2015.
Article56. Pang D, Casey K. Use of an anal sphincter pressure monitor during operations on the sacral spinal cord and nerve roots. Neurosurgery. 13:562–568. 1983.
Article57. Pang D, Wilberger JE Jr. Tethered cord syndrome in adults. J Neurosurg. 57:32–47. 1982.
Article58. Pang D, Zovickian J, Moes GS. Retained medullary cord in humans: late arrest of secondary neurulation. Neurosurgery. 68:1500–1519. discussion 1519. 2011.
Article59. Pang D, Zovickian J, Oviedo A. Long-term outcome of total and near-total resection of spinal cord lipomas and radical reconstruction of the neural placode: part I-surgical technique. Neurosurgery. 65:511–528. discussion 528-529. 2009.60. Pang D, Zovickian J, Oviedo A. Long-term outcome of total and near-total resection of spinal cord lipomas and radical reconstruction of the neural placode, part II: outcome analysis and preoperative profiling. Neurosurgery. 66:253–272. discussion 272-273. 2010.61. Pang D, Zovickian J, Wong ST, Hou YJ, Moes GS. Surgical treatment of complex spinal cord lipomas. Childs Nerv Syst. 29:1485–1513. 2013.
Article62. Pierre-Kahn A, Lacombe J, Pichon J, Giudicelli Y, Renier D, Sainte-Rose C, et al. Intraspinal lipomas with spina bifida. Prognosis and treatment in 73 cases. J Neurosurg. 65:756–761. 1986.63. Pierre-Kahn A, Zerah M, Renier D, Cinalli G, Sainte-Rose C, Lellouch-Tubiana A, et al. Congenital lumbosacral lipomas. Childs Nerv Syst. 13:298–334. discussion 335. 1997.
Article64. Sathi S, Madsen JR, Bauer S, Scott RM. Effect of surgical repair on the neurologic function in infants with lipomeningocele. Pediatr Neurosurg. 19:256–259. 1993.
Article65. Schoenwolf GC. Histological and ultrastructural observations of tail bud formation in the chick embryo. Anat Rec. 193:131–147. 1979.
Article66. Schoenwolf GC. Histological and ultrastructural studies of secondary neurulation in mouse embryos. Am J Anat. 169:361–376. 1984.
Article67. Schut L, Bruce DA, Sutton LN. The management of the child with a lipomyelomeningocele. Child Neurosurg. 30:464–476. 1983.
Article68. Stolke D, Zumkeller M, Seifert V. Intraspinal lipomas in infancy and childhood causing a tethered cord syndrome. Neurosurg Rev. 11:59–65. 1988.
Article69. Streeter GL. Factors involved in the formation of the filum terminale. Am J Anat. 25:1–11. 1919.
Article70. Sutton LN. Lipomyelomeningocele. Neurosurg Clin N Am. 6:325–338. 1995.
Article71. Talwalker VC, Datsur DK. Ectopic spinal cord myelomeningocele with tethering: a clinicopathological entity. Dev Med Child Neurol. 16(Suppl 32):159–160. 1974.72. Toole BP. Glycosaminoglycans in morphogenesis. In : Hay E, editor. Cell Biology of Extracellular Matrix. New York: Plenum Press;1981. p. 229–294.73. Wykes V, Desai D, Thompson DN. Asymptomatic lumbosacral lipomas- -a natural history study. Childs Nerv Syst. 28:1731–1739. 2012.
Article74. Xenos C, Sgouros S, Walsh R, Hockley A. Spinal lipomas in children. Pediatr Neurosurg. 32:295–307. 2000.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intramedullary Spinal Cord Lipoma without Spinal Dysraphism
- Long Term Outcome of Non-Dysraphic Intramedullary Spinal Cord Lipomas in Adults: Case Series and Review
- Spinal Intramedullary Lipoma without Dysraphism
- A Case of Intradural Spinal Lipoma
- Perspectives on Spinal Dysraphism : Past, Present, and Future
